

Abstract
Background
This article provides a summary of the 2013 European Renal Association–European Dialysis and Transplant Association (ERA-EDTA) Registry Annual Report (available at http://www.era-edta-reg.org), with a focus on patients with diabetes mellitus (DM) as the cause of end-stage renal disease (ESRD).
Methods
In 2015, the ERA-EDTA Registry received data on renal replacement therapy (RRT) for ESRD from 49 national or regional renal registries in 34 countries in Europe and bordering the Mediterranean Sea. Individual patient data were provided by 31 registries, while 18 registries provided aggregated data. The total population covered by the participating registries comprised 650 million people.
Results
In total, 72 933 patients started RRT for ESRD within the countries and regions reporting to the ERA-EDTA Registry, resulting in an overall incidence of 112 per million population (pmp). The overall prevalence on 31 December 2013 was 738 pmp (n = 478 990). Patients with DM as the cause of ESRD comprised 24% of the incident RRT patients (26 pmp) and 17% of the prevalent RRT patients (122 pmp). When compared with the USA, the incidence of patients starting RRT pmp secondary to DM in Europe was five times lower and the incidence of RRT due to other causes of ESRD was two times lower. Overall, 19 426 kidney transplants were performed (30 pmp). The 5-year adjusted survival for all RRT patients was 60.9% [95% confidence interval (CI) 60.5–61.3] and 50.6% (95% CI 49.9–51.2) for patients with DM as the cause of ESRD.
Keywords: end-stage renal disease, incidence, prevalence, renal replacement therapy, survival
Introduction
The European Renal Association–European Dialysis and Transplant Association (ERA-EDTA) Registry collects data on renal replacement therapy (RRT) for end-stage renal disease (ESRD) via national and regional renal registries in Europe and from countries bordering the Mediterranean Sea. Each year an annual report is produced, presenting an overview of the incidence and prevalence of RRT, kidney transplant activity and the survival of patients on RRT in Europe. With this article, we aim to provide a summary of the 2013 Annual Report of the ERA-EDTA Registry [1]. Both the Annual Report and slides summarizing the Annual Report are available at http://www.era-edta-reg.org. This article specifically focuses on the most common cause of ESRD in the Western world: diabetes mellitus (DM).
Methods
In 2015, the ERA-EDTA Registry received 2013 data from 49 national and regional renal registries in 34 countries in Europe and those bordering the Mediterranean Sea. The majority of renal registries (31 of 49) contributed individual patient data, whereas the other 18 renal registries contributed aggregated data (Figure 1).
Fig. 1.
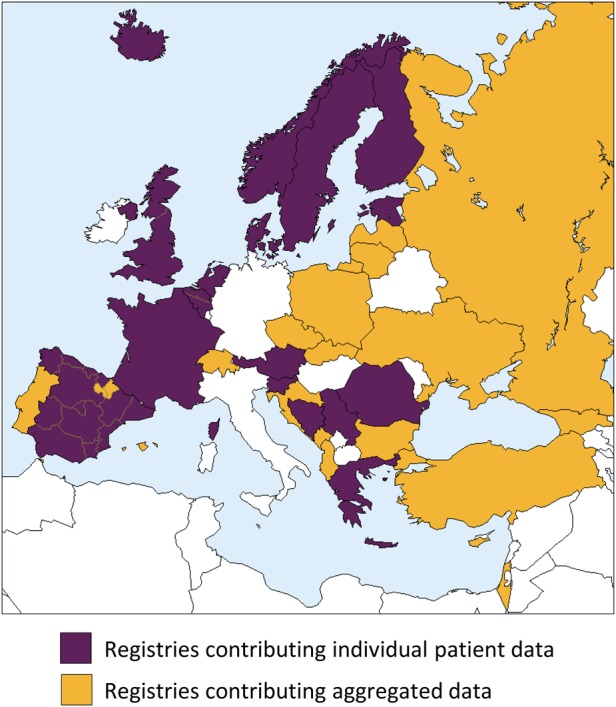
Renal registries from countries and regions in Europe and bordering the Mediterranean Sea that contributed individual patient data or aggregated data to the ERA-EDTA Registry for 2013.
While a standard Microsoft Excel template was used for the collection of aggregated data, the individual patient data were received in different formats, including SPSS, Microsoft Excel and SAS. Extensive data checking was performed and the data were converted to a standard format in order to be stored in a relational database. After data analysis, the results were checked by the participating renal registries. All registry-specific results in the ERA-EDTA Registry Annual Report were approved by the registries before publication.
Mid-year population data for the contributing countries/regions were received from Eurostat (http://ec.europa.eu/eurostat), the national bureau of statistics or the renal registry.
The incidence of RRT was defined as the number of patients starting RRT in one year (2013) and the prevalence of RRT as the number of patients alive and receiving RRT on 31 December 2013. Incidence and prevalence per million population (pmp) were calculated by dividing the observed count by the mid-year population. Time trends of the incidence rates were analysed using Joinpoint regression, with the trends presented as annual percentage change (APC) [2, 3].
Patient survival on RRT, on dialysis and following kidney transplantation was analysed using data from renal registries providing individual patient data for the period 2004–13. A detailed description of the survival methods is given in the Appendix.
Patients were included in the DM subgroup if they were registered as having DM type 1 or type 2 as the cause of ESRD (ERA-EDTA primary renal disease 1995 codes 80 or 81 or ERA-EDTA primary renal disease 2012 codes 2316, 2328, 2337 or 2344 [1]). As information on DM as comorbidity is not routinely collected by the ERA-EDTA Registry, this article only focuses on DM as the cause of ESRD.
Statistical methods
Within this article, patient survival on RRT and following kidney transplantation was analysed using the Kaplan–Meier method and Cox proportional hazards regression. For dialysis patients, kidney transplantation is an event that competes with death. Therefore, we used the cumulative incidence competing risk method for the estimation of the unadjusted cause-specific death probabilities, and the Fine and Gray method for the adjusted cause-specific death probabilities [7]. For the calculation of patient survival on RRT and on dialysis, the date of RRT initiation was the starting point and death was the event studied. Censored observations were recovery of renal function, loss to follow-up and end of the follow-up period (31 December 2013). For analysis of patient survival following kidney transplantation, the date of the first kidney transplant was defined as the first day of follow-up and death was the event studied. Reasons for censoring were loss to follow-up and end of the follow-up period. RRT and dialysis survival probabilities were adjusted for fixed values for age (60 years), gender (60% men) and the cause of ESRD distribution (20% DM, 17% hypertension/renal vascular disease, 15% glomerulonephritis and 48% other causes of ESRD). Transplantation survival probabilities were adjusted for the following values: age 45 years, 60% men, 10% DM, 8% hypertension/renal vascular disease, 28% glomerulonephritis and 54% other causes of ESRD. For the adjusted survival probabilities of the DM subgroup, the corresponding fixed values were used with the exception of the cause of ESRD distribution.
