

We will focus on those MR methods that have shown promise in demonstrating evidence of subtle brain injury in mild traumatic brain injury not apparent at conventional imaging; these can be considered in three main categories based on their ability to characterize brain structure, function, and metabolism.
Abstract
Mild traumatic brain injury (mTBI), also commonly referred to as concussion, affects millions of Americans annually. Although computed tomography is the first-line imaging technique for all traumatic brain injury, it is incapable of providing long-term prognostic information in mTBI. In the past decade, the amount of research related to magnetic resonance (MR) imaging of mTBI has grown exponentially, partly due to development of novel analytical methods, which are applied to a variety of MR techniques. Here, evidence of subtle brain changes in mTBI as revealed by these techniques, which are not demonstrable by conventional imaging, will be reviewed. These changes can be considered in three main categories of brain structure, function, and metabolism. Macrostructural and microstructural changes have been revealed with three-dimensional MR imaging, susceptibility-weighted imaging, diffusion-weighted imaging, and higher order diffusion imaging. Functional abnormalities have been described with both task-mediated and resting-state blood oxygen level–dependent functional MR imaging. Metabolic changes suggesting neuronal injury have been demonstrated with MR spectroscopy. These findings improve understanding of the true impact of mTBI and its pathogenesis. Further investigation may eventually lead to improved diagnosis, prognosis, and management of this common and costly condition.
© RSNA, 2016
Introduction
Approximately 1.7 million new cases of traumatic brain injury (TBI) occur in the United States annually, generating over a million emergency room visits (1). The majority, 70%–90%, represent mild injury (2), which is now known to cause more morbidity than previously thought (3). Aside from civilian injury, it is also estimated that up to 35% of the 1.6 million U.S. military service members deployed to Iraq and Afghanistan over the past decade have sustained mild TBI (mTBI) (4). A substantial number of mTBI patients have measurable deficits in a number of cognitive domains, including processing speed, attention, and memory (4,5). A subgroup of patients has persistent symptoms, known as postconcussion syndrome (6). It is estimated that up to 40%–50% of mTBI patients continue to have symptoms at 3 months after injury (7,8) and 10%–15% at 1 year (9). Postconcussion syndrome can cause significant long-term disability and loss of productivity, contributing to the estimated $17 billion that mTBI costs the United States annually in direct expenses and lost income (1,10).
Though common, merely defining mTBI is a challenge, as multiple different agencies including the World Health Organization (11), the Veterans Administration/Department of Defense (12), and the American Congress of Rehabilitation Medicine (13) all have differing criteria. To further complicate matters, the term concussion is frequently used interchangeably or as an alternative to mTBI (14). Some characteristics that are common to most definitions of mTBI and concussion include a Glasgow Coma Scale score of 13 or higher at the time of injury, posttraumatic amnesia of less than 24 hours, loss of consciousness for less than 30 minutes, or transient neurologic defects or disorientation at the time of injury (14). For the purpose of this review, we will use these characteristics to define mTBI. Some organizations also differentiate between uncomplicated and complicated mTBI, depending on whether any intracranial abnormalities are found at the time of injury on conventional imaging studies (14). Conventional imaging findings are often normal in mTBI, and the presence of computed tomographic (CT) abnormalities in mTBI has not consistently been found to correlate with symptoms. Thus, the clinical significance of this distinction is not completely clear (15).
To add to the challenge of the clinical study of this entity, mTBI encompasses a wide spectrum of injury mechanisms (eg, direct impact, acceleration-deceleration, and blast injuries), with potentially different outcome patterns (16,17). For example, blast injuries, more commonly seen in military populations, have been shown to cause more diffuse and spatially variable white matter (WM) damage than nonblast injuries (18). Confounding factors, such as pre-existing psychiatric illness drug or alcohol misuse, are prevalent in patients presenting with mTBI in both civilian and military populations (19–27). Sport-related injuries are also quite prevalent and have recently been in the media spotlight (28). Athletes competing in high-risk sports may endure multiple episodes of concussive or subconcussive head impacts, with cumulative effects that are impossible to quantify and attribute to individual events. In fact, these cumulative effects are thought to be responsible for chronic traumatic encephalopathy, a neurodegenerative disease traditionally reported in boxers and football players who have sustained multiple episodes of mTBI (29). Cumulative effects of mTBI have also been identified in a military population, where repeated mTBI blast injuries caused significant increases in neurobehavioral symptoms (30). Lastly, the determination of symptom severity by patient self-report introduces reporting bias (31). Coexisting psychiatric illness, substance abuse, and participation in high-stakes sports may all produce ulterior motives or attribution errors that can undermine the accuracy of self-reported symptoms and injury timeline.
From an imaging perspective, CT remains the standard of care for emergent evaluation and triage of acute TBI, regardless of severity (32,33). In certain situations, magnetic resonance (MR) imaging may prove useful as an adjunct modality, as it might reveal more subtle injury (34,35) and improve short-term outcome prediction over CT (36). In assessing long-term outcome for mTBI, however, there is essentially no role for conventional CT and MR imaging, as the findings are frequently normal in this setting.
In the past decade, the number of research articles related to MR imaging of mTBI has grown exponentially (Fig 1), due in large part to a growing public awareness of the disease, as well as the development of novel MR and analytical techniques. In this review, we will focus on those MR methods that have shown promise in demonstrating evidence of subtle brain injury in mTBI not apparent at conventional imaging; these can be considered in three main categories based on their ability to characterize brain structure, function, and metabolism.
Figure 1:

Graph shows the number of articles found in PubMed from 1990 to the year indicated on the x-axis, with search terms as specified in the legend. An increase in rate of publication is demonstrated with all search parameters after 2005.
Structural Imaging
Macrostructural Changes: Brain Morphometry
Despite lack of evidence for direct injury by most conventional imaging, measurable morphometric changes have recently been described in mTBI by using a variety of segmentation techniques. These segmentation techniques have found cortical thickening after mTBI, presumably related to edema, which have correlated with outcome. In fact, in a study of motor-vehicle accident survivors imaged 2 weeks and 3 months after injury, mTBI patients demonstrated thicker cortex of the left rostral middle frontal gyrus and right precuneus gyrus than did non-mTBI survivors (37). Greater cortical thickness of the right precuneus in the acute phase correlated with acute traumatic stress symptoms (37). The attribution of early cortical thickening to transient brain edema has been demonstrated in mTBI animal models (38).
Postinjury increase in cortical thickness appears to be transient in humans, as well. Toth et al showed cortical volume loss to be present as early as 1 month after mTBI (39). Wang et al demonstrated that after 3 months, there was cortical thinning in the left rostral middle frontal gyrus of mTBI patients relative to the acute phase (37). In military service members who sustained mild blast injury, Tate et al showed subacute-to-chronic cortical thinning in the left superior frontal and temporal gyri, areas that are functionally implicated in audition and language. In a post hoc review, most of their patients were found to have audiology problems (40). Similar cortical atrophy has also been demonstrated in a pediatric population (41).
Morphometric changes after mTBI appear to extend beyond the cortex. In a study of professional boxers, caudate volume loss was found to correlate with the number of years of professional fighting after adjusting for age, race, and education, presumably secondary to cumulative effects of multiple concussive episodes (42). In a longitudinal study of civilian individuals after a single episode of mTBI, Zhou et al found global volume loss greater than what was seen in age-matched healthy control subjects between the subacute phase of injury (average 1 month) and 1-year follow-up (Fig 2). There was significant WM volume loss in the anterior cingulum and the cingulate gyrus isthmus, as well as precuneal cortex (43). In addition, these structural findings correlated with neuropsychiatric testing performance: Over time, left rostral anterior cingulate volume loss correlated with a decrease in verbal learning scores, right rostral anterior cingulate volume loss correlated with decreases in scores of sustained attention, concentration, working memory, and information processing, and lower left cingulate gyrus isthmus WM volumes correlated with higher scores on anxiety and postconcussion syndrome clinical symptoms (43).
Figure 2a:
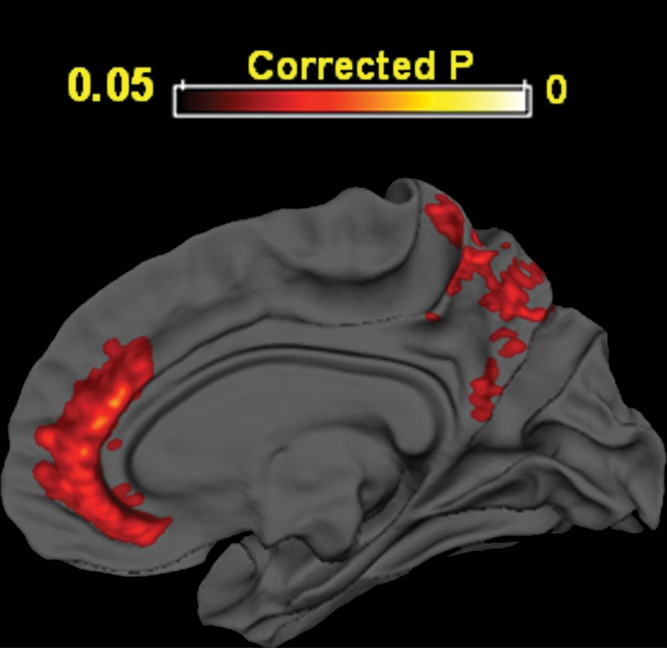
Areas of significant volume loss are demonstrated by projecting coregistered data from (a) medial and (b) lateral projections in 28 mTBI patients and (c) medial and (d) lateral projections in 22 control subjects onto right cerebral hemisphere templates after 1 year (Bonferroni-corrected P < .05). (Parts a and b reprinted from reference 43.)
Figure 2b:
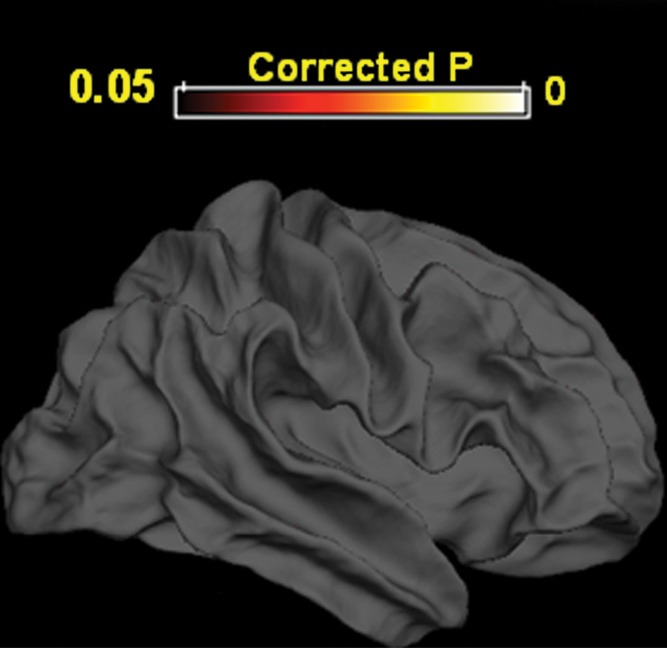
Areas of significant volume loss are demonstrated by projecting coregistered data from (a) medial and (b) lateral projections in 28 mTBI patients and (c) medial and (d) lateral projections in 22 control subjects onto right cerebral hemisphere templates after 1 year (Bonferroni-corrected P < .05). (Parts a and b reprinted from reference 43.)
