

Abstract
Background
Sexual minority youth, especially girls, are at risk for alcohol, cigarette, and marijuana use when these substances are examined individually. However, little is known about concurrent use of these substances (i.e., three-substance use) in relation to sexual orientation.
Objectives
The present study compared profiles of past year alcohol, cigarette, and marijuana use between SMGs and heterosexual girls. In addition, because internalizing and externalizing symptoms are associated with substance use, we examined whether sexual orientation was associated with substance use profile over and above co-occurring psychopathology.
Methods
Mixture modeling was used to identify patterns of alcohol (including binge drinking), cigarette, and marijuana use in the past year using a cross-sectional sample of urban adolescent girls (Pittsburgh Girls Study; N=2064; mean age=17). Approximately 8% (n=173) of the girls endorsed a lesbian or bisexual identity.
Results
Five substance using classes were identified: low-level substance use (72%), marijuana use (5%), cigarette use (8%), alcohol use (8%), and three-substance use (7%). SMGs were at an increased risk for substance use than heterosexual girls, particularly three-substance use (OR=6.69, p<.001), cigarette use (OR=6.26, p<.001), and marijuana use (OR=3.86, p<.001) classes. Substance use patterns were regressed on sexual orientation, internalizing symptoms (i.e., depression, anxiety), and externalizing symptoms (i.e., conduct problems, oppositional defiant disorder). The disparities remained robust after controlling for internalizing and externalizing symptoms.
Conclusions/Importance
Clinicians and researchers should be aware of potential three-substance use among SMGs. Substance use interventions for SMG may benefit from targeting risk factors that cut-across several substances, particularly externalizing symptoms.
Keywords: bisexual, lesbian, substance use, mixture modeling, internalizing, externalizing
Introduction
A growing literature suggests that sexual minority girls (SMG) are at a greater risk for substance use than heterosexual girls (Marshal et al., 2008). A recent comprehensive review of sexual minority health research highlights the continued need for describing health disparities among sexual minorities, particularly during adolescence when these disparities emerge (Institute of Medicine, 2011). Moreover, a recent research priority of the U.S. Department of Health and Human Services includes identifying youth at risk for heavy substance use, such as sexual minority individuals, to inform targeted prevention and intervention efforts (U.S. Department of Health and Human Services, 2012). To address these concerns, the current study focuses on disparities in substance use between sexual minority and heterosexual girls.
“Sexual minority” is a label describing an overarching group including lesbian, gay, and bisexual individuals. On average, sexual minority youth (SMY) report more substance use than heterosexual youth (Marshal et al., 2008). A meta-analysis showed that SMY report nearly 3 times more substance use than heterosexual youth (Marshal et al., 2008), including tobacco (Austin et al., 2004; Cochran, Stewart, Ginzler, & Cauce, 2002; Lampinen, McGhee, & Martin, 2006), alcohol (Robin et al., 2002; Smith, Lindsay, & Rosenthaly, 1999; Whitbeck, Chen, Hoyt, Tyler, & Johnson, 2004), and marijuana use (Cochran et al., 2002; Lampinen et al., 2006; Rostosky, Owens, Zimmerman, & Riggle, 2003). These disparities were at least twice as large for SMGs (OR = 5.02) than sexual minority boys (OR = 1.90). Thus, recent studies, although relatively limited in number, have begun to characterize disparities among SMGs. The disparities have been replicated (Hipwell et al. 2013; Marshal et al. 2013b; Marshal et al. 2012b; Marshal et al. 2012a), with SMGs reporting higher levels of past year alcohol (Corliss et al., 2008; Marshal, Sucato, et al., 2012), tobacco (Corliss et al., 2013; Marshal, Dermody, et al., 2013; Marshal, Sucato, et al., 2012), and marijuana use (Corliss et al., 2010; Marshal, Dermody, et al., 2013) than heterosexual girls that persist into young adulthood (Dermody et al., 2014; Marshal, King, et al., 2012). As relatively few studies have focused on the health and wellness of SMGs, additional research is needed to improve understanding of the disparities.
While SMGs are at risk for alcohol, cigarette, and marijuana use independently, these findings may be partially explained by a subset of SMGs who multiple types of or all three substances. It remains unknown if SMGs are at risk for concurrent use of multiple substances relative to heterosexual girls and if multiple substance use is the main source of the SMGs’ heightened risk for substance use in general. Identifying multiple substance use among SMGs is critical because using a combination of tobacco, alcohol, and marijuana places individuals at risk for additional health and social consequences, such as increased likelihood and severity of mental health symptoms, future substance dependence, risk behaviors (e.g., driving under the influence, high school dropout, less condom use), school non-completion, and respiratory problems (Kelly et al., 2015; McKee & Weinberger, 2013; Moss, Chen, & Yi, 2014; Ramo, Liu, & Prochaska, 2012). Thus, comprehensive interventions to address the use of multiple substances may be needed.