Results
For the majority of renal registries contributing data to the ERA-EDTA Registry, the coverage of the population was 100%, with the exception of Croatia (80%), Latvia (80%), Serbia (94%), Switzerland (94%), Spain (95%), Poland (95%), Georgia (96%), Bulgaria (97%), Czech Republic (98%) and Romania (99%). The total population covered by the participating registries comprised 650 million people. The proportion of the European population covered by the ERA-EDTA Registry in 2013 was 73.6%. A list of the European countries with available data and those without is provided in the Appendix.
Incidence of RRT in 2013
In 2013, a total of 72 933 patients started RRT for ESRD in all the registries reporting to the ERA-EDTA Registry, resulting in an overall incidence of 112 pmp (Figure 2). For countries/regions providing individual patient data (left panel), the overall incidence at Day 1 was 135 pmp, while it was 98 pmp for countries providing aggregated data (right panel). The lowest incidence rates were found in Montenegro (27 pmp), Ukraine (30 pmp) and Russia (50 pmp), whereas the highest rates were observed in Greece (216 pmp) and both parts of Belgium (Dutch-speaking part: 187 pmp, French-speaking part: 183 pmp). Figure 2 also shows the contribution of DM as the cause of ESRD to the incidence of RRT. Overall, patients who had DM as the cause of ESRD comprised 24% of the incident patients (26 pmp). For 48% of those patients, the type of DM was unknown (12 pmp), while 12% (3 pmp) had DM type 1 and 40% (10 pmp) had DM type 2. Among countries/regions whose registries provide individual patient data, the incidence of RRT for ESRD secondary to DM ranged between 12 pmp in Iceland and 58 pmp in Greece. However, in countries with a high proportion of patients with an unknown or missing cause of ESRD, the proportion of patients with DM as the cause of ESRD may be underestimated, as DM may be the cause of ESRD in some of these patients. For this reason, we also report the incidence of RRT for ESRD due to unknown or missing causes of ESRD, which varied widely between 0 pmp in Estonia and 73 pmp in Greece. Countries providing aggregated data showed a greater difference in the incidence of RRT secondary to DM, ranging from 5 pmp in Ukraine to 83 pmp in Israel. In general, countries/regions with a high overall incidence of RRT also had a high incidence of RRT for ESRD secondary to DM.
Fig. 2.

Unadjusted incidence of RRT pmp at Day 1 in 2013 by cause of ESRD. Data are from renal registries providing individual patient data (left panel) and from renal registries providing aggregated data (right panel). Data for Bulgaria, the Czech Republic, Lithuania, Slovakia and Switzerland only include dialysis patients. Registries from Dutch- and French-speaking Belgium, the Spanish regions of Cantabria, Castile and León and Castile-La Mancha and the UK (England, Northern Ireland and Wales) do not report on patients <20 years of age.
Table 1 shows the unadjusted incidence of RRT pmp on Day 91 after the onset of RRT by established treatment modality (haemodialysis, peritoneal dialysis and kidney transplantation). Overall, most patients were treated with haemodialysis (99 pmp in renal registries providing individual patient data and 137 pmp in those providing aggregated data), whereas the incidence of peritoneal dialysis was much lower (19 and 10 pmp, respectively). The incidence of kidney transplantation on Day 91 was highest in The Netherlands (17 pmp) and Norway (15 pmp), whereas it was lowest in Bosnia and Herzegovina and the Spanish region of Extremadura (0 pmp in both cases). Table 2 presents the percentages of established treatment modalities on Day 91 after the start of RRT for all patients, for patients with DM, for patients with other causes of ESRD and for patients with an unknown cause of ESRD. Patients with DM were more often treated with any type of dialysis on Day 91 after the start of RRT than patients with other causes of ESRD (98 versus 93%), while they were less often transplanted (2 versus 7%).
Table 1.
Unadjusted incidence of RRT pmp for ESRD at Day 91 by established modality in 2013 for countries/regions providing individual patient data and for countries providing aggregated data
| All (pmp) | HD (pmp) | PD (pmp) | Tx (pmp) | Other (pmp) | |
|---|---|---|---|---|---|
| Countries/regions providing individual patient data | |||||
| Austriaa | 132.1 | 113.0 | 13.5 | 5.6 | 0 |
| Belgium | |||||
| Dutch-speakingb | 168.4 | 146.2 | 18.4 | 3.8 | 0 |
| French-speakingb | 164.9 | 140.2 | 19.5 | 5.3 | 0 |
| Bosnia and Herzegovina | 110.0 | 106.3 | 3.7 | 0 | 0 |
| Denmark | 109.7 | 66.1 | 34.4 | 8.8 | 0.4 |
| Estonia | 59.9 | 44.0 | 12.1 | 3.8 | 0 |
| Finland | 85.7 | 57.5 | 27.4 | 0.7 | 0 |
| France | 145.9 | 121.3 | 17.5 | 6.5 | 0.6 |
| Greece | 194.4 | 179.9 | 13.9 | 0.5 | 0 |
| Iceland | 74.1 | 30.9 | 34.0 | 9.3 | 0 |
| Norway | 96.1 | 59.5 | 22.0 | 14.6 | 0 |
| Romania | 130.5 | 122.0 | 6.9 | 1.5 | 0 |
| Serbia | 136.9 | 117.0 | 17.2 | 2.7 | 0 |
| Slovenia | 114.6 | 101.5 | 11.2 | 1.9 | 0 |
| Spain | |||||
| Andalusia | 122.2 | 95.7 | 21.1 | 5.4 | 0 |
| Aragon | 125.1 | 95.9 | 26.2 | 3.0 | 0 |
| Asturiasa | 149.2 | 100.5 | 45.6 | 3.1 | 0 |
| Basque country | 114.6 | 71.8 | 32.2 | 10.6 | 0 |
| Cantabriab | 83.2 | 54.3 | 22.1 | 6.8 | 0 |
| Castile and Leónb | 106.5 | 85.0 | 18.3 | 3.2 | 0 |
| Castile-La Manchab | 103.6 | 76.7 | 23.5 | 3.4 | 0 |
| Cataloniaa | 139.3 | 106.6 | 20.0 | 12.8 | 0 |
| Community of Madrid | 117.3 | 92.4 | 17.4 | 7.5 | 0 |
| Extremaduraa | 119.6 | 102.1 | 17.5 | 0.0 | 0 |
| Galicia | 139.8 | 99.8 | 31.6 | 8.3 | 0 |
| Region of Murcia | 103.9 | 78.8 | 23.8 | 1.4 | 0 |
| Valencia Region | 130.0 | 99.9 | 28.6 | 1.6 | 0 |
| Sweden | 104.2 | 57.5 | 37.7 | 9.0 | 0 |
| The Netherlands | 108.4 | 73.8 | 17.7 | 16.8 | 0 |
| UK | |||||
| Englanda,b | 103.3 | 71.1 | 21.1 | 11.1 | 0 |
| Northern Irelanda,b | 86.4 | 59.9 | 16.6 | 9.8 | 0 |
| Scotland | 91.2 | 69.3 | 14.3 | 7.7 | 0 |
| Walesa,b | 103.7 | 75.6 | 19.2 | 8.9 | 0 |
| All countries | 125.8 | 99.1 | 19.1 | 7.3 | 0.2 |
| Countries providing aggregated patient data | |||||
| Albania | 59.2 | 53.6 | 4.8 | 0.7 | 0 |
| Bulgariac | 132.3 | 128.9 | 3.4 | 0 | |
| Croatia | 133.3 | 123.1 | 9.0 | 1.2 | 0 |
| Cyprus | 175.4 | 145.0 | 24.6 | 5.8 | 0 |
| Czech Republicc | 139.3 | 130.5 | 8.8 | 0 | |
| Georgia | 148.6 | 139.3 | 5.8 | 0.2 | 3.3 |
| Israel | 171.7 | 146.9 | 16.3 | 8.6 | 0 |
| Latvia | 70.6 | 61.2 | 8.7 | 0.6 | 0 |
| Lithuaniac | 106.3 | 99.6 | 6.7 | 0 | |
| Montenegro | 22.6 | 14.5 | 0.0 | 8.1 | 0 |
| Portugald | 218.9 | 198.8 | 19.3 | 0.9 | 0 |
| Slovakiac | 132.4 | 128.6 | 3.9 | 0 | |
| All countries | 148.7 | 136.6 | 10.2 | 1.7 | 0.2 |
The category HD also includes haemofiltration and haemodiafiltration. When cells are left empty, the data are unavailable.