Figure 2c:
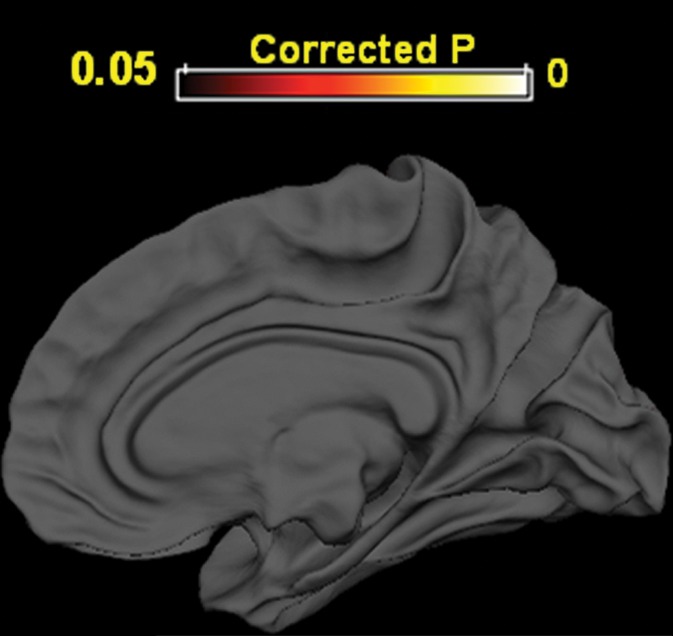
Areas of significant volume loss are demonstrated by projecting coregistered data from (a) medial and (b) lateral projections in 28 mTBI patients and (c) medial and (d) lateral projections in 22 control subjects onto right cerebral hemisphere templates after 1 year (Bonferroni-corrected P < .05). (Parts a and b reprinted from reference 43.)
Figure 2d:
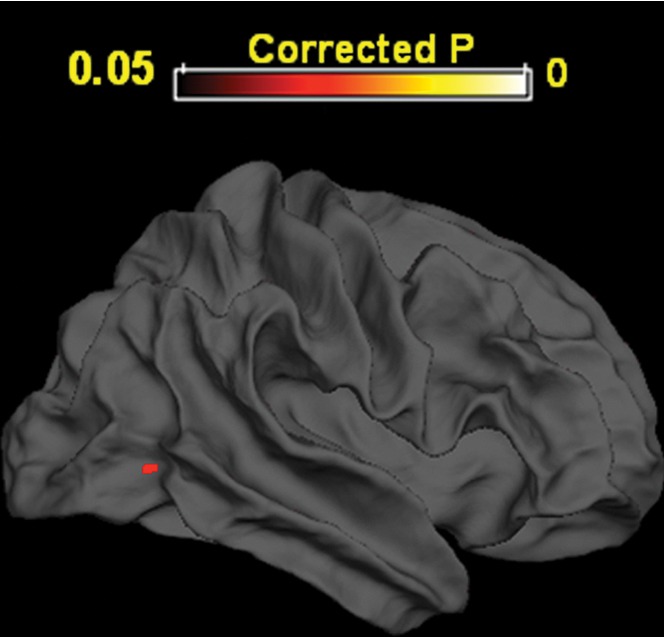
Areas of significant volume loss are demonstrated by projecting coregistered data from (a) medial and (b) lateral projections in 28 mTBI patients and (c) medial and (d) lateral projections in 22 control subjects onto right cerebral hemisphere templates after 1 year (Bonferroni-corrected P < .05). (Parts a and b reprinted from reference 43.)
Even decades after injury, middle-aged adults who sustained remote mTBI were found to have lower hippocampal volume when compared with age-matched control subjects (44). Overall, the presence of macroscopic morphologic changes supports the presence of long-term brain injury after mTBI in at least a subgroup of patients, despite the lack of evidence for direct injury at conventional imaging.
Microstructural Alterations: Diffusion MR Imaging and Magnetization Transfer Imaging
Axons are considered especially vulnerable to shearing injury from rotational, accelerational, and decelerational forces. Traumatic axonal injury has been well described in human studies as well as in animal models of TBI, most prevalent in moderate to severe injury (45), but demonstrable in mTBI as well (46). In normal axon bundles, free diffusion of water is radially restricted by these highly organized structures; thus, traumatic axonal injury is expected to cause abnormal diffusion metrics in WM (47). Diffusion-tensor imaging (DTI), the technical basis of which has been previously reviewed, for example by Mukherjee et al, allows for the investigation of such WM microstructural changes in vivo (47). In 2002, Arfanakis et al demonstrated decreased fractional anisotropy (FA), primarily within the corpus callosum and internal capsule, in a small cohort of patients with acute mTBI (48). Kraus et al corroborated this finding in a chronic mTBI cohort, showing decreased FA in the corticospinal tract, sagittal stratum, and superior longitudinal fasciculus. Numerous articles published since then support the findings of decreased FA and increased mean diffusivity in various WM tracts after mTBI, some correlating with symptom severity and persistence (49–53). Alterations in these metrics were strongly correlated with the number of “knockouts” in a study of boxers and mixed martial artists, supporting cumulative effects of multiple episodes of mTBI (54).
Interestingly, a minority of articles report regions of increased FA after mTBI relative to those of control subjects (55,56). In a meta-analysis of mTBI research published before November 2011, Eierud et al found that such paradoxical findings are significantly more common for studies of acute mTBI (less than 2 weeks), while lower FA values are generally reported for studies of postacute mTBI (57). These results suggest that anisotropy changes in mTBI are dependent on the time since injury. Transient axonal swelling and loss of extracellular (and thus freely diffusing) water have been proposed as possible reasons behind this early increase in FA (55). Compensatory changes related to Wallerian degeneration of other tracts, as well as selective axonal loss within an area of crossing fibers, are other potential explanations for this paradoxical increase (58). Thus, improved delineation of complex axonal anatomy may contribute to a better understanding of such apparently disparate DTI data.
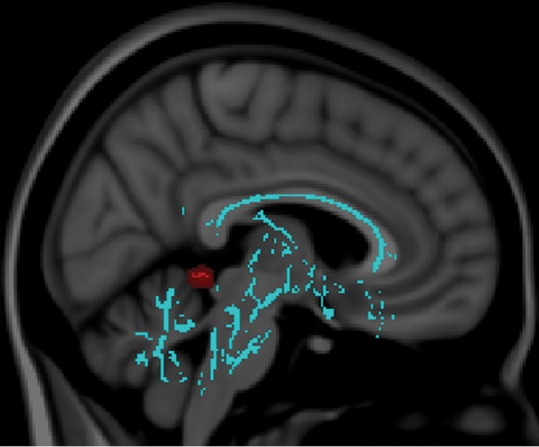
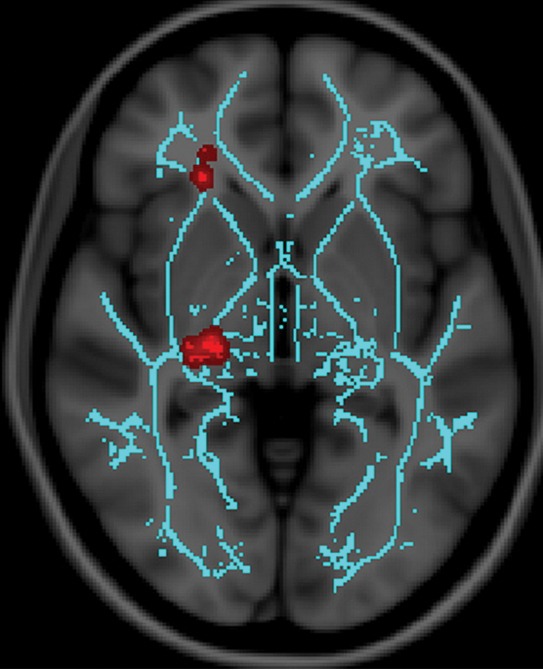
There is evidence of correspondence between DTI metrics and clinical symptoms of mTBI. In their meta-analysis, Eierud et al found that this connection appears to be time-dependent as well, with lower neuropsychological performance correlating with higher anisotropy in the acute phase and lower anisotropy in later phases (57). The number of regions with decreased FA has also been negatively correlated with cognitive outcome (59). Lipton et al linked prefrontal WM FA decreases to lower executive function (60). In terms of noncognitive symptoms of mTBI, Alhilali et al demonstrated a correspondence between decreased FA in the cerebellum/fusiform gyri and vestibular symptoms, as well as decreased FA in the right anterior thalamic radiation/geniculate nucleus optic tracts and ocular convergence insufficiency (Fig 3) (61). Fakhran et al have also demonstrated that sleep/wake disturbances in mTBI patients are correlated with decreased FA in the parahippocampal gyri (62). Taken together, these DTI findings suggest that axonal injury is related to cognitive deficits, as well as postconcussion symptoms in mTBI patients.
Figure 3a:
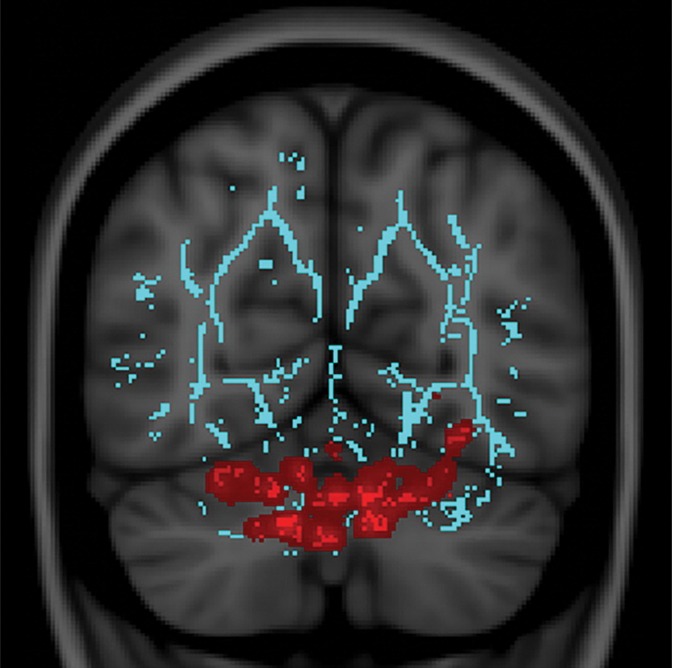
In 30 mTBI patients, vestibular disturbances correlated with (a) decreased FA in cerebellar regions and (b) increased mean diffusivity in vermian lobules of the spinocerebellum, while convergence insufficiency in 25 mTBI patients correlated with (c) increased FA in the right anterior thalamic and right geniculate nucleus optic radiations. Images were derived from tract-based spatial statistics (TBSS) results and rendered on T1-weighted images from the Montreal Neurologic Institute in coronal (a), sagittal (b), and axial (c) projections. Significant voxels (P < .05, corrected for multiple comparisons) were thickened by using TBSS fill function into local tracts (red) and overlaid on WM skeleton (blue). (Reprinted from reference 61.)
Figure 3b:
In 30 mTBI patients, vestibular disturbances correlated with (a) decreased FA in cerebellar regions and (b) increased mean diffusivity in vermian lobules of the spinocerebellum, while convergence insufficiency in 25 mTBI patients correlated with (c) increased FA in the right anterior thalamic and right geniculate nucleus optic radiations. Images were derived from tract-based spatial statistics (TBSS) results and rendered on T1-weighted images from the Montreal Neurologic Institute in coronal (a), sagittal (b), and axial (c) projections. Significant voxels (P < .05, corrected for multiple comparisons) were thickened by using TBSS fill function into local tracts (red) and overlaid on WM skeleton (blue). (Reprinted from reference 61.)
Figure 3c:
In 30 mTBI patients, vestibular disturbances correlated with (a) decreased FA in cerebellar regions and (b) increased mean diffusivity in vermian lobules of the spinocerebellum, while convergence insufficiency in 25 mTBI patients correlated with (c) increased FA in the right anterior thalamic and right geniculate nucleus optic radiations. Images were derived from tract-based spatial statistics (TBSS) results and rendered on T1-weighted images from the Montreal Neurologic Institute in coronal (a), sagittal (b), and axial (c) projections. Significant voxels (P < .05, corrected for multiple comparisons) were thickened by using TBSS fill function into local tracts (red) and overlaid on WM skeleton (blue). (Reprinted from reference 61.)
In addition to FA, other diffusion metrics have also been studied in mTBI. Animal models suggest that axial diffusivity correlates with axonal integrity, while radial diffusivity correlates with myelin integrity and extracellular edema (63,64). Studies have demonstrated changes in axial diffusivity (59) as well as radial diffusivity (53,56) in mTBI. Early increases in the acute phase of mTBI have been attributed to transient edema (65). These findings support the existence of additional pathophysiologic changes that accompany axonal injury after mTBI. There is ongoing work to better model and understand various diffusion metrics to delineate underlying cellular pathophysiology (66).