To date, the few studies describing multiple drug use have focused almost exclusively on illicit and club drug use by sexual minority adults. These studies examine associations between sexual orientation and count variables of the number of substances used, typically during the past year. It appears that sexual minority adult men (Greenwood et al., 2001; Operario et al., 2006; Thiede et al., 2003) and women (Lea, Reynolds, & de Wit, 2013) are at risk for using multiple illicit substances concurrently (e.g., within the same 1-year period) relative to their heterosexual counterparts. Thus, the present study aims to address a gap in the research literature concerning multiple substance use among SMGs by describing their profiles of alcohol, tobacco, and marijuana use.
Substance use profiles have been described for adolescents as a whole, rather than stratifying them in terms of their sexual orientations. Using mixture modeling, research has identified latent subgroups of adolescents characterized by relative levels of alcohol, cigarette, and marijuana use. The approach has identified a subgroup of adolescents who engage in multiple substance use, representing 8–15% of adolescents in national samples (Conway et al., 2013; Dierker, Vesel, Sledjeski, Costello, & Perrine, 2007). Specifically, in a national cohort of 10th-grade students in the U.S., non-users (59%), alcohol-users (23%), marijuana users (11%) and polysubstance users (8%) were identified (Conway et al., 2013). To our knowledge, concurrent use of alcohol, cigarette, and marijuana use among SMGs has not been described.
Using a sample of urban girls, the present project examined if SMGs are at risk for using multiple substances compared to heterosexual girls. Prior research with the sample identified higher use of any alcohol, cigarettes, or marijuana (examined separately) in the past year among SMGs (Marshal, Dermody, et al., 2013). The present study extends these findings by identifying subgroups of SMGs who show different patterns in using substances, including use of multiple substances, using mixture modeling technique. The strength of mixture modeling is that it is person-centered, which facilitates identifying heterogeneity in substance use patterns and associated risk. Using a subset black and white girls in the present sample, recent research detected a subgroup using a combination of alcohol, tobacco, and marijuana at least once in the past year (Chung, Kim, Hipwell, & Stepp, 2013). The present investigation differs from the prior research in several ways, not limited to the focus on sexual orientation-related disparities and examining the relations between mental health symptoms and substance use patterns. Based on the limited research in the area, it was anticipated that SMGs would be disproportionally represented in each substance use class, including multiple substance users, than heterosexual girls.
Substance Use and Mental Health among SMGs
Internalizing and externalizing symptoms may place SMGs at risk for substance use. According to the minority stress theory, SMY may self-medicate stress using substance use (Meyer, 2003). Specifically, SMYs report experiencing discrimination and victimization related to their minority status (Friedman et al., 2011; Williams, Connolly, Pepler, & Craig, 2005). SMY, particularly SMGs, are at risk for internalizing symptoms such as depression and anxiety compared to heterosexual youth (Bostwick, Boyd, Hughes, & McCabe, 2010; Marshal, Dermody, et al., 2013; Marshal et al., 2011; Marshal, Sucato, et al., 2012). Substance use may be a means to self-medicate negative affective states (Bandura & McClelland, 1977; Cooper, Russell, & George, 1988; Goldbach, Tanner-Smith, Bagwell, & Dunlap, 2014) that result from these negative interpersonal experiences as well as associated mental health symptoms, such as depression and anxiety (Hussong, Jones, Stein, Baucom, & Boeding, 2011). A cross-sectional study of SMGs (n=64) and heterosexual girls (n=92), recruited from medical centers in Pennsylvania and Ohio, suggested that depressive symptoms may mediate the relation between victimization and substance use (Marshal, Burton, Chisolm, Sucato, & Friedman, 2013). Similarly, the minority stress model appears to explain risk for marijuana use among lesbian, gay, and bisexual adolescents (Goldbach et al., 2015). As a result, internalizing symptoms may help explain the link between sexual orientation and substance use.