HD: haemodialysis, PD: peritoneal dialysis, Tx: kidney transplant.
aThe incidence at Day 91 is based on patients who started RRT in the first 9 months of 2013.
bPatients <20 years of age are not reported.
cData include dialysis patients only.
dOnly pre-emptive transplantations (at Day 1) are included.
Table 2.
Percentages of established RRT modalities at Day 91, unadjusted, by DM as the cause of ESRD, for countries/regions providing individual patient data
| All |
DM |
Other causes of ESRD |
Unknown/missing cause of ESRD |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HD | PD | Tx | Other | HD | PD | Tx | Other | HD | PD | Tx | Other | HD | PD | Tx | Other | |
| Austriaa | 86 | 10 | 4 | 0 | 89 | 9 | 2 | 0 | 84 | 11 | 5 | 0 | 88 | 8 | 4 | 0 |
| Belgium | ||||||||||||||||
| Dutch-speakingb | 87 | 11 | 2 | 0 | 92 | 7 | 1 | 0 | 85 | 13 | 3 | 0 | 93 | 6 | 1 | 0 |
| French-speakingb | 85 | 12 | 3 | 0 | 90 | 10 | 0 | 0 | 83 | 12 | 4 | 0 | 87 | 9 | 4 | 0 |
| Bosnia and Herzegovina | 97 | 3 | 0 | 0 | 97 | 3 | 0 | 0 | 96 | 4 | 0 | 0 | 97 | 3 | 0 | 0 |
| Denmark | 60 | 31 | 8 | 0 | 67 | 30 | 3 | 0 | 60 | 28 | 12 | 0 | 55 | 41 | 4 | 1 |
| Estonia | 73 | 20 | 6 | 0 | 56 | 38 | 6 | 0 | 78 | 16 | 6 | 0 | 0 | 0 | 0 | 0 |
| Finland | 67 | 32 | 1 | 0 | 66 | 34 | 0 | 0 | 66 | 33 | 2 | 0 | 75 | 25 | 0 | 0 |
| France | 83 | 12 | 4 | 0 | 88 | 10 | 2 | 0 | 82 | 12 | 5 | 0 | 82 | 14 | 4 | 0 |
| Greece | 93 | 7 | 0 | 0 | 91 | 9 | 0 | 0 | 93 | 7 | 0 | 0 | 93 | 6 | 0 | 0 |
| Iceland | 42 | 46 | 13 | 0 | 50 | 25 | 25 | 0 | 44 | 44 | 11 | 0 | 0 | 100 | 0 | 0 |
| Norway | 62 | 23 | 15 | 0 | 69 | 17 | 14 | 0 | 60 | 24 | 16 | 0 | 79 | 21 | 0 | 0 |
| Romania | 94 | 5 | 1 | 0 | 94 | 5 | 0 | 0 | 93 | 5 | 2 | 0 | 94 | 6 | 0 | 0 |
| Serbia | 85 | 13 | 2 | 0 | 78 | 20 | 1 | 0 | 89 | 9 | 2 | 0 | 82 | 17 | 1 | 0 |
| Slovenia | 89 | 10 | 2 | 0 | 89 | 11 | 0 | 0 | 85 | 12 | 3 | 0 | 98 | 2 | 0 | 0 |
| Spain | ||||||||||||||||
| Andalusia | 78 | 17 | 4 | 0 | 83 | 15 | 2 | 0 | 74 | 21 | 5 | 0 | 84 | 12 | 5 | 0 |
| Aragon | 77 | 21 | 2 | 0 | 81 | 17 | 2 | 0 | 71 | 26 | 3 | 0 | 87 | 13 | 0 | 0 |
| Asturiasa | 67 | 31 | 2 | 0 | 45 | 55 | 0 | 0 | 71 | 28 | 1 | 0 | 90 | 0 | 10 | 0 |
| Basque country | 63 | 28 | 9 | 0 | 72 | 26 | 2 | 0 | 65 | 25 | 10 | 0 | 44 | 42 | 14 | 0 |
| Cantabriab | 65 | 27 | 8 | 0 | 77 | 8 | 15 | 0 | 61 | 33 | 6 | 0 | 0 | 0 | 0 | 0 |
| Castile and Leónb | 80 | 17 | 3 | 0 | 88 | 11 | 1 | 0 | 76 | 21 | 4 | 0 | 80 | 16 | 4 | 0 |
| Castile-La Manchab | 74 | 23 | 3 | 0 | 81 | 16 | 4 | 0 | 70 | 26 | 4 | 0 | 78 | 22 | 0 | 0 |
| Cataloniaa | 76 | 14 | 9 | 0 | 82 | 16 | 2 | 0 | 73 | 14 | 13 | 0 | 78 | 14 | 8 | 0 |
| Community of Madrid | 79 | 15 | 6 | 0 | 83 | 15 | 2 | 0 | 74 | 16 | 9 | 0 | 86 | 10 | 4 | 0 |
| Extremaduraa | 85 | 15 | 0 | 0 | 82 | 18 | 0 | 0 | 85 | 15 | 0 | 0 | 90 | 9 | 0 | 1 |
| Galicia | 71 | 23 | 6 | 0 | 78 | 22 | 0 | 0 | 63 | 27 | 10 | 0 | 82 | 14 | 3 | 0 |
| Region of Murciaa | 76 | 23 | 1 | 0 | 85 | 15 | 0 | 0 | 72 | 26 | 2 | 0 | 76 | 24 | 0 | 0 |
| Valencia Region | 77 | 22 | 1 | 0 | 82 | 17 | 1 | 0 | 73 | 25 | 2 | 0 | 82 | 18 | 0 | 0 |
| Sweden | 55 | 36 | 9 | 0 | 60 | 36 | 4 | 0 | 53 | 37 | 10 | 0 | 57 | 34 | 8 | 0 |
| The Netherlands | 68 | 16 | 16 | 0 | 82 | 15 | 2 | 0 | 75 | 20 | 6 | 0 | 49 | 11 | 40 | 0 |
| UK | ||||||||||||||||
| Englanda,b | 69 | 20 | 11 | 0 | 76 | 20 | 4 | 0 | 65 | 21 | 14 | 0 | 71 | 20 | 9 | 0 |
| Northern Irelanda,b | 69 | 19 | 11 | 0 | 74 | 23 | 3 | 0 | 69 | 16 | 15 | 0 | 64 | 28 | 8 | 0 |
| Scotland | 76 | 16 | 8 | 0 | 86 | 11 | 3 | 0 | 72 | 17 | 11 | 0 | 78 | 17 | 4 | 0 |
| Walesa,b | 73 | 19 | 9 | 0 | 76 | 18 | 6 | 0 | 69 | 20 | 11 | 0 | 80 | 15 | 6 | 0 |
| All countries | 77 | 16 | 6 | 0 | 82 | 15 | 2 | 0 | 76 | 17 | 7 | 0 | 77 | 15 | 7 | 0 |
The category HD also includes haemofiltration and haemodiafiltration. Categories may not add up because of missing values or rounding off. Percentages are row percentages. When cells are left empty, the data are unavailable.