Although region-of-interest–based, voxel-based, and fiber-tracking analyses of DTI have yielded significant insight into axonal injury and TBI, the presence of crossing axonal fibers in any given voxel poses a significant challenge to the use of FA as an accurate metric of the extent of WM injury. This is because crossing WM fibers in a single voxel may result in a low FA value despite high anisotropy in each of the individual fibers (67). Furthermore, first-order diffusion analysis is still limited by the inherent assumptions of its ellipsoidal, Gaussian modeling of diffusion (47). Cellular structures within each voxel create distinct intracellular and extracellular compartments, leading to non-Gaussian water diffusion (68).
Continued advances in DTI acquisition and postprocessing for tractography attempt to address several of these issues (69,70). It is generally accepted that sampling in multiple diffusion-gradient directions yields a more accurate and reliable representation of the complexities of WM anatomy by modeling crossing fibers, in a technique known as high angular resolution diffusion-weighted imaging (HARDI). Multiple different tractography algorithms are available, a discussion of which is beyond the scope of this review (69,70). A recent study using HARDI with 55 diffusion-gradient directions found WM damage to be more widely distributed than previously reported with DTI in Iraq and Afghanistan veterans with remote history of mTBI (71).
Higher order diffusion imaging using multiple and higher b values has also been developed to study non-Gaussian water diffusion, including techniques such as diffusion kurtosis imaging (DKI). DKI incorporates an additional term in the modeling function to assess the degree of deviation from a Gaussian distribution, reflective of tissue microstructure (68). In an animal model of TBI, perturbations in mean kurtosis were shown to be correlated with reactive astrogliosis (72). A recent in vivo study of mTBI patients demonstrated similar perturbations in the anterior internal capsule across three different time points after injury, despite no significant changes in traditional DTI metrics (73). Changes in mean kurtosis and radial kurtosis across time were also correlated with cognitive improvements 1–6 months after injury, demonstrating potential clinical relevance of DKI findings (73). Patients with mTBI have also shown alterations of mean kurtosis in the thalamus that correlated with cognitive impairment (74), suggesting that DKI may offer better sensitivity in the evaluation of gray matter structures that lack high anisotropy. DKI has also allowed for improved modeling of diffusion within intracellular and extracellular spaces and the calculation of axonal water fraction, which reflects myelin fiber density and may play a role in assessing axonal and/or myelin loss in mTBI patients (75). Further studies of mTBI with these higher order diffusion metrics will offer potential insights into microscopic mechanisms of injury.
To date, most—if not all—of the research of diffusion imaging in mTBI consists of population-based studies. There are no diffusion findings that can be used on an individual level to detect injury or predict outcomes. However, current research is being conducted to distinguish mTBI patients from control subjects by using a multimodal classification system, of which diffusion imaging—specifically, the mean kurtosis—plays an important part (76). With further individualized research and development, diffusion imaging may become a useful tool in the assessment of mTBI in the future.
WM integrity has also been measured by using magnetic transfer imaging, which relies on the principle that protons bound in intact macromolecules can exhibit T1 relaxation coupling with free water protons (77). The efficiency of exchange may be quantified as the magnetic transfer ratio (MTR), which can act as a general measure of WM structural integrity. MTR abnormalities have been correlated to axonal loss, Wallerian degeneration, and edema (78–80). Decreased MTR has been shown to correlate with axonal injury and persistent symptoms in moderate to severe TBI (81). Alterations in MTR have also been previously described in mTBI patients (82,83), although a more recent multimodal study did not demonstrate an appreciable difference in MTR between their mTBI cohort and control subjects (84). Thus, further work in the field of magnetic transfer imaging, perhaps by using metrics other than MTR, is necessary to determine its value in the evaluation of mTBI.
Microhemorrhages and Iron Detection: Gradient Echo, Susceptibility-weighted Imaging, and Magnetic Field Correlation
When patients sustain diffuse axonal injury, the same forces that cause axonal injury can also cause vascular injury and hemorrhage (45). Hemorrhagic lesions are more commonly identified in moderate and severe TBI (45), though with increasing sensitivity of newer techniques, there is evidence that microhemorrhages occur in mTBI more commonly than had been previously suspected. Susceptibility-weighted imaging combines magnitude and phase information by using a gradient-echo sequence (85,86) and demonstrates superior sensitivity for paramagnetic deoxygenated blood products after TBI (87–91). Detection of these microhemorrhages in mTBI is important as the presence of hemorrhage correlates with injury severity (91,92) and can explain focal neurologic deficits (Fig 4).
Figure 4:

Image in 40-year-old female bicyclist who sustained mTBI and presented with right visual field homonymous hemianopsia. On axial susceptibility-weighted image, which is highly sensitive for hemorrhage, microhemorrhages can be seen in the region of the left postchiasmatic optic radiation (arrow), as well as medial left cerebral peduncle.
Abnormal susceptibility after mTBI has also been studied as it relates to brain iron. Nisenbaum et al recently reviewed this topic in depth (93). Briefly, animal models show abnormal iron handling in the central nervous system after TBI (94). In human studies, Raz et al found increased magnetic field inhomogeneity in deep gray matter structures (thalamus and globus pallidus) using magnetic field correlation (95), an asymmetric spin-echo pulse sequence thought to reflect magnetic field inhomogeneity induced by iron on the cellular scale (96). Increased iron, implicated in a number of neurodegenerative conditions, can contribute to oxidative stress and facilitate neuronal degeneration (97,98). This is of particular interest in mTBI patients who have persistent symptoms, long-term complications, and poor outcome (93), and further studies are ongoing in this area to determine the importance of iron content in mTBI pathogenesis.
Functional Imaging
Changes in Memory and Attention: Task-mediated Functional MR Imaging
Changes in task-mediated brain activation have been documented after mTBI with blood oxygen level–dependent functional MR imaging. Several groups have demonstrated these changes using working memory tasks (99–101), as this is a domain affected after TBI (102,103). The working memory networks include several regions: dorsal lateral prefrontal cortex, ventral lateral prefrontal cortex, premotor cortex, anterior cingulate, posterior parietal cortex, and basal ganglia (104).
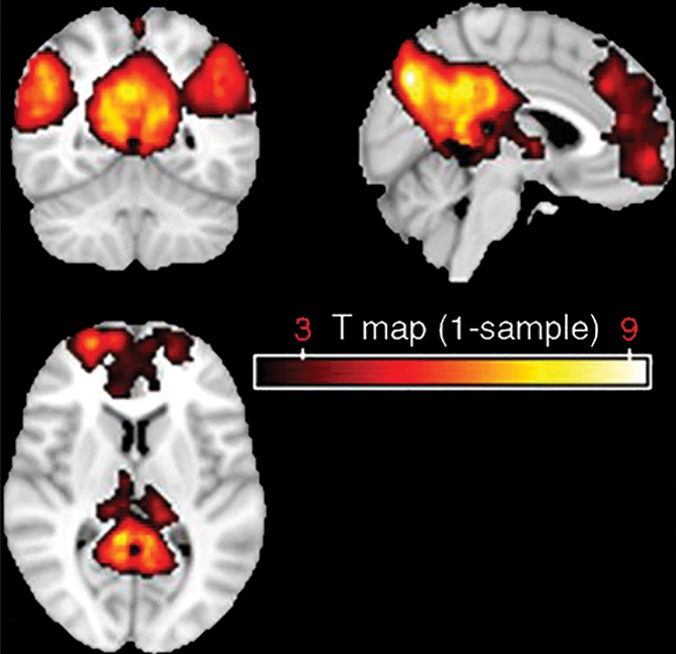
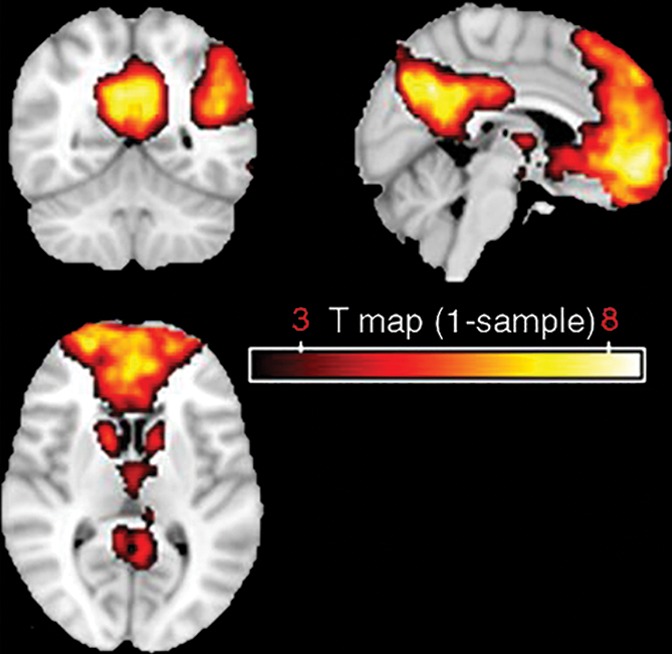
Most studies of working memory in acute-to-subacute mTBI patients have found decreased activity in working memory networks compared with those of control subjects (Fig 5) (100,101,105). Frequently, this is accompanied by abnormally increased activity in areas not traditionally considered part of working memory networks (99,100). Despite these alterations in functional activation patterns, many mTBI patients do not exhibit performance deficits in working memory tasks (99,100). These findings suggest that after mTBI, there may be primary injury or suppression of established working memory networks with compensatory neuronal activation elsewhere. Interestingly, such compensatory activation may not be present in children. In a group of pediatric mTBI patients, Keightley et al found lower activity in multiple areas within the working memory network during verbal and nonverbal working memory tasks. For this pediatric cohort, decreased activity in the bilateral dorsal lateral prefrontal cortex correlated directly with poorer task performance, suggesting a lack of compensatory mechanism (106).
Figure 5:

Blood oxygen level–dependent functional MR activation maps for one-, two-, and three-back working memory tasks (in which subjects were presented with a series of number stimuli and asked to indicate when a given stimulus was identical to the number presented one, two, or three turns ago, respectively) in 20 mTBI patients and 18 control subjects (display threshold, P < .001; extent, three voxels). Lesser extent of activation in the bilateral frontal and parietal regions is seen in the mTBI group. (Reprinted from reference 100.)
In a meta-analysis of functional MR studies, the majority of which investigated working memory, Eierud et al offers a connection between functional and structural abnormalities in mTBI. They found that functional MR imaging activity appears to be decreased anteriorly and increased posteriorly in mTBI subjects relative to that of control subjects. WM anisotropy abnormalities are also more commonly reported anteriorly (57). Anterior regions of the brain are not only associated with working memory circuits but executive function at large. They are also more susceptible to traumatic injury. Increased functional MR imaging activity in the posterior regions may represent compensation for anterior structural and/or functional abnormalities after injury.
Interestingly, some conflicting evidence exists demonstrating that, in the face of a heavier task load, mTBI patients can show greater activation within working memory networks compared with control subjects (99). This activity may again reflect a compensatory change in effort as this patient cohort demonstrated no measurable deficits in task performance (99). Similar findings were also observed in a different patient cohort, where the degree of increased activation correlated with symptom severity (107). These discrepant findings may illustrate challenges inherent to the study of mTBI, where there exists heterogeneity in injury severity, symptoms, mechanism of injury, time course of injury, as well as testing methods and paradigms. All these factors may influence the results of complex tasked-based functional studies (108).
Aside from working memory, task-based studies of other memory domains also demonstrate altered activation in mTBI patients. Improper suppression of declarative memory regions during working memory tasks is linked with duration of posttraumatic amnesia and poor declarative memory function (109). Examinations of episodic memory demonstrated decreased intensity and spatial extent of activation in mTBI patients in response to both familiar and unfamiliar stimuli (110). When presented with an image-based relational memory task, adults with remote history of mTBI were found to have decreased activation in relevant cortical regions as well as poorer task performance relative to control subjects (44).