Socialization Theory also suggests that substance use plays an important role among sexual minority individuals, in that the social networks or communities they affiliate with tend to be more tolerant of drug use (Carpiano, Kelly, Easterbrook, & Parsons, 2011). Associations with deviant peer groups who are more tolerant of drug use may serve as an externalizing pathway for SMY to substance use. Like adolescents who are rejected by their mainstream peers are at risk for forming relationships with deviant peers (Rudolph et al., 2014) and in turn using substances (Dishion, Ha, & Veronneau, 2012), SMY who are victimized or experience peer-rejcetion may similarly be at risk for substance use through their associations with deviant peer groups. While this externalizing pathway has not been emphasized in the disparities literature, substance use is associated with conduct disorder symptoms and oppositional defiant disorder symptoms among heterosexual youth (Fergusson, Horwood, & Ridder, 2007; King, Iacono, & McGue, 2004; Pardini, White, & Stouthamer-Loeber, 2007), and may similarly predict substance use among SMG. As SMGs appear to be at an increased risk for conduct problems compared to heterosexual girls (Marshal, Dermody, et al., 2013; Marshal, Sucato, et al., 2012), we examine the extent to which sexual orientation is associated with substance use over and above co-occurring internalizing and externalizing symptoms.
The present study aims to address a critical gap in knowledge regarding the extent to which concurrent (i.e., within the past year) patterns of substance use differ for SMGs and heterosexual girls. We hypothesized that SMGs will be more likely than heterosexual girls to endorse multiple substance use. As pathways involving internalizing (Meyer, 2003) and externalizing behaviors may be associated with substance use, we also examined the extent to which sexual orientation is associated with substance use profiles over and above internalizing (anxiety, depression) and externalizing (conduct problems, oppositional defiant behaviors) symptoms. We hypothesized that sexual orientation would remain significantly related to substance use profiles over and above internalizing and externalizing mental health symptoms, which would support the unique role of minority sexual orientation as a risk factor for early substance use among adolescent girls.
Methods
Study Participants and Design
The Pittsburgh Girls Study (PGS) is a multiple cohort, prospective study of urban girls designed to investigate the development of conduct problems and substance use. All households in the greater Pittsburgh area were enumerated, and low-income households were oversampled to increase power to examine an at-risk population. Of the 2,876 eligible girls, based on age and being successfully contacted, 2,451 (85.2%) agreed to participate in the longitudinal study (see Keenan et al. 2010; Hipwell et al. 2002 for detailed description of the study design). Since 2000, when the girls were 5–8 years old, assessments were completed annually. The University of Pittsburgh Institutional Review Board approved all study procedures. Prior to data collection, caregivers provided written informed consent and the girls provided verbal and written assent when developmentally appropriate.
At Wave 11, beginning in the Fall 2011, self-reported sexual orientation was added to the battery for all girls. The present study focused on Wave 11 because it was the only available wave that included self-reported sexual orientation. At Wave 11, the girls were 15 – 19 years old and the retention rate was 85.1% (n = 2,086). Of these participants, 7 did not respond to the substance use items and an additional 15 did not respond to the sexual identity item, leaving a final sample size of 2,064 girls for the present analyses. The mean age of the sample examined in these analyses was 17.20 (SD = 1.28) and 39% of the girls identified themselves as Caucasian (2.2% of which were Hispanic (n=18)), 55% were African-American (1.5% Hispanic (n=16)), and 6% were multi-racial or another race (2.7% Hispanic (n=3)). Over half of girls’ parents completed more than 12 years of education (56.3%) and were not receiving public assistance (60.4%). Half of parents were cohabiting with a spouse or partner (50.8%).
Measures
Sexual orientation
Participants responded to the question: “Do you consider yourself to be a) Heterosexual or straight; b) Gay or lesbian; or c) Bisexual?” There were 173 (8.3%) SMGs who identified themselves as lesbian (n = 32) or bisexual (n = 141). Given the small number of lesbian girls, the subgroups were combined into a single SMGs group for the analyses. The SMGs did not significantly differ from the heterosexual girls on demographic or parent characteristics.
Substance use
Girls’ report of substance use frequency in the past year was assessed by the Nicotine, Alcohol, and Drug Use scale adapted from Pandina, Labouvie, and White (1984). Response options were: (0) I did not use within the past year, (1) Less than 5 times in the past year, (2) More than 5 times in the past year, but less than once a month, (3) About once a month, (4) About once a week, (5) A couple times per week, (6) Nearly every day, and (7) Every day or more than once a day. All of the substance use items, except for binge drinking, were treated as continuous in the analyses because they included 8 categories reflecting various degrees of use and research has shown that treating variables with ordered categories as continuous does not introduce substantial biases to the results if the variable has more than 4 or 5 categories (Bollen & Barb, 1981; Johnson & Creech, 1983; Rhemtulla, Brosseau-Liard, & Savalei, 2012; Torra, Domingo-Ferrer, Mateo-Sanz, & Ng, 2006; Zumbo & Zimmerman, 1993). As participants reported the frequency of drinking beer, wine, and liquor separately, the highest reported frequency for beer, wine, or liquor was used to indicate alcohol use frequency. For example, if a participant drank beer more frequently than liquor and wine, then the alcohol use frequency variable would reflect the participant’s frequency of consuming beer. This approach was taken (as opposed to adding the frequencies across the types) because it was unknown if the different alcohol types were used during the same drinking episodes. The occurrence of any binge drinking (i.e., drinking 5 or more drinks in one sitting) during the past year was assessed with an additional yes/no item and was treated as a dichotomous variable.
