

Abstract
Recurrent patellar instability can be very debilitating and may require surgical intervention. A thorough workup must be completed in this subset of patients. Risk factors for recurrent instability include patella alta, trochlear dysplasia, an increased tibial tubercle–trochlear groove distance, and insufficiencies in the medial retinacular structures. Necessary treatment of these risk factors, once identified, should be addressed surgically. Patellofemoral reconstruction must be individually tailored to each patient's anatomy and may necessitate medial patellofemoral ligament reconstruction, tibial tubercle osteotomy, or trochleoplasty in any combination or as a standalone procedure. This article details our technique for surgical treatment of recurrent patellar instability with a medial patellofemoral ligament reconstruction, an open trochleoplasty, and a tibial tubercle osteotomy for patients with severe trochlear dysplasia, an increased tibial tubercle–trochlear groove distance, or patella alta.
Primary patellar dislocations occur in a small percentage of individuals, and only 17% of these patients have a recurrent dislocation.1 However, after a second dislocation, the chance of additional dislocations increases to approximately 50%.1 Whereas primary dislocations can be treated with a brace, surgical treatment is essential for patients who have recurrent patellofemoral dislocations because symptoms often do not resolve.2 Risk factors for chronic patellar instability include patella alta, trochlear dysplasia, an increased tibial tubercle–trochlear groove (TT-TG) distance, and insufficiencies in the medial retinacular structures.3 The purpose of this article is to describe our technique for treating recurrent patellar instability with medial patellofemoral ligament (MPFL) reconstruction, an open trochleoplasty in patients with severe trochlear dysplasia, and a tibial tubercle osteotomy (TTO) in patients with an increased TT-TG distance or patella alta.
Technique
Objective Diagnosis
Lateral radiographs are useful to assess abnormal trochlear morphology and to categorize the joint according to the Dejour classification4 (Fig 1). Lateral radiographs are also useful to assess patella alta by calculating the Insall-Salvati, modified Insall-Salvati, Blackburne-Peel, and Caton-Deschamps ratios. The Caton-Deschamps index is the preferred method because of its accuracy and ability to remain unaffected by the degree of knee flexion.5 In addition, axial radiographs with the knee in 30° of flexion enable assessment of the sulcus angle and the depth of the trochlear groove.6 A sulcus angle of 145° or greater indicates a dysplastic trochlea.4 Lateral and medial trochlear inclination can be helpful in assessing dysplasia severity. Trochlear dysplasia is best characterized by use of a combination of quantitative radiographic measurements and the Dejour classification system.2
Fig 1.

Dejour classification system for trochlear dysplasia represented by lateral radiographic views and axial cross sections. (A) In type A dysplasia, the trochlea is shallow but still symmetrical and concave, with the crossing sign on the lateral radiograph. (B) In type B dysplasia, the trochlea is flat or convex, with the crossing sign and a trochlear spur on the lateral radiograph. (C) In type C dysplasia, the lateral facet is convex and the medial facet is hypoplastic, with the crossing sign and double contour sign (subchondral sclerosis of the medial hypoplastic facet) on the lateral radiograph. (D) In type D dysplasia, the cliff pattern is present on the axial view; the crossing sign, a supratrochlear spur, and the double contour sign can all be seen on the lateral radiograph. Reprinted with permission.2
In addition, magnetic resonance imaging (MRI) is helpful to evaluate articular cartilage status and identify soft-tissue damage, particularly MPFL injury. MRI is also used to measure lateral trochlear inclination.7 Furthermore, lateral radiographs generally underestimate lateral inclination compared with MRI.2
Preoperative computed tomography (CT) is helpful for measuring the TT-TG distance. A TT-TG distance greater than 20 mm on CT scans is considered pathologic and is a substantial risk factor for patellar instability.4 These patients may be candidates for a medializing tubercle transfer.