Dysfunction in the attention circuitry has been observed during auditory orientation tasks (111) designed to evaluate executive cognitive function. Witt et al found that decreased activation in mTBI patients in the right dorsal lateral prefrontal cortex was coupled with increased activation in multiple other frontal and parietal regions (112). Similar to some of the working memory functional studies, these functional MR findings have not been found to correlate with performance or clinical symptoms, suggesting that the increased activation may reflect a compensatory process (112).
Alterations of Baseline Functional Synchronization: Resting-State Functional MR Imaging
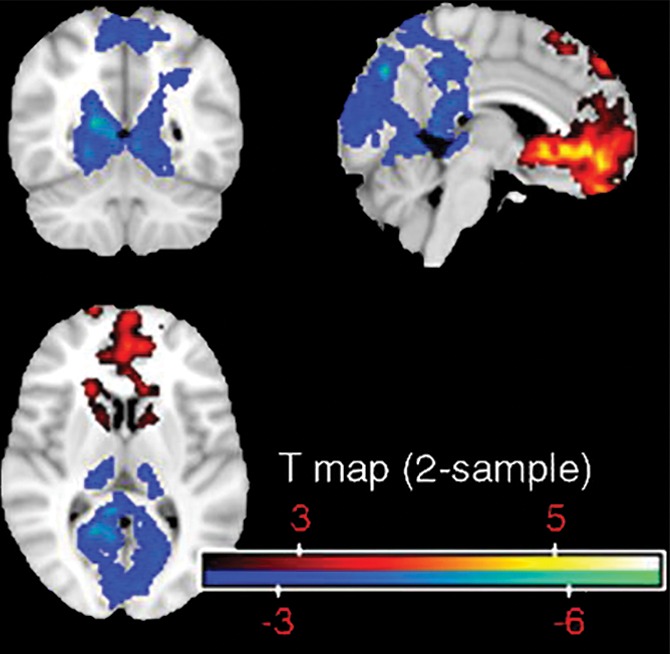
Resting-state functional MR imaging reflects baseline brain functional fluctuations and their synchronization. The default mode network (DMN) is a network of brain areas, including the precuneus, parietal cortex, and orbitofrontal region, that is most active when subjects are at rest, that is, in the absence of a task (113). Abnormalities in the DMN have been reported in severe TBI (114–117), and there is increasing evidence that it is disrupted by mTBI as well. Mayer et al conducted a seed-based resting-state functional MR analysis and found decreased functional connectivity within the DMN (118). These findings were confirmed with an independent component analysis approach by Zhou et al, who showed significantly reduced connectivity in the posterior cingulate cortex and parietal regions, as well as increased frontal connectivity around the medial prefrontal cortex (Fig 6) (119). With both independent component analysis and seed-based analytic methods, Johnson et al correlated decreased connectivity within the DMN with number of concussions experienced by athletes (120). Limited physical stress has been shown to further alter the integrity of the DMN in mTBI patients (121,122). Interestingly, unlike activation changes in task-mediated functional MR imaging, changes in DMN have been linked to neurocognitive dysfunction and posttraumatic symptoms (119). Although the DMN is not activated during functional tasks, this finding suggests that its integrity is intimately connected with cognition and cognitive function. This correlation is also seen in patients with cognitive impairment secondary to other insults, such as aging, stroke, and Parkinson disease (123–127). A lack of compensatory mechanism for resting-state functionality may also help explain this discrepancy. Furthermore, it has been shown that mTBI patients, including those injured with blast mechanisms, exhibit altered internetwork connectivity between the DMN and other networks (118,128,129). In fact, abnormal connections between DMN and the task-positive network and salience network is linked to poorer memory performance in mTBI patients (128).
Figure 6a:
Default mode network templates obtained with hybrid ICA seed method in (a) 18 control subjects and (b) 23 mTBI subjects. (c) Differences between the two groups are highlighted, where blue indicates decreased relative functional connectivity in mTBI subjects and red indicates increased relative functional connectivity (corrected, P < .05; K ≥ 20). (Reprinted from reference 119.)
Figure 6b:
Default mode network templates obtained with hybrid ICA seed method in (a) 18 control subjects and (b) 23 mTBI subjects. (c) Differences between the two groups are highlighted, where blue indicates decreased relative functional connectivity in mTBI subjects and red indicates increased relative functional connectivity (corrected, P < .05; K ≥ 20). (Reprinted from reference 119.)
Figure 6c:
Default mode network templates obtained with hybrid ICA seed method in (a) 18 control subjects and (b) 23 mTBI subjects. (c) Differences between the two groups are highlighted, where blue indicates decreased relative functional connectivity in mTBI subjects and red indicates increased relative functional connectivity (corrected, P < .05; K ≥ 20). (Reprinted from reference 119.)
Other functional networks have also been studied in the resting state. Namely, Sours et al found that reduced interhemispheric connectivity in the dorsal lateral prefrontal cortex at rest was associated with mTBI symptoms and cognitive performance at 1-month follow-up (130). An abnormal increase in the number of thalamocortical resting-state networks has also been shown after mTBI, which speaks to a disruption of the normal small world organization of neuronal networks, where clusters of neighboring functional regions are efficiently linked to anatomically distant clusters by long-range neuronal connections (131–133). Using independent component analysis, Shumskaya et al have documented decreased functional connectivity in the motor-striatal network and increased connectivity in the right frontoparietal network in mTBI patients who have specifically sustained frontal-occipital impact (134).
Together, these findings point to reorganization of a variety of functional neural networks after mTBI, including task-mediated and resting-state neural networks. These changes may be primarily related to injury as well as secondary and compensatory. Alterations in resting-state functional MR imaging seem to correlate with clinical symptoms, indicating that this may be a potentially powerful technique to understand the biologic underpinning of disease after injury.
A Note on Perfusion in mTBI
Blood oxygen level–dependent imaging depends on the cerebral metabolic rate of oxygen consumption, cerebral blood oxygenation, as well as cerebral blood flow and volume. Thus, altered brain perfusion could contribute to and possibly confound results from functional MR studies. Impairment of cerebrovascular autoregulation has been documented in severe, as well as mild TBI, with Doppler velocity recordings (135,136). In TBI patients, cerebral blood volume can be decreased even in areas of the brain that appear normal (137). Using dynamic susceptibility contrast MR imaging, decreased cerebral blood flow to the anterior cingulate and cerebellum, which correlated with neurocognitive results, was demonstrated by Liu et al in mTBI patients (138). Lower thalamic cerebral blood flow in mTBI patients has been demonstrated by using arterial spin labeling MR techniques (139,140). MR findings of cerebral hypoperfusion in the anterior cingulate and frontal lobes are also supported by single photon emission computed tomography (141–144), as well as CT perfusion studies (145–147). Although causation is difficult to establish, perfusion abnormalities have been described in concert with metabolic changes (148) and DTI abnormalities (145), and it is conceivable that hypoxia secondary to hypoperfusion may play a role in perpetuating metabolic disturbance and neuronal injury. Furthermore, these perfusion abnormalities have been linked to clinical metrics of injury (141,145,146), suggesting that the pathogenesis of mTBI likely results from complex interactions between perfusion, functional, structural, and metabolic changes after traumatic injury.
Metabolic Alterations: Proton MR Spectroscopy and a Brief Note on PET
Metabolic changes occurring after mTBI can be examined with standard MR hardware by using hydrogen 1 (1H) MR spectroscopy. Unlike changes in brain morphometry and neuronal connectivity that are dependent on cell death, alterations in metabolite levels are capable of reflecting milder neuronal injury, which is perhaps more common in mTBI. Three main MR spectroscopy metabolites have been evaluated in mTBI: N-acetylaspartate (NAA), a marker of neuronal integrity, creatine (Cr), a marker of energy consumption, and choline (Cho), a marker of cellular turnover. NAA has been extensively studied in mTBI, either in absolute amounts or in ratios to Cr and Cho. Decreases in any of these three values, usually interpreted as neuronal injury, have been recorded throughout the gray matter and WM, in specific regions, as well as globally (149–160). Some of these findings have shown correlations with postconcussive symptoms (156,159), as in a recent study that found lower global WM NAA only in symptomatic patients (Fig 7) (161). These metabolic abnormalities may persist after symptom resolution (155,157,158), with serial studies in sports concussion suggesting a lag of approximately 2 weeks before normalization of the NAA/Cr and NAA/Cho ratios (157,158). A second mTBI prolongs the recovery period of both symptoms and NAA abnormalities (154,158). These data suggest that measures of NAA reflect reversible neurometabolic disturbances, which are related to patient presentation and may have a role in objectively monitoring patient recovery.
Figure 7:

Box plots display 25%, median, 75% (box), and 95% (whiskers) of the NAA concentrations distributions in the WM of 11 postconcussive symptoms–negative and 15 postconcussive symptoms–positive mTBI patients, compared with their age- and sex-matched control subjects (n = 8 and 12, respectively). A significant (P < .001) NAA deficit was observed only in the postconcussive symptoms–positive cohort. (Reprinted from reference 161).
Levels of Cr, a marker of energy metabolism, are often used as the denominator in metabolic ratios, as they are assumed to vary less than the other metabolites (162). It is important, therefore, to consider that three studies suggest Cr alterations in mTBI (163–165). Elevated Cr was found in the centrum semiovale and corpus callosum (163,164), while decreased levels were reported in frontal WM (165). Interestingly, both groups showed normalization of these abnormalities over time, a behavior similar to that of NAA. Changes in Cr, however, may be more heterogeneous as they reflect not only neuronal, but also glial metabolism. Finally, two studies found correlations between WM Cr concentrations and cognitive performance (163,166).
Changes in Cho are usually assessed with a ratio to NAA and Cr. Overall, compared with the other major metabolites, there is less evidence of Cho abnormalities in mTBI. This is consistent with the view that in mTBI, as opposed to more severe injuries, there is less cell-membrane breakdown, which would release 1H MR spectroscopically detectable Cho. In the chronic TBI stages, however, any Cho elevations are likely to reflect glial proliferation (160). Time from injury, therefore, should be taken into account when discussing changes in Cho, while in the interpretation of the NAA/Cho ratio, possible Cho increases (149,167), as well as decreases (166), should be considered.
Only a few studies have examined metabolites detectable exclusively at short echo times in mTBI. The literature on glutamate (Glu), glutamine (Gln), and the Glu and Gln complex (Glx) suggests that, compared with other metabolites, their concentrations are more dependent on tissue types. While in cortical gray matter, Glx (163,164) and Glu/Cr ratio were decreased (156), Glx was increased in WM (164) and the putamen (168). In serial studies, the abnormalities tended to resolve (164,169), but in one instance they were replaced by an increase in myo-inositol (169), a marker of astrocytes, which are an integral part of the glutamate cycle. Intriguingly, in a cross-sectional study that included a much wider range of time from injury (168), myo-inositol elevations were also found alongside higher Glx. In more severe TBI, Glx is increased in both gray matter and WM and that is interpreted as excitotoxicity (170), while myo-inositol changes are thought to reflect astrogliosis (171). The functional meaning of the more heterogeneous findings in mTBI is therefore not clear. Finally, both myo-inositol and Glx abnormalities were not necessarily accompanied by perturbations of NAA or Cho (163,164,168), suggesting the potential of short echo-time spectroscopy to reveal processes not reflected in the concentrations of the more traditional markers.
While not an MR technique, positron emission tomography (PET) has also contributed to the evaluation of brain metabolism in mTBI. However, unlike in moderate or severe TBI, fluorodeoxyglucose (FDG) PET findings in mTBI are not always consistent. While a few studies demonstrate decreased glucose metabolism in the frontal and temporal regions during task performance (172,173), others have shown both increased and decreased metabolic activity that correlates with symptoms (174). Evaluations of glucose uptake in the resting state are equally controversial, with some finding changes in the frontal and temporal lobes (175), while others demonstrating no significant difference (176). Intrinsic heterogeneity of the mTBI patient population and differences in analytical methodology may both contribute to these inconsistencies, and more work is necessary to better determine the role of FDG PET in mTBI. Recently, development of novel PET tracers, such as amyloid and tau ligands, has opened up new areas of investigation. Using amyloid PET, Yang et al have demonstrated increased amyloid β accumulation in mTBI patients with cognitive impairment, supporting the link between mTBI and neurodegenerative disease (177).
