

Sir,
A 73-year-old man presented with a plaque lesion on the nose of three years duration. No prominent change has occured on the lesion for a long time. On examination, a brown, waxy surfaced, sharply circumscribed plaque lesion on the left side of the nose near the medial epicanthus was observed [Figure 1a]. Milia-like cysts and comedo-like openings were also observed on dermoscopy. The lesion was asymptomatic. The patient was diagnosed as seborrheic keratosis (SebK) on clinical findings and dermoscopy. He refused cryotherapy or surgical resection and requested topical treatment. Diclofenac gel was started twice a day. The lesion was completely cleared after one month [Figure 1b].
Figure 1.
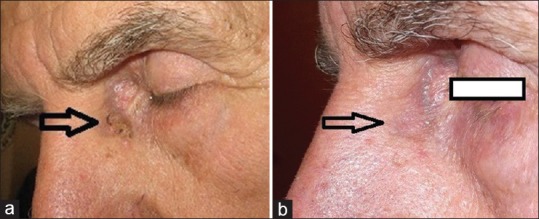
(a) Seborrheic keratosis lesion on the nose. (b) Disappearence of the lesion after the treatment with diclofenac gel (arrows)
SebK is one of the most common benign epidermal tumors. The lesions are usually removed for cosmetic reasons. The most commonly used treatment methods for SebK are cryosurgery with liquid nitrogen and curettage. Topical drugs such as tazarotene, dobesilate, calcipotriene, ammonium lactate, and imiquimod are the other therapeutic options for SebK.[1,2,3,4]
Diclofenac gel is a nonsteroidal anti-inflammatory drug that is used to treat actinic keratosis. It inhibits the cyclooxygenase pathway and decrease prostaglandin E2 (PGE2) synthesis. The drug is generally applied twice a day for 2-3 months. The complete clearance rate for actinic keratosis was 47% at 3 months follow up.[5] We herein present a case of SebK succesfully treated with diclofenac gel 3%. The lesion was completely cleared after the application of diclofenac gel twice a day for one month. The pathogenesis of SebK are not clearly understood. Diclofenac is an anti-inflammatory agent.[5] Although we failed to explain the mechanism of action of diclofenac on SebK lesions, this is the first such case reported. We believe that, diclofenac deserves to be investigated further as a treatment option for SebK.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Herron MD, Bowen AR, Krueger GG. Seborrheic keratoses: A study comparing the standard cryosurgery with topical calcipotriene, topical tazarotene, and topical imiquimod. Int J Dermatol. 2004;43:300–2. doi: 10.1111/j.1365-4632.2004.02282.x. [DOI] [PubMed] [Google Scholar]
- 2.Cuevas P, Angulo J, Salgüero I, Giménez-Gallego G. Clearance of seborrhoeic keratoses with topical dobesilate. BMJ Case Rep 2012. 2012:pii: bcr0120125628. doi: 10.1136/bcr.01.2012.5628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Asagami C, Muto M, Hirota T, Shimizu T, Hamamoto Y. Anti-tumor effects of 1,25-dihydroxyvitamin D3 (1,25(OH) 2D3) in seborrheic keratosis. J Investig Dermatol Symp Proc. 1996;1:94–6. [PubMed] [Google Scholar]
- 4.Klaus MV, Wehr RF, Rogers RS, Jr, Russell TJ, Krochmal L. Evaluation of ammonium lactate in the treatment of seborrheic keratoses. J Am Acad Dermatol. 1990;22:199–203. doi: 10.1016/0190-9622(90)70023-b. [DOI] [PubMed] [Google Scholar]
- 5.Dréno B, Amici JM, Basset-Seguin N, Cribier B, Claudel JP, Richard MA. AKTeam™. Management of actinic keratosis: A practical report and treatment algorithm from AKTeam™ expert clinicians. J Eur Acad Dermatol Venereol. 2014;28:1141–9. doi: 10.1111/jdv.12434. [DOI] [PubMed] [Google Scholar]