HD: haemodialysis, PD: peritoneal dialysis, Tx: kidney transplant.
aThe incidence at Day 91 is based on patients who started RRT in the first 9 months of 2013.
bPatients <20 years of age are not reported.
Trends in the incidence of RRT over time in the USA and Europe
Figure 3 shows the trend in the incidence of RRT over the last 10 years, by cause of ESRD, in both Europe and the USA [data extracted from the US Renal Data System (USRDS) Annual Report [4]]. When compared with the USA, the incidence of patients starting RRT for ESRD secondary to DM is almost five times lower in Europe and the incidence of RRT for ESRD due to other causes of ESRD is at least two times lower. Joinpoint regression analyses revealed that in Europe, the incidence of patients starting RRT for ESRD secondary to DM decreased from 2007, although this was not statistically significant {2004–7: APC 1.9 [95% confidence interval (CI) −1.1–+5.1], 2007–13: APC −0.9 [95% CI −1.9–0.2]}. In the USA, the reported incidence of RRT for ESRD secondary to DM remained stable during the last decade [APC 0.2 (95% CI −0.2–0.5)].
Fig. 3.

Unadjusted incidence of RRT pmp at Day 1 by cause of ESRD for the USA [4] and Europe. Data for Europe were based on those renal registries that had individual patient data available from 2004, including Austria, Belgium (Dutch-speaking and French-speaking), Denmark, Finland, Greece, Iceland, Norway, Spain (Andalusia, Aragon, Asturias, Basque country, Cantabria, Castile and León, Castile-La Mancha, Catalonia and Valencia Region), Sweden, The Netherlands and UK (all countries).
Prevalence of RRT on 31 December 2013
Figure 4 shows the unadjusted prevalence of RRT pmp on 31 December 2013, by cause of ESRD. Overall, 477 186 patients were receiving RRT on 31 December 2013, resulting in an overall prevalence of 738 pmp The prevalence was highest in Portugal (1749 pmp), French-speaking Belgium (1270 pmp) and the Spanish region of Catalonia (1262 pmp), whereas it was lowest in Ukraine (159 pmp), Russia (241 pmp) and Montenegro (305 pmp). Patients with DM as the cause of ESRD comprised 17% of the prevalent patients (122 pmp). For 54% of these patients, the type of DM was unknown (66 pmp), while 14% (18 pmp) had DM type 1 and 31% (38 pmp) had DM type 2. In countries/regions with registries providing individual patient data, the overall prevalence of RRT for ESRD secondary to DM was 159 pmp, ranging between 74 pmp in Iceland and 219 pmp in Greece. Tables 3 and 4 present the prevalence by treatment modality (haemodialysis, peritoneal dialysis and kidney transplantation) on 31 December 2013 (pmp and as percentage). In countries/regions with registries providing individual patient data, most prevalent patients were receiving haemodialysis, closely followed by those with a functioning graft. In countries with registries providing aggregated data, the great majority of the patients were receiving haemodialysis. Table 4 shows that in case of patients with DM as the cause of ESRD, only four registries reported ≥50% of patients living with a functioning graft. In contrast, for other causes of ESRD, the vast majority of the registries reported that more than half of the patients had a functioning graft.
Fig. 4.

Unadjusted prevalence of RRT pmp on 31 December 2013 by cause of ESRD. Data are from renal registries providing individual patient data (left panel) and from renal registries providing aggregated data (right panel). Data for Israel, Slovakia and Switzerland only include dialysis patients. For Romania, the overall prevalence of RRT is underestimated by ∼3% due to an estimated 30% underreporting of patients living on a functioning graft. Registries from Dutch- and French-speaking Belgium, the Spanish regions of Cantabria, Castile and León and Castile-La Mancha and the UK (England, Northern Ireland and Wales) do not report on patients <20 years of age.
Table 3.