Conclusion and Future Directions: Combining Metrics toward Better Evaluation of mTBI
Recent advances in MR imaging have led to multiple insights into the structural, functional, and metabolic disturbances present in mTBI, despite usually normal conventional imaging appearance. Taken together, the current findings support the notion that mTBI causes primary WM damage that is on the mild end of the spectrum of traumatic axonal injury, now detectable with advanced imaging methods. These injuries, in turn, lead to complex, temporally evolving secondary changes in gray matter and WM structure, metabolism, and function that are correlated with symptoms. We are at the threshold of piecing together a more detailed and complete understanding of the mechanisms of injury and recovery after mTBI. Further work is warranted to allow for specific diagnosis, early detection, and stratification, ultimately pointing the way toward targeted treatments.
So far, most imaging research related to mTBI consists of groupwise analyses with limited power and applicability for diagnosis and prognosis on an individual level. With the established findings, however, there is growing interest in developing such individual-based analyses. For example, Kim et al have established a method of analyzing FA maps of individual patients that can discriminate mTBI patients from control subjects (178). There is also growing interest in combining multimodal MR metrics, as well as linking disparate hypotheses in the evaluation of mTBI. Evidence exists that abnormalities in brain volume, DTI, functional neuronal activation, and MR spectroscopy are linked in mTBI (151,179,180). Work by Kou et al examined serum in combination with imaging biomarkers and showed that glial biomarkers correlated with presence of intracranial hemorrhages detected with susceptibility-weighted imaging, while abnormal FA and WM volumes were correlated with impaired neurofunctional status (181). A recent pilot study using a multifeature classification algorithm showed that a multimodal evaluation achieved higher accuracy than the best single metric in differentiating mTBI patients from control subjects (76).
Further advances in these and other novel imaging techniques, validation of the techniques, and linking of relevant imaging metrics are sure to play a role in the development of improved diagnostic criteria and enhanced clinical follow-up for mTBI in the future. In turn, they will hopefully facilitate appropriate intervention for mTBI patients, who currently have few options.
Essentials
■ Developments in MR imaging of mild traumatic brain injury (mTBI) are contributing to improved understanding of its structural, functional, and metabolic sequelae.
■ Structural MR imaging, diffusion-tensor imaging, susceptibility-weighted imaging, and brain iron imaging demonstrate macrostructural and microstructural changes after mTBI; recent work with diffusion imaging using higher order tensor models attempts to improve injury detection and understanding of axonal pathophysiology by resolving crossing fibers in tractography and more accurately modeling intravoxel diffusion.
■ Functional brain activation has been shown to be altered by both task-mediated blood oxygen level–dependent functional MR imaging, as well as resting state functional MR imaging; this includes alterations in the default mode network, suggesting disruptions of intrinsic neural connectivity.
■ Metabolic changes to the brain are present as documented using MR spectroscopy, with the primary finding of decreased N-acetylaspartate, a marker of neuronal injury.
■ Continued progress in identifying imaging biomarkers of mTBI and personalizing these measures can contribute to improved diagnosis, prognosis, and management of this common pathologic condition.
Received November 16, 2014; revision requested December 15; final revision received April 25, 2015; accepted May 18; final version accepted June 4; final review January 21, 2016.
Y.W.L. supported by the National Institute of Neurological Disorders and Stroke (UL1 TR000038), National Institutes of Health (RO1 NS039135-11), and National Institute of Biomedical Imaging and Bioengineering (P41 EB017183). R.I.G. supported by the National Institutes of Health (grant RO1 NS039135-11).
Disclosures of Conflicts of Interest: X.W. Disclosed no relevant relationships. I.I.K. disclosed no relevant relationships. O.G. disclosed no relevant relationships. Y.G. disclosed no relevant relationships. R.I.G. disclosed no relevant relationships. Y.W.L. disclosed no relevant relationships.
Abbreviations:
- Cho
- choline
- Cr
- creatine
- DTI
- diffusion-tensor imaging
- FA
- fractional anisotropy
- mTBI
- mild TBI
- NAA
- N-acetylaspartate
- TBI
- traumatic brain injury
- WM
- white matter
References
- 1.Faul MLW, Wald MM, Coronado VG. Traumatic brain injury in the United States: emergency department visits, hospitalizations and deaths 2002-2006. Atlanta, Ga: Centers for Disease Control and Prevention, 2010. [Google Scholar]
- 2.Cassidy JD, Carroll LJ, Peloso PM, et al. Incidence, risk factors and prevention of mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med 2004;(43 Suppl):28–60. [DOI] [PubMed] [Google Scholar]
- 3.Carroll LJ, Cassidy JD, Cancelliere C, et al. Systematic review of the prognosis after mild traumatic brain injury in adults: cognitive, psychiatric, and mortality outcomes: results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch Phys Med Rehabil 2014;95(3 Suppl):S152–S173. [DOI] [PubMed] [Google Scholar]
- 4.Rigg JL, Mooney SR. Concussions and the military: issues specific to service members. PM R 2011;3(10 Suppl 2):S380–S386. [DOI] [PubMed] [Google Scholar]
- 5.Rimel RW, Giordani B, Barth JT, Boll TJ, Jane JA. Disability caused by minor head injury. Neurosurgery 1981;9(3):221–228. [PubMed] [Google Scholar]
- 6.Prigatano GP, Gale SD. The current status of postconcussion syndrome. Curr Opin Psychiatry 2011;24(3):243–250. [DOI] [PubMed] [Google Scholar]
- 7.Bazarian JJ, Atabaki S. Predicting postconcussion syndrome after minor traumatic brain injury. Acad Emerg Med 2001;8(8):788–795. [DOI] [PubMed] [Google Scholar]
- 8.Sigurdardottir S, Andelic N, Roe C, Jerstad T, Schanke AK. Post-concussion symptoms after traumatic brain injury at 3 and 12 months post-injury: a prospective study. Brain Inj 2009;23(6):489–497. [DOI] [PubMed] [Google Scholar]
- 9.Alexander MP. Mild traumatic brain injury: pathophysiology, natural history, and clinical management. Neurology 1995;45(7):1253–1260. [DOI] [PubMed] [Google Scholar]
- 10.Centers for Disease Control and Prevention . Report to congress on mild traumatic brain injury in the United States: steps to prevent a serious public health problem. Atlanta, Ga: CDC, National Center for Injury Prevention and Control, 2003. [Google Scholar]
- 11.Borg J, Holm L, Cassidy JD, et al. Diagnostic procedures in mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med 2004;36(43 Suppl):61–75. [DOI] [PubMed] [Google Scholar]
- 12.Management of Concussion/mTBI Working Group . VA/DoD clinical practice guideline for management of concussion/mild traumatic brain injury. J Rehabil Res Dev 2009;46(6):CP1–CP68. [PubMed] [Google Scholar]
- 13.Ruff RM, Iverson GL, Barth JT, Bush SS, Broshek DK; Policy NAN. and Committee Planning. Recommendations for diagnosing a mild traumatic brain injury: a National Academy of Neuropsychology education paper. Arch Clin Neuropsychol 2009;24(1):3–10. [DOI] [PubMed] [Google Scholar]
- 14.Rosenbaum SB, Lipton ML. Embracing chaos: the scope and importance of clinical and pathological heterogeneity in mTBI. Brain Imaging Behav 2012;6(2):255–282. [DOI] [PubMed] [Google Scholar]
- 15.Lange RT, Iverson GL, Franzen MD. Neuropsychological functioning following complicated vs uncomplicated mild traumatic brain injury. Brain Inj 2009;23(2):83–91. [DOI] [PubMed] [Google Scholar]
- 16.French LM. Military traumatic brain injury: an examination of important differences. Ann N Y Acad Sci 2010;1208:38–45. [DOI] [PubMed] [Google Scholar]
- 17.Maruta J, Lee SW, Jacobs EF, Ghajar J. A unified science of concussion. Ann N Y Acad Sci 2010;1208:58–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Davenport ND, Lim KO, Armstrong MT, Sponheim SR. Diffuse and spatially variable white matter disruptions are associated with blast-related mild traumatic brain injury. Neuroimage 2012;59(3):2017–2024. [DOI] [PubMed] [Google Scholar]
- 19.Corrigan JD. Substance abuse as a mediating factor in outcome from traumatic brain injury. Arch Phys Med Rehabil 1995;76(4):302–309. [DOI] [PubMed] [Google Scholar]
- 20.Rona RJ, Jones M, Fear NT, et al. Mild traumatic brain injury in UK military personnel returning from Afghanistan and Iraq: cohort and cross-sectional analyses. J Head Trauma Rehabil 2012;27(1):33–44. [DOI] [PubMed] [Google Scholar]
- 21.Petrie EC, Cross DJ, Yarnykh VL, et al. Neuroimaging, behavioral, and psychological sequelae of repetitive combined blast/impact mild traumatic brain injury in Iraq and Afghanistan war veterans. J Neurotrauma 2014;31(5):425–436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kashluba S, Paniak C, Casey JE. Persistent symptoms associated with factors identified by the WHO Task Force on Mild Traumatic Brain Injury. Clin Neuropsychol 2008;22(2):195–208. [DOI] [PubMed] [Google Scholar]
- 23.Cernich AN, Chandler L, Scherdell T, Kurtz S. Assessment of co-occurring disorders in veterans diagnosed with traumatic brain injury. J Head Trauma Rehabil 2012;27(4):253–260. [DOI] [PubMed] [Google Scholar]
- 24.De Guise E, Leblanc J, Dagher J, et al. Early outcome in patients with traumatic brain injury, pre-injury alcohol abuse and intoxication at time of injury. Brain Inj 2009;23(11):853–865. [DOI] [PubMed] [Google Scholar]
- 25.Lange RT, Iverson GL, Franzen MD. Short-term neuropsychological outcome following uncomplicated mild TBI: effects of day-of-injury intoxication and pre-injury alcohol abuse. Neuropsychology 2007;21(5):590–598. [DOI] [PubMed] [Google Scholar]
- 26.Iverson GL, Lange RT, Franzen MD. Effects of mild traumatic brain injury cannot be differentiated from substance abuse. Brain Inj 2005;19(1):11–18. [DOI] [PubMed] [Google Scholar]
- 27.Lagarde E, Salmi LR, Holm LW, et al. Association of symptoms following mild traumatic brain injury with posttraumatic stress disorder vs postconcussion syndrome. JAMA Psychiatry 2014;71(9):1032–1040. [DOI] [PubMed] [Google Scholar]
- 28.Graham R, Rivara FP, Ford MA, Spicer CM, eds. Institute of Medicine, Committee on Sports-Related Concussions in Youth and National Research Council. Sports-related concussions in youth: improving the science, changing the culture. Washington, DC: National Academies Press, 2013. [PubMed] [Google Scholar]
- 29.Montenigro PH, Corp DT, Stein TD, Cantu RC, Stern RA. Chronic traumatic encephalopathy: historical origins and current perspective. Annu Rev Clin Psychol 2015;11:309–330. [DOI] [PubMed] [Google Scholar]
- 30.Reid MW, Miller KJ, Lange RT, et al. A multisite study of the relationships between blast exposures and symptom reporting in a post-deployment active duty military population with mild traumatic brain injury. J Neurotrauma 2014;31(23):1899–1906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lange RT, Iverson GL, Rose A. Post-concussion symptom reporting and the “good-old-days” bias following mild traumatic brain injury. Arch Clin Neuropsychol 2010;25(5):442–450. [DOI] [PubMed] [Google Scholar]