Indications for Surgery
Whereas primary patellar dislocations should be treated nonoperatively in a brace, chronic dislocations should be treated surgically.8 Patients with Dejour type A trochlear dysplasia (Fig 1) should undergo an MPFL reconstruction rather than a trochleoplasty, and patients with Dejour type B, C, or D dysplasia should be evaluated regarding a possible sulcus-deepening trochleoplasty in addition to MPFL reconstruction2, 9 (Table 1). The MPFL has been reported to provide up to 60% of resistance to lateral displacement of the patella.10 As a result, an MPFL reconstruction should be performed in conjunction with any trochleoplasty procedure.2
Table 1.
Indications and Contraindications for Trochleoplasty
| Indications |
| Recurrent patellar dislocations |
| Dejour type B, C, or D trochlear dysplasia |
| Contraindications |
| Open physes |
| Diffuse patellofemoral arthritis |
A trochleoplasty is contraindicated in patients with open physes. For these patients, an MPFL reconstruction should be proposed as a safe surgical alternative. A trochleoplasty is also contraindicated in patients with diffuse patellofemoral arthritis because of a significant risk of increasing pain levels.2
Patients with patella alta or a TT-TG distance greater than 20 mm (on CT scans) may require a TTO (Table 2). The TT-TG distance is the most reliable diagnostic method to indicate the need for a TTO. This method has been validated for CT scans by a recent study that reported a systematic bias toward lower TT-TG distances on MRI compared with CT scans.11 A distalization of the tubercle is recommended for patients with patella alta. The senior author (R.F.L.) routinely uses a Caton-Deschamps index greater than 1.4 to define patella alta. Of note, some degree of medialization should be expected with tuberosity distalization.12 For patients with a TT-TG measurement greater than 20 mm, a medialization of the tubercle is recommended to reduce contact pressures on the lateral trochlear and patellar facets.2 Contraindications for TTO include open physes, advanced patellofemoral arthritis, patella baja, knee pain or instability that does not have a rational biomechanical or articular cartilage basis, and localized or systematic inflammatory disease.13
Table 2.
Indications and Contraindications for Tibial Tubercle Osteotomy
| Indications |
| Recurrent lateral patellar dislocations∗ |
| TT-TG distance >20 mm |
| Patella alta |
| Contraindications |
| Open physes |
| Advanced patellofemoral arthritis |
| Patella baja |
| Knee pain or instability that does not have a rational biomechanical or articular cartilage basis |
| Localized or systematic inflammatory disease |
TT-TG, tubercle–trochlear groove.
Medial patellofemoral ligament reconstruction is indicated in all surgical candidates with recurrent patellar dislocations.
Patellofemoral reconstruction actually comprises a spectrum of procedures that must be individually tailored to each patient's necessities. This list of possible procedures to address patellofemoral instability is what is referred to by the French school as the menu à la carte.14 Surgical strategies may include MPFL reconstruction, TTO, or trochleoplasty in any combination or as a standalone procedure. In this article we present a complex patient who met the indications for all 3 procedures.
Patient Positioning and Anesthesia
The patient undergoes induction of general anesthesia and is positioned supine on the operating table. A well-padded high-thigh tourniquet is placed on the operative leg, and a bilateral comparative examination under anesthesia is performed to confirm the preoperative diagnosis and to better evaluate patellar translation abnormalities. A sterile bump should be placed under the knee to maintain 20° of flexion.