Unadjusted prevalence of RRT pmp for ESRD on 31 December 2013 by treatment modality for countries/regions providing individual patient data and for countries providing aggregated data
| All (pmp) | HD (pmp) | PD (pmp) | Tx (pmp) | Other (pmp) | |
|---|---|---|---|---|---|
| Countries/regions providing individual patient data | |||||
| Austria | 1053.7 | 471.3 | 49.8 | 532.4 | 0.2 |
| Belgium | |||||
| Dutch-speakinga | 1223.1 | 648.7 | 56.8 | 517.6 | 0 |
| French-speakinga | 1269.9 | 677.6 | 57.5 | 530.6 | 4.2 |
| Bosnia and Herzegovina | 746.9 | 666.5 | 24.2 | 56.2 | 0 |
| Denmark | 876.9 | 354.1 | 95.0 | 424.6 | 3.2 |
| Estonia | 572.1 | 192.7 | 33.4 | 346.0 | 0 |
| Finland | 825.9 | 269.2 | 65.8 | 490.9 | 0 |
| France | 1175.1 | 601.1 | 44.4 | 522.1 | 7.5 |
| Greece | 1172.1 | 871.8 | 61.3 | 239.0 | 0 |
| Iceland | 685.7 | 148.3 | 77.2 | 460.2 | 0 |
| Norway | 900.5 | 212.8 | 39.0 | 648.7 | 0 |
| Romaniab | 816.9 | 676.7 | 75.8 | 64.1 | 0.3 |
| Serbia | 839.1 | 648.2 | 69.9 | 120.4 | 0.6 |
| Slovenia | 1008.3 | 654.9 | 25.2 | 328.2 | 0 |
| Spain | |||||
| Andalusia | 1107.7 | 493.5 | 46.4 | 567.9 | 0 |
| Aragon | 1131.2 | 416.5 | 53.2 | 661.5 | 0 |
| Asturias | 1131.3 | 402.7 | 105.8 | 622.8 | 0 |
| Basque country | 1175.4 | 373.8 | 90.2 | 711.3 | 0 |
| Cantabriaa | 998.5 | 336.2 | 59.4 | 602.9 | 0 |
| Castile and Leóna | 1123.6 | 484.2 | 73.8 | 565.6 | 0 |
| Castile-La Manchaa | 1025.5 | 390.0 | 59.0 | 575.6 | 1.0 |
| Catalonia | 1262.2 | 532.2 | 53.4 | 676.6 | 0 |
| Community of Madrid | 999.3 | 388.7 | 54.3 | 556.2 | 0 |
| Extremadura | 1081.5 | 531.7 | 66.1 | 482.8 | 0.9 |
| Galicia | 1220.9 | 537.6 | 101.3 | 581.9 | 0 |
| Region of Murcia | 1200.4 | 609.4 | 63.9 | 527.2 | 0 |
| Valencia Region | 1232.5 | 651.4 | 77.4 | 502.0 | 1.8 |
| Sweden | 939.5 | 313.2 | 86.8 | 539.5 | 0.1 |
| The Netherlands | 945.4 | 332.0 | 55.2 | 558.2 | 0 |
| UK | |||||
| Englanda | 890.4 | 372.9 | 59.0 | 458.5 | 0 |
| Northern Irelanda | 846.0 | 354.2 | 44.3 | 447.6 | 0 |
| Scotland | 866.0 | 350.4 | 43.4 | 471.9 | 0.4 |
| Walesa | 886.0 | 348.1 | 57.4 | 480.5 | 0 |
| All countries | 1019.8 | 501.0 | 57.5 | 459.3 | 2.0 |
| Countries providing aggregated patient data | |||||
| Albania | 340.5 | 257.1 | 18.0 | 65.4 | 0 |
| Bulgaria | 540.9 | 449.4 | 22.3 | 69.3 | 0 |
| Croatia | 799.5 | 583.3 | 37.1 | 159.9 | 19.3 |
| Czech Republic | 1033.5 | 562.3 | 50.3 | 420.9 | 0 |
| Georgia | 385.2 | 324.1 | 20.8 | 38.5 | 1.9 |
| Israelc | 734.7 | 692.1 | 42.4 | 0.1 | |
| Latvia | 600.3 | 221.8 | 53.7 | 324.8 | 0 |
| Lithuania | 719.0 | 475.4 | 15.8 | 227.8 | 0 |
| Montenegro | 304.8 | 133.9 | 4.8 | 166.1 | 0 |
| Poland | 822.4 | 513.4 | 27.9 | 281.1 | 0 |
| Portugal | 1749.3 | 1046.7 | 69.8 | 632.8 | 0 |
| Russia | 241.4 | 179.8 | 13.8 | 47.8 | 0 |
| Slovakiac | 609.0 | 592.9 | 16.1 | ||
| Spain (18 of 19 regions) | 1125.8 | 482.1 | 62.1 | 579.9 | 1.8 |
| Switzerlandc | 381.6 | 349.5 | 32.0 | 0.1 | |
| Turkey | 870.2 | 687.1 | 59.2 | 123.9 | 0 |
| Ukraine | 159.0 | 117.6 | 21.3 | 20.1 | 0 |
| All countries | 589.6 | 392.4 | 33.4 | 163.3 | 0.4 |
The category HD also includes haemofiltration and haemodiafiltration. When cells are left empty, the data are unavailable.
HD: haemodialysis, PD: peritoneal dialysis, Tx: kidney transplant.
aPatients <20 years of age are not reported.
bThe overall prevalence of RRT is underestimated by ∼3% due to an estimated 30% underreporting of patients living with a functioning graft.
cData include dialysis patients only.
Table 4.
Percentages of RRT modalities among prevalent patients on 31 December 2013, unadjusted, by DM as the cause of ESRD for countries/regions providing individual patient data
| All |
DM |
Other causes of ESRD |
Unknown/missing cause of ESRD |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HD | PD | Tx | Other | HD | PD | Tx | Other | HD | PD | Tx | Other | HD | PD | Tx | Other | |
| Austria | 45 | 5 | 51 | 0 | 60 | 4 | 36 | 0 | 40 | 5 | 55 | 0 | 45 | 5 | 50 | 0 |
| Belgium | ||||||||||||||||
| Dutch-speakinga | 53 | 5 | 42 | 0 | 71 | 4 | 25 | 0 | 48 | 5 | 47 | 0 | 57 | 2 | 41 | 0 |
| French-speakinga | 53 | 5 | 42 | 0 | 71 | 5 | 23 | 0 | 50 | 4 | 45 | 0 | 44 | 5 | 51 | 0 |
| Bosnia and Herzegovina | 89 | 3 | 8 | 0 | 92 | 5 | 3 | 0 | 89 | 3 | 8 | 0 | 87 | 2 | 11 | 0 |
| Denmark | 40 | 11 | 48 | 0 | 54 | 13 | 33 | 0 | 36 | 9 | 55 | 0 | 44 | 15 | 41 | 0 |
| Estonia | 34 | 6 | 60 | 0 | 26 | 10 | 64 | 0 | 36 | 5 | 60 | 0 | 0 | 0 | 0 | 0 |
| Finland | 33 | 8 | 59 | 0 | 40 | 10 | 50 | 0 | 26 | 6 | 67 | 0 | 56 | 12 | 32 | 0 |
| France | 51 | 4 | 44 | 1 | 73 | 5 | 22 | 0 | 47 | 3 | 49 | 1 | 51 | 5 | 43 | 1 |
| Greece | 74 | 5 | 20 | 0 | 89 | 7 | 4 | 0 | 68 | 5 | 27 | 0 | 77 | 5 | 19 | 0 |
| Iceland | 22 | 11 | 67 | 0 | 29 | 13 | 58 | 0 | 20 | 10 | 70 | 0 | 29 | 29 | 43 | 0 |
| Norway | 24 | 4 | 72 | 0 | 34 | 4 | 63 | 0 | 22 | 4 | 74 | 0 | 42 | 5 | 54 | 0 |