- 32.Barbosa RR, Jawa R, Watters JM, et al. Evaluation and management of mild traumatic brain injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg 2012;73(5 Suppl 4):S307–S314. [DOI] [PubMed] [Google Scholar]
- 33.Tavender EJ, Bosch M, Green S, et al. Quality and consistency of guidelines for the management of mild traumatic brain injury in the emergency department. Acad Emerg Med 2011;18(8):880–889. [DOI] [PubMed] [Google Scholar]
- 34.Jagoda AS, Bazarian JJ, Bruns JJ, Jr, et al. Clinical policy: neuroimaging and decisionmaking in adult mild traumatic brain injury in the acute setting. Ann Emerg Med 2008;52(6):714–748. [DOI] [PubMed] [Google Scholar]
- 35.Kim SC, Park SW, Ryoo I, et al. Contrast-enhanced FLAIR (fluid-attenuated inversion recovery) for evaluating mild traumatic brain injury. PLoS One 2014;9(7):e102229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Yuh EL, Mukherjee P, Lingsma HF, et al. Magnetic resonance imaging improves 3-month outcome prediction in mild traumatic brain injury. Ann Neurol 2013;73(2):224–235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wang X, Xie H, Cotton AS, et al. Early cortical thickness change after mild traumatic brain injury following motor vehicle collision. J Neurotrauma 2015;32(7):455–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lewén A, Fredriksson A, Li GL, Olsson Y, Hillered L. Behavioural and morphological outcome of mild cortical contusion trauma of the rat brain: influence of NMDA-receptor blockade. Acta Neurochir (Wien) 1999;141(2):193–202. [DOI] [PubMed] [Google Scholar]
- 39.Toth A, Kovacs N, Perlaki G, et al. Multi-modal magnetic resonance imaging in the acute and sub-acute phase of mild traumatic brain injury: can we see the difference? J Neurotrauma 2013;30(1):2–10. [DOI] [PubMed] [Google Scholar]
- 40.Tate DF, York GE, Reid MW, et al. Preliminary findings of cortical thickness abnormalities in blast injured service members and their relationship to clinical findings. Brain Imaging Behav 2014;8(1):102–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mayer AR, Hanlon FM, Ling JM. Gray matter abnormalities in pediatric mild traumatic brain injury. J Neurotrauma 2015;32(10):723–730. [DOI] [PubMed] [Google Scholar]
- 42.Bernick C, Banks S. What boxing tells us about repetitive head trauma and the brain. Alzheimers Res Ther 2013;5(3):23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Zhou Y, Kierans A, Kenul D, et al. Mild traumatic brain injury: longitudinal regional brain volume changes. Radiology 2013;267(3):880–890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Monti JM, Voss MW, Pence A, McAuley E, Kramer AF, Cohen NJ. History of mild traumatic brain injury is associated with deficits in relational memory, reduced hippocampal volume, and less neural activity later in life. Front Aging Neurosci 2013;5:41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bigler ED, Maxwell WL. Neuropathology of mild traumatic brain injury: relationship to neuroimaging findings. Brain Imaging Behav 2012;6(2):108–136. [DOI] [PubMed] [Google Scholar]
- 46.Browne KD, Chen XH, Meaney DF, Smith DH. Mild traumatic brain injury and diffuse axonal injury in swine. J Neurotrauma 2011;28(9):1747–1755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Mukherjee P, Berman JI, Chung SW, Hess CP, Henry RG. Diffusion tensor MR imaging and fiber tractography: theoretic underpinnings. AJNR Am J Neuroradiol 2008;29(4):632–641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Arfanakis K, Haughton VM, Carew JD, Rogers BP, Dempsey RJ, Meyerand ME. Diffusion tensor MR imaging in diffuse axonal injury. AJNR Am J Neuroradiol 2002;23(5):794–802. [PMC free article] [PubMed] [Google Scholar]
- 49.Miles L, Grossman RI, Johnson G, Babb JS, Diller L, Inglese M. Short-term DTI predictors of cognitive dysfunction in mild traumatic brain injury. Brain Inj 2008;22(2):115–122. [DOI] [PubMed] [Google Scholar]
- 50.Aoki Y, Inokuchi R, Gunshin M, Yahagi N, Suwa H. Diffusion tensor imaging studies of mild traumatic brain injury: a meta-analysis. J Neurol Neurosurg Psychiatry 2012;83(9):870–876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Brandstack N, Kurki T, Tenovuo O. Quantitative diffusion-tensor tractography of long association tracts in patients with traumatic brain injury without associated findings at routine MR imaging. Radiology 2013;267(1):231–239. [DOI] [PubMed] [Google Scholar]
- 52.Yuh EL, Cooper SR, Mukherjee P, et al. Diffusion tensor imaging for outcome prediction in mild traumatic brain injury: a TRACK-TBI study. J Neurotrauma 2014;31(17):1457–1477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kumar R, Gupta RK, Husain M, et al. Comparative evaluation of corpus callosum DTI metrics in acute mild and moderate traumatic brain injury: its correlation with neuropsychometric tests. Brain Inj 2009;23(7):675–685. [DOI] [PubMed] [Google Scholar]
- 54.Shin W, Mahmoud SY, Sakaie K, et al. Diffusion measures indicate fight exposure-related damage to cerebral white matter in boxers and mixed martial arts fighters. AJNR Am J Neuroradiol 2014;35(2):285–290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bazarian JJ, Zhong J, Blyth B, Zhu T, Kavcic V, Peterson D. Diffusion tensor imaging detects clinically important axonal damage after mild traumatic brain injury: a pilot study. J Neurotrauma 2007;24(9):1447–1459. [DOI] [PubMed] [Google Scholar]
- 56.Mayer AR, Ling J, Mannell MV, et al. A prospective diffusion tensor imaging study in mild traumatic brain injury. Neurology 2010;74(8):643–650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Eierud C, Craddock RC, Fletcher S, et al. Neuroimaging after mild traumatic brain injury: review and meta-analysis. Neuroimage Clin 2014;4:283–294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Lo C, Shifteh K, Gold T, Bello JA, Lipton ML. Diffusion tensor imaging abnormalities in patients with mild traumatic brain injury and neurocognitive impairment. J Comput Assist Tomogr 2009;33(2):293–297. [DOI] [PubMed] [Google Scholar]
- 59.Kraus MF, Susmaras T, Caughlin BP, Walker CJ, Sweeney JA, Little DM. White matter integrity and cognition in chronic traumatic brain injury: a diffusion tensor imaging study. Brain 2007;130(Pt 10):2508–2519. [DOI] [PubMed] [Google Scholar]
- 60.Lipton ML, Gulko E, Zimmerman ME, et al. Diffusion-tensor imaging implicates prefrontal axonal injury in executive function impairment following very mild traumatic brain injury. Radiology 2009;252(3):816–824. [DOI] [PubMed] [Google Scholar]
- 61.Alhilali LM, Yaeger K, Collins M, Fakhran S. Detection of central white matter injury underlying vestibulopathy after mild traumatic brain injury. Radiology 2014;272(1):224–232. [DOI] [PubMed] [Google Scholar]
- 62.Fakhran S, Yaeger K, Alhilali L. Symptomatic white matter changes in mild traumatic brain injury resemble pathologic features of early Alzheimer dementia. Radiology 2013;269(1):249–257. [DOI] [PubMed] [Google Scholar]
- 63.Mac Donald CL, Dikranian K, Bayly P, Holtzman D, Brody D. Diffusion tensor imaging reliably detects experimental traumatic axonal injury and indicates approximate time of injury. J Neurosci 2007;27(44):11869–11876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Wang S, Wu EX, Qiu D, Leung LH, Lau HF, Khong PL. Longitudinal diffusion tensor magnetic resonance imaging study of radiation-induced white matter damage in a rat model. Cancer Res 2009;69(3):1190–1198. [DOI] [PubMed] [Google Scholar]
- 65.Hasan KM, Wilde EA, Miller ER, et al. Serial atlas-based diffusion tensor imaging study of uncomplicated mild traumatic brain injury in adults. J Neurotrauma 2014;31(5):466–475. [DOI] [PubMed] [Google Scholar]
- 66.Novikov DS, Jensen JH, Helpern JA, Fieremans E. Revealing mesoscopic structural universality with diffusion. Proc Natl Acad Sci U S A 2014;111(14):5088–5093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Chung HW, Chou MC, Chen CY. Principles and limitations of computational algorithms in clinical diffusion tensor MR tractography. AJNR Am J Neuroradiol 2011;32(1):3–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Steven AJ, Zhuo J, Melhem ER. Diffusion kurtosis imaging: an emerging technique for evaluating the microstructural environment of the brain. AJR Am J Roentgenol 2014;202(1):W26–W33. [DOI] [PubMed] [Google Scholar]
- 69.Berman JI, Lanza MR, Blaskey L, Edgar JC, Roberts TP. High angular resolution diffusion imaging probabilistic tractography of the auditory radiation. AJNR Am J Neuroradiol 2013;34(8):1573–1578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Farquharson S, Tournier JD, Calamante F, et al. White matter fiber tractography: why we need to move beyond DTI. J Neurosurg 2013;118(6):1367–1377. [DOI] [PubMed] [Google Scholar]
- 71.Morey RA, Haswell CC, Selgrade ES, et al. Effects of chronic mild traumatic brain injury on white matter integrity in Iraq and Afghanistan war veterans. Hum Brain Mapp 2013;34(11):2986–2999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Zhuo J, Xu S, Proctor JL, et al. Diffusion kurtosis as an in vivo imaging marker for reactive astrogliosis in traumatic brain injury. Neuroimage 2012;59(1):467–477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Stokum JA, Sours C, Zhuo J, Kane R, Shanmuganathan K, Gullapalli RP. A longitudinal evaluation of diffusion kurtosis imaging in patients with mild traumatic brain injury. Brain Inj 2015;29(1):47–57. [DOI] [PubMed] [Google Scholar]
- 74.Grossman EJ, Ge Y, Jensen JH, et al. Thalamus and cognitive impairment in mild traumatic brain injury: a diffusional kurtosis imaging study. J Neurotrauma 2012;29(13):2318–2327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Fieremans E, Jensen JH, Helpern JA. White matter characterization with diffusional kurtosis imaging. Neuroimage 2011;58(1):177–188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Lui YW, Xue Y, Kenul D, Ge Y, Grossman RI, Wang Y. Classification algorithms using multiple MRI features in mild traumatic brain injury. Neurology 2014;83(14):1235–1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Wolff SD, Balaban RS. Magnetization transfer contrast (MTC) and tissue water proton relaxation in vivo. Magn Reson Med 1989;10(1):135–144. [DOI] [PubMed] [Google Scholar]
- 78.Dousset V, Grossman RI, Ramer KN, et al. Experimental allergic encephalomyelitis and multiple sclerosis: lesion characterization with magnetization transfer imaging. Radiology 1992;182(2):483–491. [DOI] [PubMed] [Google Scholar]
- 79.Lexa FJ, Grossman RI, Rosenquist AC. Dyke Award paper. MR of wallerian degeneration in the feline visual system: characterization by magnetization transfer rate with histopathologic correlation. AJNR Am J Neuroradiol 1994;15(2):201–212. [PMC free article] [PubMed] [Google Scholar]
- 80.Loevner LA, Grossman RI, Cohen JA, Lexa FJ, Kessler D, Kolson DL. Microscopic disease in normal-appearing white matter on conventional MR images in patients with multiple sclerosis: assessment with magnetization-transfer measurements. Radiology 1995;196(2):511–515. [DOI] [PubMed] [Google Scholar]
- 81.Bagley LJ, McGowan JC, Grossman RI, et al. Magnetization transfer imaging of traumatic brain injury. J Magn Reson Imaging 2000;11(1):1–8. [DOI] [PubMed] [Google Scholar]
- 82.Hofman PA, Verhey FR, Wilmink JT, Rozendaal N, Jolles J. Brain lesions in patients visiting a memory clinic with postconcussional sequelae after mild to moderate brain injury. J Neuropsychiatry Clin Neurosci 2002;14(2):176–184. [DOI] [PubMed] [Google Scholar]