Surgical Technique
An anterior midline incision is performed followed by medial and lateral subcutaneous dissection to create soft-tissue flaps (Video 1). The MPFL attachment on the patella is then identified, which is approximately 41% from the proximal pole, and an anterior cruciate ligament guide (Arthrex, Naples, FL) is used to place a guide pin transversely across the patella. Using the aiming guide helps prevent inadvertent piercing of the patellar cartilage surface. A 4.5-mm cannulated EndoButton reamer (Smith & Nephew, Andover, MA) is used to create a complete tunnel to allow the passage of a cortical fixation device (EndoButton; Smith & Nephew); a 5-mm EndoButton reamer (Smith & Nephew) is then used to create an 8- to 10-mm-deep socket for the graft. The total length of the tunnel is measured to select the appropriate fixation device size. The course of the MPFL is followed along the distal edge of the vastus medialis obliquus with sharp dissection medially. With the adductor magnus tendon used as a landmark, the adductor tubercle and medial epicondyle are identified. The femoral attachment of the MPFL is located at a point 1.9 mm anterior and 3.8 mm distal to the adductor tubercle (Fig 2), and two suture anchors (SuperAnchor; Mitek, Westwood, MA) are placed in this location.15
Fig 2.
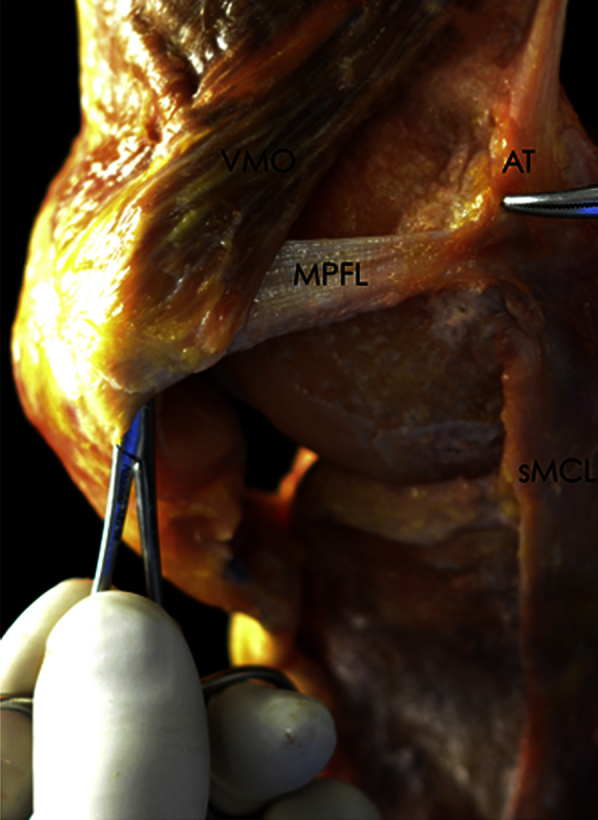
Cadaveric photograph of a right knee showing the relation of the patella, vastus medialis obliquus (VMO), and adductor tubercle (AT) relative to the medial patellofemoral ligament (MPFL). A needle holder is under the MPFL, and the scissors are pointing to the femoral insertion of the MPFL. (sMCL, superficial medial collateral ligament.)
Next, the semitendinosus graft is harvested for the MPFL reconstruction. Once identified within the pes anserine bursa and released of all adhesions with the help of a Cobb elevator, the semitendinosus is harvested with an open tendon stripper (Arthrex) and sharply detached from the distal tibial insertion. The graft is then looped around a cortical fixation device and undergoes tubularization on the back table with a nonabsorbable No. 2 FiberWire whipstitch suture (Arthrex). The graft should have a minimum length of 16 cm.
Attention is then turned to the tibial tubercle in preparation for the osteotomy. First, a scalpel is used to elevate the periosteum off the medial and lateral aspects of the tibial tubercle in a proximal-to-distal fashion. The most proximal attachment of the patellar tendon is identified. A distance of 30 mm is measured distally from this location and marked with cautery. It is important that the bone block is 30 mm in length and thick enough to include cancellous bone and to prevent breakage. Once this is confirmed, a 2-mm drill (Synthes, West Chester, PA) is used to create multiple holes along the medial and lateral borders of the osteotomy. The surgeon then releases the medial border of the tubercle with an osteotome, completing the line demarcated with the previously made holes. An oscillating saw (ConMed, Utica, NY) is used to release the distal border of the tubercle. The tibial tubercle is then reflected superiorly, exposing the distal edge of the osteotomy (Fig 3). On the basis of preoperative planning, a saw and osteotome are used to create the new location of the tibial tubercle by removing the necessary bone for proper distalization. This distance is typically around 1 cm. A rasp is used to prepare the bony bed before fixation. If medialization is also desired, a rasp is used to ensure that the tubercle will sit flush against the bony bed.