| Romaniab | 83 | 9 | 8 | 0 | 86 | 11 | 3 | 0 | 81 | 9 | 9 | 0 | 84 | 9 | 7 | 0 |
| Serbia | 77 | 8 | 14 | 0 | 77 | 16 | 7 | 0 | 78 | 7 | 15 | 0 | 73 | 9 | 17 | 0 |
| Slovenia | 65 | 3 | 33 | 0 | 86 | 3 | 11 | 0 | 59 | 2 | 39 | 0 | 70 | 2 | 27 | 0 |
| Spain | ||||||||||||||||
| Andalusia | 45 | 4 | 51 | 0 | 63 | 6 | 31 | 0 | 39 | 4 | 57 | 0 | 50 | 3 | 47 | 0 |
| Aragon | 37 | 5 | 58 | 0 | 57 | 6 | 37 | 0 | 36 | 4 | 60 | 0 | 24 | 4 | 72 | 0 |
| Asturias | 36 | 9 | 55 | 0 | 46 | 18 | 36 | 0 | 32 | 8 | 60 | 0 | 39 | 6 | 55 | 0 |
| Basque country | 32 | 8 | 61 | 0 | 56 | 12 | 32 | 0 | 27 | 7 | 67 | 0 | 38 | 11 | 52 | 0 |
| Cantabriaa | 34 | 6 | 60 | 0 | 50 | 6 | 44 | 0 | 31 | 6 | 63 | 0 | 36 | 0 | 64 | 0 |
| Castile and Leóna | 43 | 7 | 50 | 0 | 60 | 7 | 32 | 0 | 45 | 8 | 47 | 0 | 29 | 3 | 68 | 0 |
| Castile-La Manchaa | 38 | 6 | 56 | 0 | 57 | 7 | 35 | 0 | 33 | 6 | 61 | 0 | 39 | 4 | 57 | 0 |
| Catalonia | 42 | 4 | 54 | 0 | 63 | 6 | 31 | 0 | 34 | 3 | 62 | 0 | 51 | 5 | 43 | 0 |
| Community of Madrid | 39 | 5 | 56 | 0 | 57 | 7 | 36 | 0 | 33 | 6 | 61 | 0 | 43 | 3 | 54 | 0 |
| Extremadura | 49 | 6 | 45 | 0 | 76 | 7 | 17 | 0 | 43 | 7 | 50 | 0 | 46 | 4 | 50 | 0 |
| Galicia | 44 | 8 | 48 | 0 | 63 | 11 | 26 | 0 | 37 | 8 | 56 | 0 | 49 | 9 | 42 | 0 |
| Region of Murcia | 51 | 5 | 44 | 0 | 71 | 6 | 23 | 0 | 46 | 6 | 48 | 0 | 52 | 4 | 44 | 0 |
| Valencia Region | 53 | 6 | 41 | 0 | 71 | 7 | 22 | 0 | 47 | 6 | 46 | 0 | 59 | 6 | 35 | 0 |
| Sweden | 33 | 9 | 57 | 0 | 45 | 12 | 43 | 0 | 29 | 8 | 63 | 0 | 43 | 12 | 45 | 0 |
| The Netherlands | 35 | 6 | 59 | 0 | 55 | 7 | 38 | 0 | 33 | 6 | 62 | 0 | 32 | 5 | 63 | 0 |
| UK | ||||||||||||||||
| Englanda | 42 | 7 | 51 | 0 | 59 | 9 | 32 | 0 | 37 | 6 | 58 | 0 | 45 | 8 | 47 | 0 |
| Northern Irelanda | 42 | 5 | 53 | 0 | 66 | 6 | 28 | 0 | 36 | 5 | 59 | 0 | 46 | 9 | 45 | 0 |
| Scotland | 40 | 5 | 54 | 0 | 59 | 6 | 35 | 0 | 35 | 5 | 60 | 0 | 48 | 5 | 47 | 0 |
| Walesa | 39 | 6 | 54 | 0 | 55 | 7 | 39 | 0 | 34 | 7 | 60 | 0 | 46 | 5 | 49 | 0 |
| All countries | 49 | 6 | 45 | 0 | 66 | 8 | 27 | 0 | 45 | 5 | 50 | 0 | 51 | 6 | 41 | 0 |
The category HD also includes haemofiltration and haemodiafiltration. When cells are left empty, the data are unavailable.
HD: haemodialysis, PD: peritoneal dialysis, Tx: kidney transplant.
aPatients <20 years of age are not reported.
bThe overall prevalence of RRT is underestimated by ∼3% due to an estimated 30% underreporting of patients living with a functioning graft.
Kidney transplants performed in 2013
Figure 5 shows the kidney transplant rate in 2013 for countries/regions whose registries provide individual patient data and for countries whose registries provide aggregated patient data, by donor type. Overall, 19 426 kidney transplantations were performed (30 pmp), of which 6002 (9 pmp) transplants came from living donors, 13 207 (20 pmp) from deceased donors and 217 (0.3 pmp) from an unknown donor source. The three Spanish regions—Cantabria (104 pmp), Basque country (75 pmp) and Catalonia (71 pmp)—had the highest kidney transplant rates, while Ukraine (3 pmp), Albania (3 pmp) and Russia (7 pmp) showed the lowest rates. The highest living donor kidney transplant rates were found in The Netherlands (31 pmp), Turkey (31 pmp) and Cyprus (27 pmp).
Fig. 5.

Kidney transplants pmp performed in 2013, unadjusted. Data are from renal registries providing individual patient data (left panel) and aggregated data (right panel). For Slovakia, data were obtained from the Slovak Centre of Organ Transplantation, and for Spain (18 of 19 regions), from the Organización Nacional de Transplantes. For Romania, the kidney transplantation activity reflects 70% of the total kidney transplantation activity in the country due to an underreporting of pre-emptive kidney transplantations. Registries from Dutch- and French-speaking Belgium, the Spanish regions of Cantabria, Castile and León and Castile-La Mancha and the UK (England, Northern Ireland and Wales) do not report on patients <20 years of age.
Patient survival
Survival analyses included data from 22 registries in 11 countries, which provided individual patient data for the period of 2004–11. Table 5 shows the unadjusted and adjusted survival probabilities for patients starting RRT or dialysis or receiving their first kidney transplant between 2004 and 2008. In order to present more recent survival data, 1- and 2-year survival probabilities are also presented, for patients starting RRT/dialysis or receiving their first kidney transplant between 2007 and 2011. The survival of patients with DM as the cause of ESRD was worse when compared with the total group of patients starting RRT, dialysis or receiving a kidney transplant. Two-year survival probabilities were higher for patients starting RRT, dialysis or receiving a kidney transplant between 2007 and 2011 than between 2004 and 2008.
Table 5.