- 83.McGowan JC, Yang JH, Plotkin RC, et al. Magnetization transfer imaging in the detection of injury associated with mild head trauma. AJNR Am J Neuroradiol 2000;21(5):875–880. [PMC free article] [PubMed] [Google Scholar]
- 84.Narayana PA, Yu X, Hasan KM, et al. Multi-modal MRI of mild traumatic brain injury. Neuroimage Clin 2015;7:87–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Haacke EM, Mittal S, Wu Z, Neelavalli J, Cheng YC. Susceptibility-weighted imaging: technical aspects and clinical applications, part 1. AJNR Am J Neuroradiol 2009;30(1):19–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Mittal S, Wu Z, Neelavalli J, Haacke EM. Susceptibility-weighted imaging: technical aspects and clinical applications, part 2. AJNR Am J Neuroradiol 2009;30(2):232–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Beauchamp MH, Ditchfield M, Babl FE, et al. Detecting traumatic brain lesions in children: CT versus MRI versus susceptibility weighted imaging (SWI). J Neurotrauma 2011;28(6):915–927. [DOI] [PubMed] [Google Scholar]
- 88.Sigmund GA, Tong KA, Nickerson JP, Wall CJ, Oyoyo U, Ashwal S. Multimodality comparison of neuroimaging in pediatric traumatic brain injury. Pediatr Neurol 2007;36(4):217–226. [DOI] [PubMed] [Google Scholar]
- 89.Ashwal S, Babikian T, Gardner-Nichols J, Freier MC, Tong KA, Holshouser BA. Susceptibility-weighted imaging and proton magnetic resonance spectroscopy in assessment of outcome after pediatric traumatic brain injury. Arch Phys Med Rehabil 2006;87(12 Suppl 2):S50–S58. [DOI] [PubMed] [Google Scholar]
- 90.Hasiloglu ZI, Albayram S, Selcuk H, et al. Cerebral microhemorrhages detected by susceptibility-weighted imaging in amateur boxers. AJNR Am J Neuroradiol 2011;32(1):99–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Park JH, Park SW, Kang SH, Nam TK, Min BK, Hwang SN. Detection of traumatic cerebral microbleeds by susceptibility-weighted image of MRI. J Korean Neurosurg Soc 2009;46(4):365–369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Benson RR, Gattu R, Sewick B, et al. Detection of hemorrhagic and axonal pathology in mild traumatic brain injury using advanced MRI: implications for neurorehabilitation. NeuroRehabilitation 2012;31(3):261–279. [DOI] [PubMed] [Google Scholar]
- 93.Nisenbaum EJ, Novikov DS, Lui YW. The presence and role of iron in mild traumatic brain injury: an imaging perspective. J Neurotrauma 2014;31(4):301–307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Onyszchuk G, LeVine SM, Brooks WM, Berman NE. Post-acute pathological changes in the thalamus and internal capsule in aged mice following controlled cortical impact injury: a magnetic resonance imaging, iron histochemical, and glial immunohistochemical study. Neurosci Lett 2009;452(2):204–208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Raz E, Jensen JH, Ge Y, et al. Brain iron quantification in mild traumatic brain injury: a magnetic field correlation study. AJNR Am J Neuroradiol 2011;32(10):1851–1856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Jensen JH, Chandra R, Ramani A, et al. Magnetic field correlation imaging. Magn Reson Med 2006;55(6):1350–1361. [DOI] [PubMed] [Google Scholar]
- 97.Connor JR. Iron transport proteins in the diseased brain. J Neurol Sci 2003;207(1-2):112–113. [DOI] [PubMed] [Google Scholar]
- 98.Campbell A, Smith MA, Sayre LM, Bondy SC, Perry G. Mechanisms by which metals promote events connected to neurodegenerative diseases. Brain Res Bull 2001;55(2):125–132. [DOI] [PubMed] [Google Scholar]
- 99.McAllister TW, Saykin AJ, Flashman LA, et al. Brain activation during working memory 1 month after mild traumatic brain injury: a functional MRI study. Neurology 1999;53(6):1300–1308. [DOI] [PubMed] [Google Scholar]
- 100.Chen CJ, Wu CH, Liao YP, et al. Working memory in patients with mild traumatic brain injury: functional MR imaging analysis. Radiology 2012;264(3):844–851. [DOI] [PubMed] [Google Scholar]
- 101.Chen JK, Johnston KM, Frey S, Petrides M, Worsley K, Ptito A. Functional abnormalities in symptomatic concussed athletes: an fMRI study. Neuroimage 2004;22(1):68–82. [DOI] [PubMed] [Google Scholar]
- 102.Christodoulou C, DeLuca J, Ricker JH, et al. Functional magnetic resonance imaging of working memory impairment after traumatic brain injury. J Neurol Neurosurg Psychiatry 2001;71(2):161–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Newsome MR, Scheibel RS, Steinberg JL, et al. Working memory brain activation following severe traumatic brain injury. Cortex 2007;43(1):95–111. [DOI] [PubMed] [Google Scholar]
- 104.Schlösser RG, Wagner G, Sauer H. Assessing the working memory network: studies with functional magnetic resonance imaging and structural equation modeling. Neuroscience 2006;139(1):91–103. [DOI] [PubMed] [Google Scholar]
- 105.Gosselin N, Bottari C, Chen JK, et al. Electrophysiology and functional MRI in post-acute mild traumatic brain injury. J Neurotrauma 2011;28(3):329–341. [DOI] [PubMed] [Google Scholar]
- 106.Keightley ML, Saluja RS, Chen JK, et al. A functional magnetic resonance imaging study of working memory in youth after sports-related concussion: is it still working? J Neurotrauma 2014;31(5):437–451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Smits M, Dippel DW, Houston GC, et al. Postconcussion syndrome after minor head injury: brain activation of working memory and attention. Hum Brain Mapp 2009;30(9):2789–2803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Fischer BL, Parsons M, Durgerian S, et al. Neural activation during response inhibition differentiates blast from mechanical causes of mild to moderate traumatic brain injury. J Neurotrauma 2014;31(2):169–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Stulemeijer M, Vos PE, van der Werf S, van Dijk G, Rijpkema M, Fernández G. How mild traumatic brain injury may affect declarative memory performance in the post-acute stage. J Neurotrauma 2010;27(9):1585–1595. [DOI] [PubMed] [Google Scholar]
- 110.McAllister TW, Flashman LA, McDonald BC, Saykin AJ. Mechanisms of working memory dysfunction after mild and moderate TBI: evidence from functional MRI and neurogenetics. J Neurotrauma 2006;23(10):1450–1467. [DOI] [PubMed] [Google Scholar]
- 111.Mayer AR, Mannell MV, Ling J, et al. Auditory orienting and inhibition of return in mild traumatic brain injury: a FMRI study. Hum Brain Mapp 2009;30(12):4152–4166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Witt ST, Lovejoy DW, Pearlson GD, Stevens MC. Decreased prefrontal cortex activity in mild traumatic brain injury during performance of an auditory oddball task. Brain Imaging Behav 2010;4(3-4):232–247. [DOI] [PubMed] [Google Scholar]
- 113.Barkhof F, Haller S, Rombouts SA. Resting-state functional MR imaging: a new window to the brain. Radiology 2014;272(1):29–49. [DOI] [PubMed] [Google Scholar]
- 114.Boly M, Phillips C, Tshibanda L, et al. Intrinsic brain activity in altered states of consciousness: how conscious is the default mode of brain function? Ann N Y Acad Sci 2008;1129:119–129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Hillary FG, Slocomb J, Hills EC, et al. Changes in resting connectivity during recovery from severe traumatic brain injury. Int J Psychophysiol 2011;82(1):115–123. [DOI] [PubMed] [Google Scholar]
- 116.Sharp DJ, Beckmann CF, Greenwood R, et al. Default mode network functional and structural connectivity after traumatic brain injury. Brain 2011;134(Pt 8):2233–2247. [DOI] [PubMed] [Google Scholar]
- 117.Vanhaudenhuyse A, Noirhomme Q, Tshibanda LJ, et al. Default network connectivity reflects the level of consciousness in non-communicative brain-damaged patients. Brain 2010;133(Pt 1):161–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Mayer AR, Mannell MV, Ling J, Gasparovic C, Yeo RA. Functional connectivity in mild traumatic brain injury. Hum Brain Mapp 2011;32(11):1825–1835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Zhou Y, Milham MP, Lui YW, et al. Default-mode network disruption in mild traumatic brain injury. Radiology 2012;265(3):882–892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Johnson B, Zhang K, Gay M, et al. Alteration of brain default network in subacute phase of injury in concussed individuals: resting-state fMRI study. Neuroimage 2012;59(1):511–518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Zhang K, Johnson B, Gay M, et al. Default mode network in concussed individuals in response to the YMCA physical stress test. J Neurotrauma 2012;29(5):756–765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Slobounov SM, Gay M, Zhang K, et al. Alteration of brain functional network at rest and in response to YMCA physical stress test in concussed athletes: RsFMRI study. Neuroimage 2011;55(4):1716–1727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Vidal-Piñeiro D, Valls-Pedret C, Fernández-Cabello S, et al. Decreased Default Mode Network connectivity correlates with age-associated structural and cognitive changes. Front Aging Neurosci 2014;6:256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Yang AC, Huang CC, Yeh HL, et al. Complexity of spontaneous BOLD activity in default mode network is correlated with cognitive function in normal male elderly: a multiscale entropy analysis. Neurobiol Aging 2013;34(2):428–438. [DOI] [PubMed] [Google Scholar]
- 125.Ding X, Li CY, Wang QS, et al. Patterns in default-mode network connectivity for determining outcomes in cognitive function in acute stroke patients. Neuroscience 2014;277:637–646. [DOI] [PubMed] [Google Scholar]
- 126.Park JY, Kim YH, Chang WH, et al. Significance of longitudinal changes in the default-mode network for cognitive recovery after stroke. Eur J Neurosci 2014;40(4):2715–2722. [DOI] [PubMed] [Google Scholar]
- 127.Disbrow EA, Carmichael O, He J, et al. Resting state functional connectivity is associated with cognitive dysfunction in non-demented people with Parkinson’s disease. J Parkinsons Dis 2014;4(3):453–465. [DOI] [PubMed] [Google Scholar]
- 128.Sours C, Zhuo J, Janowich J, Aarabi B, Shanmuganathan K, Gullapalli RP. Default mode network interference in mild traumatic brain injury: a pilot resting state study. Brain Res 2013;1537:201–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Vakhtin AA, Calhoun VD, Jung RE, Prestopnik JL, Taylor PA, Ford CC. Changes in intrinsic functional brain networks following blast-induced mild traumatic brain injury. Brain Inj 2013;27(11):1304–1310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Sours C, Rosenberg J, Kane R, et al. Associations between interhemispheric functional connectivity and the Automated Neuropsychological Assessment Metrics (ANAM) in civilian mild TBI. Brain Imaging Behav 2015;9(2):190–203. [Published correction appears in Brain Imaging Behav 2015;9(2):353–354.] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Tang L, Ge Y, Sodickson DK, et al. Thalamic resting-state functional networks: disruption in patients with mild traumatic brain injury. Radiology 2011;260(3):831–840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Zhou Y, Lui YW, Zuo XN, et al. Characterization of thalamo-cortical association using amplitude and connectivity of functional MRI in mild traumatic brain injury. J Magn Reson Imaging 2014;39(6):1558–1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Bassett DS, Bullmore E. Small-world brain networks. Neuroscientist 2006;12(6):512–523. [DOI] [PubMed] [Google Scholar]