Mental health symptoms
Variables were self-reported symptom severities in the past year. Externalizing symptoms included oppositional defiant disorder symptoms (ODD) and conduct disorder symptoms (CD). Internalizing symptoms included depression symptoms and anxiety symptoms. ODD, CD, and depression symptom severities were assessed using the Adolescent Self-Report Inventory-4 (ASI-4; 46) through age 17 transitioning to the Adult Self-Report Inventories-4 (ASRI-4; 47) at age 18 years. Responses to questions were assessed on a four-point scale (0 = never to 3 = very often), which were averaged to obtain overall symptom severity scores for each mental health variable. For participants completing the ASI-4 (n = 1536), CD symptom severity scores were an average of 15 items, whereas for participants completing the ASRI-4 (n = 528), 13 items were available to generate a mean score. Similarly, for participants completing the ASI-4, depression severity scores were the average of 11 items, whereas for the ASRI-4, 10 questions were averaged. Anxiety symptoms were operationalized as the total summary score on the Self-Report for Childhood Anxiety Related Disorders (SCARED) (Birmaher et al., 1997).
Statistical analysis
All the analyses were run using Mplus version 7 (Muthén & Muthén, 1998–2012). Missing data on substance use items were handled using robust full information maximum likelihood (FIML) estimation, which estimates model parameters using all available data.
Substance use classes
Mixture modeling was carried out to identify subgroups of individuals based on relative levels of alcohol, cigarette, and marijuana use and the occurrence of binge drinking in the past year. The modeling approach identifies distinct subgroups in the sample based on the patterns of responding to variables (Muthén & Muthén, 1998–2012).
To extract substance use subgroups that were meaningful and fit the data well, two-, three-, four-, five-, and six-class solutions were examined. The class solution that best fit the data was selected using both a recommended a step-wise approach (Nylund, Asparouhov, & Muthén, 2007) and the relative interpretability and parsimony of the identified classes (Lanza & Rhoades, 2013). The step-wise approach involves (1) estimating each group solution separately to determine the lowest, replicable likelihood score and corresponding model fit indices, and (2) using the bootstrap likelihood ratio test (BLRT; McLachlan and Peel 1974) to compare the model fit between models with k and k-1 classes. The model with the lowest AIC and BIC values, highest entropy value, and significant BLRT (p < .05) is preferred (Nylund et al., 2007). With respect to the interpretability of the classes, we followed convention of selecting a solution with at least 5% of the sample allocated to each class (Nagin, 2005). Class membership was regressed on sexual orientation in the models to examine if SMGs are more likely to be in relatively riskier substance use classes compared to heterosexual girls. Chronological age and dichotomous race (0 = Caucasian, 1 = other race) variables were included as covariates. Each racial group included corresponding Hispanic subgroup.
The selected class solution was then used to examine interrelations with mental health symptoms. First, the relations between internalizing and externalizing symptoms with class membership was examined by regressing class membership on each mental health subscale in four models, controlling for covariates. Second, to test if the relation between mental health symptoms and class membership differs based on sexual orientation, moderation analyses were conducted by adding a product term between sexual orientation and the mean-centered mental health variable as an independent variable. Lastly, as internalizing and externalizing symptoms are also known to co-occur (Angold, Costello, & Erkanli, 1999), their associations with the substance use classes were also examined simultaneously in one model to control for the effects of the other mental health symptom subscales and remove potential effect due to the common shared variance between them. The analyses included all but one participant (n = 2063) who did not complete the depression and anxiety subscales.
Results
Substance use classes
The five-class solution was chosen based on model fit and the interpretability of the classes (Table 1). Compared to having fewer classes, the five-class solution had the lowest AIC and BIC. While the entropy value for four-classes was slightly larger (0.995) than the five-classes (0.98), the BLRT indicated the five-class solution should be chosen (p < .001). Despite the six-class solution having relatively better fit, some classes were small (i.e., 2 classes with proportions of 3.5% (n = 73), 4.9% (n = 101)), there was relatively small improvement in AIC and BIC, and no improvement in entropy.
Table 1.