One-, 2- and 5-year unadjusted and adjusted patient survival probabilities (in %) with 95% confidence interval for all patients and for patients with DM as the cause of ESRD
| 2004–8 period |
2007–11 period |
||||
|---|---|---|---|---|---|
| 1 year | 2 year | 5 year | 1 year | 2 year | |
| Patient survival on RRT | |||||
| Unadjusted | |||||
| All | 82.1 (81.9–82.3) | 71.2 (71.0–71.4) | 48.3 (48.2–48.5) | 83.5 (83.3–83.7) | 73.1 (72.9–73.3) |
| DM | 82.3 (81.8–82.7) | 68.8 (68.4–69.2) | 40.2 (39.9–40.4) | 83.9 (83.5–84.3) | 71.1 (70.7–71.5) |
| Adjusteda | |||||
| All | 89.2 (89.0–89.3) | 81.4 (81.1–81.7) | 60.9 (60.5–61.3) | 90.0 (89.8–90.2) | 82.7 (82.5–83.0) |
| DM | 87.8 (87.4–88.1) | 77.3 (76.8–77.8) | 50.6 (49.9–51.2) | 89.0 (88.7–89.4) | 79.4 (78.9–79.9) |
| Patient survival on dialysis (with kidney transplantation as competing event) | |||||
| Unadjusted | |||||
| All | 81.6 (81.4–81.8) | 70.5 (70.3–70.8) | 48.1 (47.9–48.4) | 82.8 (82.6–83.0) | 72.1 (71.9–72.3) |
| DM | 82.0 (81.6–82.4) | 68.6 (68.2–69.0) | 40.6 (40.1–41.1) | 83.5 (83.2–83.9) | 70.6 (70.1–71.1) |
| Adjusteda | |||||
| All | 89.4 (89.3–89.6) | 81.9 (81.7–82.1) | 62.4 (62.2–62.8) | 89.9 (90.0–89.8) | 82.6 (82.8–82.4) |
| DM | 87.3 (87.1–87.5) | 78.5 (78.2–78.8) | 56.6 (56.2–57.0) | 88.5 (88.6–88.3) | 80.2 (80.5–80.0) |
| Patient survival after first kidney transplantation (deceased donor) | |||||
| Unadjusted | |||||
| All | 95.7 (95.4–96.0) | 93.7 (93.4–94.1) | 87.1 (86.7–87.5) | 96.0 (95.7–96.2) | 94.0 (93.6–94.3) |
| DM | 93.9 (93.0–94.7) | 91.3 (90.3–92.2) | 81.6 (80.3–82.7) | 94.8 (94.0–95.4) | 92.2 (91.3–93.0) |
| Adjusteda | |||||
| All | 97.4 (97.2–97.6) | 96.1 (95.9–96.4) | 91.8 (91.4–92.2) | 97.6 (97.4–97.8) | 96.4 (96.1–96.6) |
| DM | 95.8 (95.1–96.4) | 93.8 (93.1–94.6) | 86.5 (85.4–87.7) | 96.5 (95.9–97.0) | 94.7 (94.0–95.4) |
| Patient survival after first kidney transplantation (living donor) | |||||
| Unadjusted | |||||
| All | 98.3 (98.0–98.6) | 97.4 (97.0–97.8) | 94.3 (93.7–94.8) | 98.6 (98.3–98.8) | 97.6 (97.3–97.9) |
| DM | 96.3 (94.2–97.6) | 93.4 (90.9–95.2) | 85.3 (82.3–87.8) | 96.8 (95.3–97.9) | 94.9 (93.0–96.2) |
| Adjusteda | |||||
| All | 98.7 (98.4–99.0) | 98.1 (97.7–98.4) | 95.6 (95.0–96.1) | 99.1 (98.9–99.3) | 98.4 (98.2–98.7) |
| DM | 97.5 (96.4–98.7) | 95.6 (94.0–97.2) | 89.8 (87.5–92.3) | 98.1 (97.3–98.9) | 96.9 (95.8–98.0) |
Based on data from Austria, Belgium (Dutch-speaking and French-speaking), Denmark, Finland, Greece, Iceland, Norway, Spain (Andalusia, Aragon, Asturias, Basque country, Cantabria, Castile and León, Castile-La Mancha, Catalonia, Extremadura and Valencia Region), Sweden, The Netherlands and UK (all countries).
aAdjusted survival probabilities were adjusted for age, gender and cause of ESRD. For the adjusted survival probabilities of the DM subgroup, only age and gender were taken into account.
Paediatric patients
For children, we performed a separate analysis of the incidence and prevalence by age group using data from 25 national or regional renal registries from 16 countries that provided individual paediatric data. In 2012–13, 686 children [7.5 per million age-related population (pmarp)] started RRT. Of these children, 135 (6.0 pmarp) were <5 years of age at the onset of RRT, 96 (4.2 pmarp) were ages 5–9 years, 175 (7.7 pmarp) were ages 10–14 years and 280 (12.1 pmarp) were ages 15–19 years. On 31 December 2013, 2529 (55.3 pmarp) children were receiving RRT, of whom 203 (18.0 pmarp) were <5 years of age, 423 (36.6 pmarp) were ages 5–9 years, 686 (60.2 pmarp) were ages 10–14 years and 1217 (105.9 pmarp) were ages 15–19 years.
A more detailed overview of the paediatric RRT data in Europe can be found at the ESPN/ERA-EDTA Registry website (http://www.espn-reg.org).
Discussion
This summary of the 2013 ERA-EDTA Registry Annual Report includes data from 49 national and regional renal registries in 34 countries in Europe and bordering the Mediterranean Sea, with a special focus on patients receiving RRT for ESRD secondary to DM.
Both the overall incidence of RRT for ESRD and the incidence of RRT for ESRD secondary to DM were substantially lower in Europe than in the USA [4]. However, even in Europe and among countries bordering the Mediterranean Sea, there were notable differences in the incidence of RRT for ESRD secondary to DM. This variation may be explained in part by differences in the prevalence of DM within the general population [5], differences in preventive measures, such as lifestyle advice and the use of renoprotective medication, and differences in macroeconomic factors and nephrology services [6]. It should be noted that this variation may also be influenced by discrepancies in the proportion of patients coded with a missing or unknown cause of ESRD. Nevertheless, in view of the ongoing epidemic of DM in Western societies [5], it is remarkable that both in Europe and in the USA, the rise in the incidence of RRT for ESRD secondary to DM appears to have subsided.
Although patients receiving RRT for ESRD secondary to DM were less likely to receive a kidney transplant and had worse survival compared with the overall group, their survival seems to be improving with time.
In conclusion, we have shown encouraging results for patients receiving RRT for ESRD secondary to DM. This suggests that advances in health care have been effective with regard to the prevention and management of ESRD secondary to DM.