- 134.Shumskaya E, Andriessen TM, Norris DG, Vos PE. Abnormal whole-brain functional networks in homogeneous acute mild traumatic brain injury. Neurology 2012;79(2):175–182. [DOI] [PubMed] [Google Scholar]
- 135.Jünger EC, Newell DW, Grant GA, et al. Cerebral autoregulation following minor head injury. J Neurosurg 1997;86(3):425–432. [DOI] [PubMed] [Google Scholar]
- 136.Strebel S, Lam AM, Matta BF, Newell DW. Impaired cerebral autoregulation after mild brain injury. Surg Neurol 1997;47(2):128–131. [DOI] [PubMed] [Google Scholar]
- 137.Garnett MR, Blamire AM, Corkill RG, et al. Abnormal cerebral blood volume in regions of contused and normal appearing brain following traumatic brain injury using perfusion magnetic resonance imaging. J Neurotrauma 2001;18(6):585–593. [DOI] [PubMed] [Google Scholar]
- 138.Liu W, Wang B, Wolfowitz R, et al. Perfusion deficits in patients with mild traumatic brain injury characterized by dynamic susceptibility contrast MRI. NMR Biomed 2013;26(6):651–663. [DOI] [PubMed] [Google Scholar]
- 139.Ge Y, Patel MB, Chen Q, et al. Assessment of thalamic perfusion in patients with mild traumatic brain injury by true FISP arterial spin labelling MR imaging at 3T. Brain Inj 2009;23(7):666–674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Grossman EJ, Jensen JH, Babb JS, et al. Cognitive impairment in mild traumatic brain injury: a longitudinal diffusional kurtosis and perfusion imaging study. AJNR Am J Neuroradiol 2013;34(5):951–957, S1–S3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Gowda NK, Agrawal D, Bal C, et al. Technetium Tc-99m ethyl cysteinate dimer brain single-photon emission CT in mild traumatic brain injury: a prospective study. AJNR Am J Neuroradiol 2006;27(2):447–451. [PMC free article] [PubMed] [Google Scholar]
- 142.Raji CA, Tarzwell R, Pavel D, et al. Clinical utility of SPECT neuroimaging in the diagnosis and treatment of traumatic brain injury: a systematic review. PLoS One 2014;9(3):e91088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Abdel-Dayem HM, Abu-Judeh H, Kumar M, et al. SPECT brain perfusion abnormalities in mild or moderate traumatic brain injury. Clin Nucl Med 1998;23(5):309–317. [DOI] [PubMed] [Google Scholar]
- 144.Uruma G, Hashimoto K, Abo M. A new method for evaluation of mild traumatic brain injury with neuropsychological impairment using statistical imaging analysis for Tc-ECD SPECT. Ann Nucl Med 2013;27(3):187–202. [DOI] [PubMed] [Google Scholar]
- 145.Metting Z, Cerliani L, Rödiger LA, van der Naalt J. Pathophysiological concepts in mild traumatic brain injury: diffusion tensor imaging related to acute perfusion CT imaging. PLoS One 2013;8(5):e64461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Metting Z, Rödiger LA, Stewart RE, Oudkerk M, De Keyser J, van der Naalt J. Perfusion computed tomography in the acute phase of mild head injury: regional dysfunction and prognostic value. Ann Neurol 2009;66(6):809–816. [DOI] [PubMed] [Google Scholar]
- 147.Metting Z, Rödiger LA, de Jong BM, Stewart RE, Kremer BP, van der Naalt J. Acute cerebral perfusion CT abnormalities associated with posttraumatic amnesia in mild head injury. J Neurotrauma 2010;27(12):2183–2189. [DOI] [PubMed] [Google Scholar]
- 148.Bartnik-Olson BL, Holshouser B, Wang H, et al. Impaired neurovascular unit function contributes to persistent symptoms after concussion: a pilot study. J Neurotrauma 2014;31(17):1497–1506. [DOI] [PubMed] [Google Scholar]
- 149.Govindaraju V, Gauger GE, Manley GT, Ebel A, Meeker M, Maudsley AA. Volumetric proton spectroscopic imaging of mild traumatic brain injury. AJNR Am J Neuroradiol 2004;25(5):730–737. [PMC free article] [PubMed] [Google Scholar]
- 150.Sivák Š, Bittšanský M, Grossmann J, et al. Clinical correlations of proton magnetic resonance spectroscopy findings in acute phase after mild traumatic brain injury. Brain Inj 2014;28(3):341–346. [DOI] [PubMed] [Google Scholar]
- 151.Cohen BA, Inglese M, Rusinek H, Babb JS, Grossman RI, Gonen O. Proton MR spectroscopy and MRI-volumetry in mild traumatic brain injury. AJNR Am J Neuroradiol 2007;28(5):907–913. [PMC free article] [PubMed] [Google Scholar]
- 152.Gardner A, Iverson GL, Stanwell P. A systematic review of proton magnetic resonance spectroscopy findings in sport-related concussion. J Neurotrauma 2014;31(1):1–18. [DOI] [PubMed] [Google Scholar]
- 153.Kirov II, Tal A, Babb JS, Lui YW, Grossman RI, Gonen O. Diffuse axonal injury in mild traumatic brain injury: a 3D multivoxel proton MR spectroscopy study. J Neurol 2013;260(1):242–252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Johnson B, Gay M, Zhang K, et al. The use of magnetic resonance spectroscopy in the subacute evaluation of athletes recovering from single and multiple mild traumatic brain injury. J Neurotrauma 2012;29(13):2297–2304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Johnson B, Zhang K, Gay M, et al. Metabolic alterations in corpus callosum may compromise brain functional connectivity in MTBI patients: an 1H-MRS study. Neurosci Lett 2012;509(1):5–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Henry LC, Tremblay S, Boulanger Y, Ellemberg D, Lassonde M. Neurometabolic changes in the acute phase after sports concussions correlate with symptom severity. J Neurotrauma 2010;27(1):65–76. [DOI] [PubMed] [Google Scholar]
- 157.Vagnozzi R, Signoretti S, Cristofori L, et al. Assessment of metabolic brain damage and recovery following mild traumatic brain injury: a multicentre, proton magnetic resonance spectroscopic study in concussed patients. Brain 2010;133(11):3232–3242. [DOI] [PubMed] [Google Scholar]
- 158.Vagnozzi R, Signoretti S, Tavazzi B, et al. Temporal window of metabolic brain vulnerability to concussion: a pilot 1H-magnetic resonance spectroscopic study in concussed athletes–part III. Neurosurgery 2008;62(6):1286–1295; discussion 1295–1296. [DOI] [PubMed] [Google Scholar]
- 159.Sarmento E, Moreira P, Brito C, Souza J, Jevoux C, Bigal M. Proton spectroscopy in patients with post-traumatic headache attributed to mild head injury. Headache 2009;49(9):1345–1352. [DOI] [PubMed] [Google Scholar]
- 160.Lin AP, Liao HJ, Merugumala SK, Prabhu SP, Meehan WP, 3rd, Ross BD. Metabolic imaging of mild traumatic brain injury. Brain Imaging Behav 2012;6(2):208–223. [DOI] [PubMed] [Google Scholar]
- 161.Kirov II, Tal A, Babb JS, et al. Proton MR spectroscopy correlates diffuse axonal abnormalities with post-concussive symptoms in mild traumatic brain injury. J Neurotrauma 2013;30(13):1200–1204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Mountford CE, Stanwell P, Lin A, Ramadan S, Ross B. Neurospectroscopy: the past, present and future. Chem Rev 2010;110(5):3060–3086. [DOI] [PubMed] [Google Scholar]
- 163.Gasparovic C, Yeo R, Mannell M, et al. Neurometabolite concentrations in gray and white matter in mild traumatic brain injury: an 1H-magnetic resonance spectroscopy study. J Neurotrauma 2009;26(10):1635–1643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Yeo RA, Gasparovic C, Merideth F, Ruhl D, Doezema D, Mayer AR. A longitudinal proton magnetic resonance spectroscopy study of mild traumatic brain injury. J Neurotrauma 2011;28(1):1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Vagnozzi R, Signoretti S, Floris R, et al. Decrease in N-acetylaspartate following concussion may be coupled to decrease in creatine. J Head Trauma Rehabil 2013;28(4):284–292. [DOI] [PubMed] [Google Scholar]
- 166.George EO, Roys S, Sours C, et al. Longitudinal and prognostic evaluation of mild traumatic brain injury: a 1H-magnetic resonance spectroscopy study. J Neurotrauma 2014;31(11):1018–1028. [DOI] [PubMed] [Google Scholar]
- 167.Garnett MR, Blamire AM, Rajagopalan B, Styles P, Cadoux-Hudson TA. Evidence for cellular damage in normal-appearing white matter correlates with injury severity in patients following traumatic brain injury: a magnetic resonance spectroscopy study. Brain 2000;123(Pt 7):1403–1409. [DOI] [PubMed] [Google Scholar]
- 168.Kierans AS, Kirov II, Gonen O, et al. Myoinositol and glutamate complex neurometabolite abnormality after mild traumatic brain injury. Neurology 2014;82(6):521–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Henry LC, Tremblay S, Leclerc S, et al. Metabolic changes in concussed American football players during the acute and chronic post-injury phases. BMC Neurol 2011;11:105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.Shutter L, Tong KA, Holshouser BA. Proton MRS in acute traumatic brain injury: role for glutamate/glutamine and choline for outcome prediction. J Neurotrauma 2004;21(12):1693–1705. [DOI] [PubMed] [Google Scholar]
- 171.Ashwal S, Holshouser B, Tong K, et al. Proton spectroscopy detected myoinositol in children with traumatic brain injury. Pediatr Res 2004;56(4):630–638. [DOI] [PubMed] [Google Scholar]
- 172.Humayun MS, Presty SK, Lafrance ND, et al. Local cerebral glucose abnormalities in mild closed head injured patients with cognitive impairments. Nucl Med Commun 1989;10(5):335–344. [DOI] [PubMed] [Google Scholar]
- 173.Ruff RM, Crouch JA, Tröster AI, et al. Selected cases of poor outcome following a minor brain trauma: comparing neuropsychological and positron emission tomography assessment. Brain Inj 1994;8(4):297–308. [DOI] [PubMed] [Google Scholar]
- 174.Gross H, Kling A, Henry G, Herndon C, Lavretsky H. Local cerebral glucose metabolism in patients with long-term behavioral and cognitive deficits following mild traumatic brain injury. J Neuropsychiatry Clin Neurosci 1996;8(3):324–334. [DOI] [PubMed] [Google Scholar]
- 175.Umile EM, Sandel ME, Alavi A, Terry CM, Plotkin RC. Dynamic imaging in mild traumatic brain injury: support for the theory of medial temporal vulnerability. Arch Phys Med Rehabil 2002;83(11):1506–1513. [DOI] [PubMed] [Google Scholar]
- 176.Chen SH, Kareken DA, Fastenau PS, Trexler LE, Hutchins GD. A study of persistent post-concussion symptoms in mild head trauma using positron emission tomography. J Neurol Neurosurg Psychiatry 2003;74(3):326–332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 177.Yang ST, Hsiao IT, Hsieh CJ, et al. Accumulation of amyloid in cognitive impairment after mild traumatic brain injury. J Neurol Sci 2015;349(1-2):99–104. [DOI] [PubMed] [Google Scholar]
- 178.Kim N, Branch CA, Kim M, Lipton ML. Whole brain approaches for identification of microstructural abnormalities in individual patients: comparison of techniques applied to mild traumatic brain injury. PLoS One 2013;8(3):e59382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 179.Matthews SC, Strigo IA, Simmons AN, O’Connell RM, Reinhardt LE, Moseley SA. A multimodal imaging study in U.S. veterans of Operations Iraqi and Enduring Freedom with and without major depression after blast-related concussion. Neuroimage 2011;54(Suppl 1):S69–S75. [DOI] [PubMed] [Google Scholar]
- 180.Costanzo ME, Chou YY, Leaman S, et al. Connecting combat-related mild traumatic brain injury with posttraumatic stress disorder symptoms through brain imaging. Neurosci Lett 2014;577:11–15. [DOI] [PubMed] [Google Scholar]
- 181.Kou Z, Gattu R, Kobeissy F, et al. Combining biochemical and imaging markers to improve diagnosis and characterization of mild traumatic brain injury in the acute setting: results from a pilot study. PLoS One 2013;8(11):e80296. [DOI] [PMC free article] [PubMed] [Google Scholar]