Fig 3.

Intraoperative photograph of a right knee with the tibial tubercle (TT) and patellar tendon reflected superiorly. A second cut is being made in the tibia at the level at which the tubercle will undergo distalization.
Attention is then focused on exposing the trochlea in preparation for the trochleoplasty. A medial parapatellar arthrotomy is made, and the patella is laterally reflected. The distal medial and lateral trochlear facets, as well as the trochlear groove, are delineated with a marking pen. A scalpel is used to elevate the periosteum 5 to 6 mm away from the articular cartilage margins along the proximal bone-cartilage transition of the distal femur. A high-speed burr (ConMed) and reamer (ConMed) are used to remove subchondral bone in a proximal-to-distal fashion, with the previous markings used as a distal endpoint (Fig 4). Emphasis is placed on deepening the trochlear groove. Next, an arthroscope (Dyonics; Smith & Nephew) is used to inspect the undersurface of the trochlea, and adjustments are made to smooth the bony bed and to eliminate any remnant bone bridge. The flap is then pushed into the newly created trough and held in place with four to six Kirschner wires. When good trochlear position is confirmed, a reamer is used over the K-wires and the flap is secured with multiple 3 × 26–mm cannulated Bio-Compression screws (Arthrex) until good fixation is ensured (Fig 5).
Fig 4.

Intraoperative photograph of a right knee with the patella reflected laterally during trochleoplasty. A high-speed reamer is being used to remove subchondral bone. (DMTF, distal medial trochlear facet; TG, trochlear groove.)
Fig 5.

Intraoperative photograph of a right knee with the cartilage flap secured with 3 × 26–mm cannulated Bio-Compression screws. (DLTF, distal lateral trochlear facet; DMTF, distal medial trochlear facet; TG, trochlear groove.)
The tibial tubercle is then pulled distally or medially (or both) to align with the prior bony preparation. Two bicortical K-wires are inserted and checked with fluoroscopy (Fig 6). Once proper placement is confirmed, two fully threaded 4.5-mm cannulated bicortical screws (Synthes) with washers are placed over the K-wires and the osteotomy is secured.
Fig 6.

Intraoperative photographs of a right knee with the tibial tubercle (TT) being pulled distally, secured with two K-wires (A) and then fully threaded 4.5-mm cannulated screws with washers (B), and checked with fluoroscopy.
Next, a passing suture is placed through the patellar tunnel and is used to pull the MPFL graft into the socket and then the cortical fixation device attached to the graft is secured to the lateral patella. The graft is then passed transversely across the previously created channel along the normal course of the native MPFL deep to the superficial layer of the medial retinaculum, just distal to the vastus medialis obliquus (Fig 7). With the knee positioned at 40° of flexion, the graft is tied to the suture anchors previously fixed at the femoral attachment. While the surgeon is tying the first sutures, the patella is manually pushed 4 to 5 mm in a lateral direction to avoid over-medialization. After the graft has several sutures in place, the patella is tested with lateral translation at varying degrees of knee flexion to confirm restoration of an adequate restraint to lateral translation without over-tightening medially. With the patient's knee at 20° of flexion, the surgeon should be able to lateralize the patella one to two quadrants with a gentle pressure applied to the medial facet. Once this is confirmed, the remaining sutures are secured. In addition, the arthrotomy is copiously irrigated and closed. Steri-Strips (3M Health Care, St. Paul, MN) and a sterile dressing are placed over the incision, and the knee is placed into an immobilizer. Pearls and pitfalls of the described procedure are summarized in Table 3, and advantages and limitations are summarized in Table 4.