Affiliated registries
Albania: N. Thereska, A. Strakosha and N. Pasko; Austria: R. Kramar; Belgium, Dutch-speaking: B. De Moor, F. Schroven and J. De Meester; Belgium, French-speaking: J.M. des Grottes and F. Collart; Bosnia-Herzegovina: H. Resić, B. Prnjavorac and N. Petković; Bulgaria: E. Vazelov and V. Mushekov; Croatia: I. Bubić, S. Rački and N. Janković; Cyprus: K. Ioannou and all of the renal units providing data; Czech Republic: I. Rychlík, J. Potucek and F. Lopot; Denmark: J.G. Heaf; Estonia: Ü. Pechter, M. Rosenberg and K. Lilienthal; Finland: P. Finne and C. Grönhagen-Riska; France: M. Lassalle and C. Couchoud; Georgia: N. Kantaria and Dialysis Nephrology and Transplantation Union of Georgia; Greece: N. Afentakis; Iceland: R. Palsson; Israel: R. Dichtiar, T. Shohat and E. Golan; Latvia: H. Cernevskis and V. Kuzema; Lithuania: V. Kuzminskis, I.A. Bumblytė and E. Žiginskienė; Montenegro: M. Ratkovic, D Radunovic and S. Ivanovic; Norway: T. Leivestad; Poland: B. Rutkowski, G. Korejwo and P. Jagodziński; Portugal: F. Macário, F. Nolasco and R. Filipe; Romania: G. Mircescu, L. Garneata and E. Podgoreanu; Russia: B. Bikbov and N. Tomilina; Serbia: working group of the Serbian RRT Registry and all of the Serbian renal units; Slovakia: V. Spustová, I. Lajdova and M. Karolyova; Slovenia: J. Buturovic-Ponikvar, J. Gubenšek and M. Arnol; Spain, Andalusia: P. Castro de la Nuez; Spain, Aragon: J.I. Sanchez Miret and J.M. Abad Diez; Spain, Asturias: R. Alonso de la Torre, J.R. Quirós and the RERCA Working Group; Spain, Basque country: Á. Magaz, J. Aranzabal, M. Rodrigo and I. Moina; Spain, Cantabria: M. Arias Rodríquez and O. García Ruiz; Spain, Castile and León: R. González and C. Fernández-Renedo; Spain, Castile-La Mancha: G. Gutiérrez Ávila and I. Moreno Alía; Spain, Catalonia: E. Arcos, J. Comas and J. Tort; Spain, Community of Madrid: M.I. Aparicio Madre and C. Chamorro Jambrina; Extremadura: J.M. Ramos Aceitero and M.A. García Bazaga; Spain, Galicia: E. Bouzas-Caamaño and J. Sánchez-Ibáñez; Region of Murcia: C. Santiuste de Pablos and I. Marín Sánchez; Spain, Valencia Region: O. Zurriaga Llorens, M. Ferrer Alamar and N. Fuster Camarena; Spain: Spanish RRT National Registry at ONT, Spanish Regional Registries and Spanish Society of Nephrology (SEN); Sweden: K.G. Prütz, M. Stendahl, M. Evans, S. Schön, L. Bäckman and M. Segelmark; Switzerland: P. Ambühl and R. Winzeler; The Netherlands: M. Hemmelder and A. Hemke; Turkey: G. Süleymanlar, N. Seyahi and M.R. Maltiparmak; Ukraine: M. Kolesnyk and S. Nikolaenko; UK, England/Northern Ireland/Wales: all the staff of the UK Renal Registry and of the renal units submitting data; UK, Scotland: all of the Scottish renal units.
ERA-EDTA registry committee members
A. Więcek (ERA-EDTA President); C. Wanner, Germany (Chairman); F.J. Caskey, UK; F. Collart, Belgium; C. Couchoud, France; D. Fouque, France; J.W. Groothoff, The Netherlands; J.G. Heaf, Denmark; P. Ravani, Italy; I. Rychlik, Czech Republic; F. Schaefer, Germany; S. Schön, Sweden.
ERA-EDTA registry office staff
K.J. Jager (Managing Director), M. Bonthuis (for paediatric section), R. Cornet, F.W. Dekker, G. Guggenheim, A. Kramer, M. Noordzij, M. Pippias, V.S. Stel and A.J. Weerstra.
Conflict of interest statement
Acknowledgements
The ERA-EDTA Registry would like to thank the patients and staff of all the dialysis and transplant units who have contributed data via their national and regional renal registries. In addition, we would like to thank the persons and organizations listed in the ‘Affiliated registries’ for their contribution to the work of the ERA-EDTA Registry. The ERA-EDTA Registry is funded by the ERA-EDTA. This article was written by Anneke Kramer et al. on behalf of the ERA-EDTA Registry, which is an official body of the ERA-EDTA, and it was approved by all co-authors.
Appendix
Coverage of the European population by the ERA-EDTA registry
European countries supplying data to the ERA-EDTA Registry in 2013: Albania, Austria, Belgium, Bosnia and Herzegovina, Bulgaria, Croatia, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Georgia, Greece, Iceland, Latvia, Lithuania, Montenegro, the Netherlands, Norway, Poland, Portugal, Romania, Russia, Serbia, Slovakia, Slovenia, Spain, Sweden, Switzerland, Turkey, Ukraine and the UK.
European countries not supplying data to the ERA-EDTA Registry in 2013: Andorra, Armenia, Azerbaijan, Belarus, former Yugoslav Republic of Macedonia, Germany, Hungary, Ireland, Italy, Kosovo (under United Nations Security Council Resolution 1244/99), Liechtenstein, Luxembourg, Malta, Moldova, Monaco and San Marino.
The coverage of the European population by the ERA-EDTA Registry in 2013 was 73.6%. For this calculation, only the proportions of the population residing in the European part of Russia and Turkey were considered.
References
- 1.ERA-EDTA Registry: ERA-EDTA Registry Annual Report 2013. Academic Medical Center, Department of Medical Informatics, Amsterdam, The Netherlands, 2015 [Google Scholar]
- 2.Kim HJ, Fay MP, Feuer EJ et al. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med 2000; 19: 335–351 [DOI] [PubMed] [Google Scholar]
- 3.Kramer A, Stel V, Zoccali C et al. An update on renal replacement therapy in Europe: ERA-EDTA Registry data from 1997 to 2006. Nephrol Dial Transplant 2009; 24: 3557–3566 [DOI] [PubMed] [Google Scholar]
- 4.United States Renal Data System. 2015 annual data report: epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2015
- 5.International Diabetes Federation. IDF Diabetes Atlas 2013. https://www.idf.org/diabetesatlas (19 November 2015, date last accessed)
- 6.Caskey FJ, Kramer A, Elliott RF et al. Global variation in renal replacement therapy for end-stage renal disease. Nephrol Dial Transplant 2011; 26: 2604–2610 [DOI] [PubMed] [Google Scholar]
- 7.Noordzij M, Leffondré K, van Stralen KJ et al. When do we need competing risks methods for survival analysis in nephrology? Nephrol Dial Transplant 2013; 28: 2670–2677 [DOI] [PubMed] [Google Scholar]