Model fit indices and model comparison statistics for mixture modeling of substance use.
| Class solutions tested | |||||
|---|---|---|---|---|---|
|
| |||||
| 2 | 3 | 4 | 5 | 6 | |
| Log likelihood | −10158 | −9574 | −8720 | −8281 | −8026 |
| AIC | 20346 | 19194 | 17502 | 16639 | 16146 |
| BIC | 20430 | 19323 | 17677 | 16859 | 16410 |
| Entropy | 0.998 | 1.00 | 0.995 | 0.98 | 0.98 |
| Parameters | 15 | 23 | 31 | 39 | 47 |
| BLRT | p < .001 | p < .001 | p < .001 | p < .001 | p < .001 |
The sample size and model estimated mean substance use levels of each class in the 5-class model are summarized in Table 2 and Figure 1. The names of each class refer to the most heavily used substance(s). The largest class (N = 1487, 72%) included individuals reporting little (42%) or no (58%) substance use or binge drinking. Individuals who reported any substance use in this class primarily reported use less than 5 times in the past year (57%). Thus, the class will be called the “low-level substance users.”
Table 2.
Characteristics of five substance use classes and their associations with sexual orientation.
| Total sample (N=2064) | Low-level users (n=1487) | Marijuana users (n=108) | Cigarette users (n=166) | Alcohol users (n=168) | Three-substance users (n=135) | |
|---|---|---|---|---|---|---|
| Model estimated mean (SD)a | ||||||
|
| ||||||
| Cigarette | 0.99(2.22) | 0.06 (.01) | 0.34(.08) | 6.18 (.08) | 0.30(.07) | 6.21(.12) |
| Marijuana | 0.76(1.70) | 0.09 (.01) | 4.56(.13) | 0.61(.09) | 0.52(.07) | 5.50(.14) |
| Alcohol | 0.77(1.24) | 0.25 (.02) | 1.68(.159) | 1.34(.13) | 2.67(.22) | 2.75(.14) |
| Binge drinkingb | 0.17(.04) | 0.02 (.01) | 0.38(.05) | 0.38(.04) | 0.77(.04) | 0.70(.04) |
|
| ||||||
| Observed Proportion of SMGs and Heterosexual Girls in each Classc | ||||||
|
| ||||||
| %SMGs(n) | 100% (173) | 61.3%(106) | 5.8% (10) | 13.9% (24) | 7.5% (13) | 11.6% (20) |
| %Heterosexual(n) | 100%1891 | 73.0%(1381) | 5.2% (98) | 7.5% (142) | 8.2% (155) | 6.1% (115) |
|
| ||||||
| Effects of SMG Status and Covariates (Low-level users as reference group)d | ||||||
|
| ||||||
| SMG status | Reference | 3.86 | 6.26 | 1.87 | 6.69 | |
| Group | (2.40–6.19)*** | (4.22–9.29)*** | (.98–3.57) | (4.35–10.26)*** | ||
| Age | Reference | 2.58 | 2.20 | 1.71 | 1.27 | |
| Group | (2.05–3.25)*** | (1.84–2.63)*** | (1.49–1.97)*** | (1.09–1.49)** | ||
| Race | Reference | 0.24 | 0.62 | 0.39 | 1.82 | |
| Group | (0.16–0.38)*** | (0.42–0.92)* | (0.28–0.55)*** | (1.08–3.07)* | ||
The reported values are estimated means from the Mplus output and can be interpreted as the average response to the substance use items on the 0 – 7 scale. Bolded values are one standard deviation or more above the total sample estimated mean.
Proportion endorsing binge drinking the past year (SD) is reported.
The observed prevalence of each sexual orientation in each class was obtained in SPSS using each participant’s most likely class membership obtained in Mplus.
Results are odds ratios (95% confidence interval) from a multinomial logistic regression of each predictor/covariate on class membership. Variables were entered simultaneously in the model. Each odds ratio represents the odds of SMGs being in each class (i.e., probability of SMGs being in class divided by probability of being in reference group) relative to the odds of heterosexual girls being in the same class.
Note:
Substance use frequency codes: (0) did not use within the past year, (1) Less than 5 times in the past year, (2) More than 5 times in the past year, but less than once a month, (3) About once a month, (4) About once a week, (5) A couple times per week, (6) Nearly every day, and (7) Every day or more than once a day
p < .10,
p < .05,
p < .01,
p < .001.
Figure 1.