Fig 7.

Intraoperative photograph sequence of a right knee undergoing medial patellofemoral ligament reconstruction with semitendinosus autograft. (A) The graft is pulled through the patella and secured laterally with a button, (B) a channel beneath the medial retinaculum is created, and (C) the graft is passed and (D) secured to the anchor in its anatomic position.
Table 3.
Pearls and Pitfalls
| Pearls | Pitfalls |
|---|---|
| Follow the distal edge of the vastus medialis obliquus muscle to find the original course of the MPFL to create a soft-tissue tunnel and allow further passage of the graft. | Bony procedures in patients with open physes can lead to physeal arrest and further deformity. Trochleoplasty and TTO should be avoided in these patients. |
| Use the adductor magnus tendon as a reference to find the adductor tubercle and then the femoral attachment of the MPFL. | Damage to the patellar cartilage can occur from drilling the transverse tunnel. To avoid this problem, use an ACL aiming guide and make sure the exit point is at the same level of the entry point. |
| When planning a TTO, bear in mind that distalization of the patella leads to automatic medialization. | The surgeon should be sure to harvest at least 16 cm of semitendinosus graft. Grafts shorter than this may not be sufficient for the MPFL reconstruction. |
| Use a 2-mm drill to create holes in the borders of the planned tubercle osteotomy. This will facilitate the procedure and help prevent an undesired fracture line. | Excessive distalization can lead to iatrogenic patella baja. The needed amount of distalization should be previously planned to prevent this complication. The surgeon should try not to lower it past an Insall-Salvati ratio of 1:1. |
| Use a marking pen to delineate the distal borders of the medial and lateral trochlear facets, as well as the trochlear groove. This will help visualize the limits of the trochleoplasty and the region under the groove, which should be the deepest part. | Proud surfaces in the front of the knee can cause discomfort to the patient. The surgeon should use a rasp to smooth the new tubercle bed and make sure it is flush. |
| Use the arthroscope to better visualize the undersurface of the trochleoplasty and make adjustments to emphasize deepening the trochlear groove. | The surgeon must be careful not to over-tighten the MPFL. The graft should be fixed with the knee at 40° of flexion, and the patella is manually pushed 4-5 mm in a lateral direction to avoid over-medialization. With the patient's knee at 20° of flexion, the surgeon should be able to lateralize the patella one to two quadrants with a gentle pressure applied to the medial facet. |
| When fixing the osteotomy, use fluoroscopy to ensure the correct position of the K-wires as well as the cortical screws that will keep the TT in place. | To avoid fracture of the tibial tubercle when performing the osteotomy, the surgeon should make sure the bone block is strong enough to support two cortical screws. It must measure at least 30 mm in length and include cancellous bone. |
ACL, anterior cruciate ligament; MPFL, medial patellofemoral ligament; TT, tibial tubercle; TTO, tibial tubercle osteotomy.
Table 4.