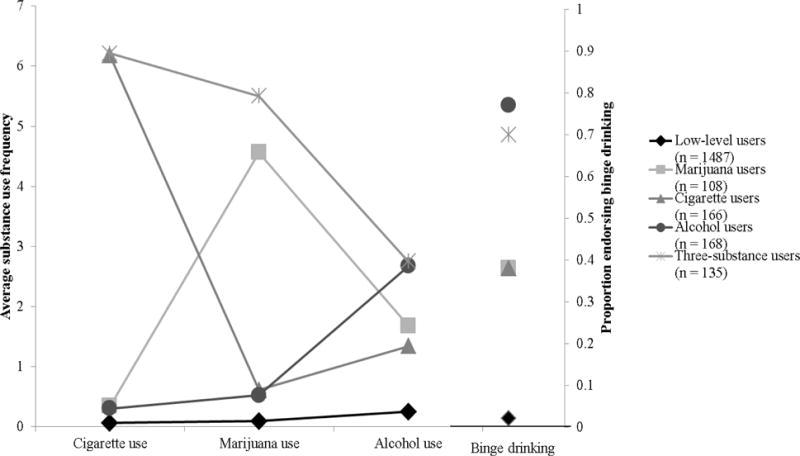
Patterns of cigarette, marijuana, and alcohol use by urban adolescent girls categorized into five substance use classes.
Note:
Substance use frequency codes: (0) did not use within the past year, (1) Less than 5 times in the past year, (2) More than 5 times in the past year, but less than once a month, (3) About once a month, (4) About once a week, (5) A couple times per week, (6) Nearly every day, and (7) Every day or more than once a day
The remaining classes were elevated on at least one substance and binge drinking (i.e., one standard deviation or more above the sample mean). The “marijuana users” class (n = 108; 5%), on average, included individuals who reported marijuana use between weekly or a couple times per week (item responses between 4 and 5). Cigarette or alcohol use levels were relatively low; however, 38% reported binge drinking in the past year. The “cigarette users” class (n = 166; 8%) included girls who typically smoke nearly every day (item response around 6) but had relatively low marijuana and alcohol use. About 38% of girls in the cigarette user class reported binge drinking in the past year. The “alcohol users” class (n = 168; 8%), on average, reported drinking every other month to monthly (item responses between 2 and 3), binge drinking at least once in the past year (77%), and relatively infrequent cigarette and marijuana use. A “three-substance users” group (n = 135, 7%) was also identified and reported elevated use of all substances assessed. Specifically, on average, the three-substance users smoked cigarettes nearly every day (item response around 6), smoked marijuana between a couple times a week and every day (item responses between 5 and 6), drank alcohol almost monthly (item response around 3), and 70% reported binge drinking during the past year.
Sexual orientation and substance use class membership
The associations between SMG status and class membership are summarized in Table 2 by four odds ratios (ORs).1 Each OR is interpreted like a multinomial logistic regression coefficient. Specifically, it indicates the likelihood of SMGs, compared to heterosexual girls, to belong in the class of interest relative to the reference group, i.e., low-level substance users.(Muthén & Muthén, 1998–2012). Compared to heterosexual girls, SMGs are 3.86 times greater higher odds to be in the marijuana users class than to the low-level substance users group (reference group) (OR = 3.86, p < .001) (Table 2). SMGs were also more likely to belong in the cigarette users class (OR = 6.26, p < .001), and three-substance users (OR = 6.69, p < .001) classes than to belong in the low-level substance users, compared to heterosexual girls (Table 2). There was a non-significant trend for disparities in the odds of being alcohol users (OR = 1.87, p = .11) relative to low-level substance users.
The analyses were replicated using the alcohol users class as the reference group, in order to examine the odds of SMGs being classified in a class that primarily used alcohol relative to those reporting predominant use of either marijuana, cigarettes, or both. Compared to heterosexual girls, SMGs were more likely to be cigarette users (OR = 3.34, p < .01) and three-substance users (OR = 3.57, p < .01) than alcohol users. There was a trend for the same effect for marijuana users (OR = 2.06, p = .11).
Covariates and substance use class membership
Older girls had greater odds of being classified in any substance-using classes relative to low-level users class (Table 2 ORs 1.27 – 2.58). Girls of minority race were at risk for three-substance relative to low-level use (OR = 1.82, p < .05), but less likely to be classified in the other substance-using classes (ORs 0.24 – 0.69).
Mental health and substance use class membership
The upper panel of Table 3 summarizes results of the four separate models testing the association between substance use class and SMG status controlling for mental health symptoms. The four models exhibited good model fit (entropy > .97). The classes remained stable after adding the mental health scales. The associations between SMG status and substance use remained robust after controlling for the significant associations between the substance use classes with mental health symptoms.
Table 3.
The associations between mental health symptom severities and membership in substance use classes.
| Dependent Variable: Substance Use Class Membership | |||||
|---|---|---|---|---|---|
|
| |||||
| Marijuana users | Cigarette users | Alcohol users | Three-substance users | ||
| Odds ratio (95% confidence interval) | |||||
|
| |||||
| Model | Effects of Independent Variables (Estimated in Four Separate Models) | ||||
|
| |||||
| 1 | Depression | 1.60(1.39–1.85)*** | 1.28(1.11–1.49)** | 1.32(1.14–1.53)** | 1.56(1.36–1.79)*** |
| SMG status | 3.11(1.91–5.07)*** | 5.55(3.72–8.28)*** | 1.62(0.85–3.08) | 5.34(3.43–8.33)*** | |
|
| |||||
| 2 | Anxiety | .98(0.82–1.16) | .87(0.75–1.01) | 1.01(0.87–1.17) | 1.16(1.01–1.34)† |
| SMG status | 3.88(2.42–6.23)*** | 6.46(4.36–9.57)*** | 1.87(0.98–4.03) | 6.43(4.16–9.95)*** | |
|
| |||||
| 3 | ODD | 2.02(1.74–2.35)*** | 1.69(1.45–1.96)*** | 1.81(1.56–2.09)*** | 2.14(1.85–2.48)*** |
| SMG status | 3.44(2.13–5.78)*** | 5.64(3.77–8.43)*** | 1.65(0.86–3.14) | 5.78(3.72–8.99)*** | |
|
| |||||
| 4 | CD | 2.59(2.19–3.05)*** | 2.37(2.02–2.78)*** | 2.55(2.15–3.03)*** | 3.23(2.82–3.92)*** |
| SMG status | 3.06(1.81–5.15)*** | 5.31(3.54–7.96)*** | 1.62(0.88–2.96) | 4.98(3.10–8.00)*** | |
|
| |||||
| Unique Effects of Independent Variables (Estimated in a Single Model) | |||||
|
| |||||
| 5 | Depression | 1.34(1.10–1.53)* | 1.14(0.95–1.37) | 1.06(0.88–1.28) | 1.15(0.95–1.39) |
| Anxiety | 0.63(0.50–0.80)** | 0.66(0.55–0.79)*** | 0.79(0.66–0.94)* | 0.80(0.66–0.98) † | |
| ODD | 1.43(1.17–1.75)** | 1.31(1.02–1.57)* | 1.36(1.14–1.62)** | 1.31(1.06–1.67)* | |
| CD | 2.19(1.92–2.64)*** | 2.13(1.79–2.55)*** | 2.20(1.81–2.68)*** | 2.88(2.39–3.46)*** | |
| SMG status | 2.84(1.66–4.85)*** | 5.21(3.43–7.91)** | 1.58(0.86–2.90) | 4.75(2.94–7.69)*** | |
Abbreviations: Oppositional defiant disorder symptom severity (ODD), conduct disorder symptom severity (CD), sexual minority girl (SMG).
Note: results are odds ratios (95% confidence interval) relative to membership in the low-level users reference group. Age and race were included as covariates.
p < .10,
p < .05,
p < .01,
p < .001.
Mental health symptoms were associated with substance use class membership. Membership in the three-substance users class over the low-level group was associated with significantly higher levels of depression (OR = 1.56, p < .001), ODD (OR = 2.14, p < .001), and CD (OR = 3.23, p < .001). The same pattern of findings was supported for each of the other substance use classes relative to the low-level substance users class. The relations between mental health symptoms and substance use class membership did not differ based on sexual orientation, as indexed by non-significant interaction terms (all p’s > .10; results not shown).
After the mental health scales were examined simultaneously in a single model (reported in the lower panel of Table 3), the sexual orientation effects remained robust. Despite the moderate correlation between ODD and CD (r = .53), ODD and CD each were associated with a significantly increased risk for membership to all of the substance use classes after controlling for the effect of the other. Depression symptoms were only associated with membership in the marijuana users class (OR = 1.34, p < .05). Anxiety was associated with reduced membership in most of the substance use classes, including marijuana users (OR = 0.63, p < .01), cigarette users (OR = 0.66, p < .001), and alcohol users (OR = 0.79, p < .05) and was marginally related to decreased risk for three-substance use (p < .10).
Discussion
This study identified five profiles of past year alcohol, marijuana and cigarette use, including a subgroup of adolescent girls who reported use of all three substances. On average, girls who reported use of all three substances in the past year smoked cigarettes nearly every day, smoked marijuana several times a week, and engaged in binge drinking. This study adds to the existing disparities literature by finding that SMGs exhibited over a 6-fold risk for using these three substances in the past year than heterosexual girls. The use of all three of these substances, although possibly not occurring on the same occasion, may exacerbate risk for negative outcomes (e.g., McKee & Weinberger, 2013; Ramo et al., 2012), and its prevalence among SMGs warrants targeted intervention efforts.