Advantages and Limitations
| Advantages |
| A single-stage procedure can be performed. |
| Addressing all the problems during the same procedure allows the surgeon to balance the effect of each technique over the patellar tracking and stability. |
| Adding trochleoplasty to the procedure in patients with a dysplastic trochlea (Dejour type B, C, or D) helps normalize the patellar tracking and likely reduces the redislocation rate. |
| Limitations |
| Aggressive procedures can lead to more scar tissue. Physical therapy should be initiated on the first day postoperatively. |
| A longer surgical time is required. |
| The literature still lacks outcome studies reporting results for the combined technique. |
Postoperative Rehabilitation
Patients should remain non–weight bearing and in an immobilizer brace for 6 weeks. A supervised rehabilitation program should start immediately postoperatively. Quadriceps exercises, straight-leg raises, and ankle pumps with the patient wearing a knee immobilizer should be performed 3 to 5 times daily. Passive range of motion should be limited from 0° to 90° of flexion for the first 2 weeks and then increased as tolerated. Return to normal levels of activity typically occurs after 6 to 9 months postoperatively.2
Discussion
Literature regarding the outcomes of combined trochleoplasty, MPFL reconstruction, and TTO for the treatment of patellar instability is limited. However, there are numerous outcome studies regarding trochlear dysplasia treated with trochleoplasty, with and without MPFL reconstruction. Reported patient satisfaction rates have ranged from as low as 67%16 to as high as 95.7%.17 TTO for the treatment of patellar instability has a high success rate.18 In a study by Servien et al.18 that included 135 distalization osteotomies with and without medialization, a 94.5% satisfaction rate was reported at an average follow-up of 5 years. However, a prospective cohort study of 129 knees with recurrent patellar instability treated either with isolated MPFL reconstruction or with MPFL reconstruction plus TTO reported no significant difference in outcomes at 1 year postoperatively.19
Further outcome studies that incorporate all 3 procedures are needed, particularly studies with long-term outcomes. Nonetheless, we believe in the effectiveness of our technique for treating recurrent patellar instability in patients with a dysplastic trochlea, patella alta, an increased TT-TG ratio, and an insufficient MPFL. We recommend our method of treatment for recurrent patellar instability with a trochleoplasty, MPFL reconstruction, and TTO and encourage additional studies by other groups to assess our surgical technique.
Footnotes
The authors report the following potential conflict of interest or source of funding: Steadman Philippon Research Institute receives support from Arthrex, Ossur, Siemens, and Smith & Nephew. R.F.L. receives support from Arthrex; Smith & Nephew; Ossur; Health East, Norway; and National Institutes of Health R13 grant for biologics.
Supplementary Data
Medial patellofemoral ligament (MPFL) reconstruction, open trochleoplasty, and tibial tubercle distalization osteotomy for the treatment of recurrent patellar instability with severe trochlear dysplasia (Dejour type B) and patella alta. With the patient supine on the operating table and the knee flexed to 20°, an anterior midline incision is performed over the knee. The MPFL is identified, a patellar tunnel is created, and suture anchors are placed at the femoral attachment. The semitendinosus tendon is then harvested. Next, the tibial tubercle osteotomy is performed, followed by the open trochleoplasty. Lastly, the MPFL reconstruction is completed.
References
- 1.Fithian D.C., Paxton E.W., Stone M.L. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med. 2004;32:1114–1121. doi: 10.1177/0363546503260788. [DOI] [PubMed] [Google Scholar]
- 2.LaPrade R.F., Cram T.R., James E.W., Rasmussen M.T. Trochlear dysplasia and the role of trochleoplasty. Clin Sports Med. 2014;33:531–545. doi: 10.1016/j.csm.2014.03.005. [DOI] [PubMed] [Google Scholar]
- 3.Mehta V.M., Inoue M., Nomura E. An algorithm guiding the evaluation and treatment of acute primary patellar dislocations. Sports Med Arthrosc. 2007;15:78–81. doi: 10.1097/JSA.0b013e318042b695. [DOI] [PubMed] [Google Scholar]
- 4.Dejour H., Walch G., Nove-Josserand L. Factors of patellar instability: An anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc. 1994;2:19–26. doi: 10.1007/BF01552649. [DOI] [PubMed] [Google Scholar]
- 5.Caton J., Deschamps G., Chambat P. Patella infera. Apropos of 128 cases. Rev Chir Orthop Reparatrice Appar Mot. 1982;68:317–325. [in French] [PubMed] [Google Scholar]
- 6.Malghem J., Maldague B. Depth insufficiency of the proximal trochlear groove on lateral radiographs of the knee: Relation to patellar dislocation. Radiology. 1989;170:507–510. doi: 10.1148/radiology.170.2.2911676. [DOI] [PubMed] [Google Scholar]
- 7.Stefanik J.J., Zumwalt A.C., Segal N.A. Association between measures of patella height, morphologic features of the trochlea, and patellofemoral joint alignment: The MOST study. Clin Orthop Relat Res. 2013;471:2641–2648. doi: 10.1007/s11999-013-2942-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Colvin A.C., West R.V. Patellar instability. J Bone Joint Surg Am. 2008;90:2751–2762. doi: 10.2106/JBJS.H.00211. [DOI] [PubMed] [Google Scholar]
- 9.Dejour D., Saggin P. The sulcus deepening trochleoplasty—The Lyon’s procedure. Int Orthop. 2010;34:311–316. doi: 10.1007/s00264-009-0933-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Desio S.M., Burks R.T., Bachus K.N. Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med. 1998;26:59–65. doi: 10.1177/03635465980260012701. [DOI] [PubMed] [Google Scholar]
- 11.Ho C.P., James E.W., Surowiec R.K. Systematic technique-dependent differences in CT versus MRI measurement of the tibial tubercle-trochlear groove distance. Am J Sports Med. 2015;43:675–682. doi: 10.1177/0363546514563690. [DOI] [PubMed] [Google Scholar]
- 12.Robin J., Neyret P. Tuberosity surgery: What is the role of distalization? Oper Tech Sports Med. 2015;23:107–113. [Google Scholar]
- 13.Farr J. Tibial tubercle osteotomy. Tech Knee Surg. 2003;2:28–42. [Google Scholar]
- 14.Dejour D.H. The patellofemoral joint and its historical roots: The Lyon School of Knee Surgery. Knee Surg Sports Traumatol Arthrosc. 2013;21:1482–1494. doi: 10.1007/s00167-012-2331-9. [DOI] [PubMed] [Google Scholar]
- 15.LaPrade R.F., Engebretsen A.H., Ly T.V. The anatomy of the medial part of the knee. J Bone Joint Surg Am. 2007;89:2000–2010. doi: 10.2106/JBJS.F.01176. [DOI] [PubMed] [Google Scholar]
- 16.Goutallier D., Raou D., Van Driessche S. Retro-trochlear wedge reduction trochleoplasty for the treatment of painful patella syndrome with protruding trochleae. Technical note and early results. Rev Chir Orthop Reparatrice Appar Mot. 2002;88:678–685. [in French] [PubMed] [Google Scholar]
- 17.Nelitz M., Dreyhaupt J., Lippacher S. Combined trochleoplasty and medial patellofemoral ligament reconstruction for recurrent patellar dislocations in severe trochlear dysplasia: A minimum 2-year follow-up study. Am J Sports Med. 2013;41:1005–1012. doi: 10.1177/0363546513478579. [DOI] [PubMed] [Google Scholar]
- 18.Servien E., Verdonk P.C., Neyret P. Tibial tuberosity transfer for episodic patellar dislocation. Sports Med Arthrosc. 2007;15:61–67. doi: 10.1097/JSA.0b013e3180479464. [DOI] [PubMed] [Google Scholar]
- 19.Mulliez A, Lambrecht D, Verbruggen D, Van Der Straeten C, Verdonk P, Victor J. Clinical outcome in MPFL reconstruction with and without tuberositas transposition. Knee Surg Sports Traumatol Arthrosc in press, available online 2 June, 2015. doi:10.1007/s00167-015-3654-0. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Medial patellofemoral ligament (MPFL) reconstruction, open trochleoplasty, and tibial tubercle distalization osteotomy for the treatment of recurrent patellar instability with severe trochlear dysplasia (Dejour type B) and patella alta. With the patient supine on the operating table and the knee flexed to 20°, an anterior midline incision is performed over the knee. The MPFL is identified, a patellar tunnel is created, and suture anchors are placed at the femoral attachment. The semitendinosus tendon is then harvested. Next, the tibial tubercle osteotomy is performed, followed by the open trochleoplasty. Lastly, the MPFL reconstruction is completed.