Consistent with previous research, SMGs were at greater risk for cigarette (Austin et al., 2004; Cochran et al., 2002; Lampinen et al., 2006) or marijuana use (Cochran et al., 2002; Lampinen et al., 2006; Rostosky et al., 2003) than heterosexual girls. SMGs were most highly represented among cigarette users (14%). The nearly daily rate of smoking in this group is troubling as it places SMGs at risk for nicotine dependence in adulthood (Colby, Tiffany, Shiffman, & Niaura, 2000; Corliss et al., 2013; Van De Ven, Greenwood, Engels, Olsson, & Patton, 2010). In contrast, SMGs were not at greater risk than heterosexual girls for mainly using alcohol. SMG disparities were significantly larger when outcomes involved multiple substances compared to alcohol alone. While previous research has described higher drinking levels among SMGs than heterosexual girls, the studies did not account for other substances use (Robin et al., 2002; Smith et al., 1999; Whitbeck et al., 2004). Thus, the present study confirms that SMGs are at risk for heavy drinking, but also adds that the drinking may tend to occur in the context of other substance use. Thus, interventions targeting substance use among SMGs may need to target use of multiple substances, particularly for SMGs who drink heavily.
Another contribution of the present study is the support of independent associations between sexual orientation and substance use over and above mental health symptoms. The substance use disparities were robust even after taking into account concurrent internalizing and externalizing symptoms. The continued associations between sexual orientation and substance use suggest that concurrent mental health symptoms among SMGs do not entirely explain the disparities supported in previous research.
Furthermore, the associations between substance use with mental health symptoms suggest that these outcomes co-occur among SMGs. Externalizing symptoms, including conduct disorder and oppositional defiant disorder symptoms, were consistently associated with alcohol, marijuana, or cigarette use and three-substance use even after taking into account coexisting internalizing symptoms. The strength of these relations did not differ based on sexual orientation. While internalizing symptoms were associated with substance use risk, the effects were relatively weak and inconsistent after taking into account externalizing symptoms. Furthermore, in some contexts, anxiety symptoms were associated with less substance use, which has been shown in previous research (e.g., Pardini et al. 2007). To date, the associations between externalizing symptoms and substance use have not been emphasized as strongly as the internalizing pathway implicated by the minority stress model. The present study suggests that substance use may frequently co-occur with conduct problems among SMGs and that the pathway warrants further study.
The results of the present study should be interpreted in light of some limitations. First, while there was support for a three-substance using group, the current study cannot speak to the extent to which these substances were used concurrently in a year versus simultaneously in a substance using episode. Additional illicit substances were not examined due to the low base rate of use. Given the cross-sectional nature of the study, the findings do not describe how these processes unfold over time or in younger adolescents, and causal inferences cannot be made. For example, it is unknown if the mental health symptoms contribute to or result from the substance use, or both. Taking a developmental prospective would be valuable to explore how these processes unfold over time and may be interrelated. Finally, while a strength of the present study is examining the role of sexual orientation using a relatively large number of SMGs compared to many investigations (n = 173), the number of SMGs in some substance using classes was relatively small and may not be representative of SMGs nationally. For example, bisexual girls were more represented among the SMGs than lesbian girls in the present study; whereas, in nationally representative samples like Add Health, bisexual and lesbian girls tend to be more equally represented (i.e., 2.1% and 1.7%, respectively; Dermody et al., 2014). This could impact results as bisexual girls may be at higher risk of substance use than lesbian girls (e.g., Marshal et al., 2008), although this was not seen in the present sample. The robust disparities despite the relatively small numbers of SMGs in some classes suggests that multiple substance use among SMGs warrants further study.
It is important to note that, despite the observed disparities, a sizable group of SMGs (61%) exhibited minimal substance use (compared to 73% of heterosexual girls). This low-level group tends to be overlooked, but could provide valuable insight about protective factors to be targeted by interventions. For instance, factors not examined in the present study, like social support (Doty, Willoughby, Lindahl, & Malik, 2010) and community connectedness (Saewyc et al., 2009), could buffer the SMGs from the effects of victimization and bullying, and, in turn, prevent heavy substance use. Future research of SMGs is needed to examine protective factors for substance use.
The present study emphasizes the heterogeneity of substance use patterns and risk among SMGs. Using a relatively large and diverse sample of girls, a subset of SMGs was identified who engage in heavy substance use, including use of multiple substances within a year. These substance use patterns place them at risk for adverse health outcomes. Importantly, SM status was uniquely associated with substance use profiles, over and above mental health symptoms, suggesting the important role of sexual orientation in risk for substance use among girls. To our knowledge, few interventions have been implemented to ameliorate these substance use disparities, particularly multiple substance use among SMGs. These interventions likely need to include methods of targeting multiple substance use by targeting risk factors that cut-across several substances, particularly externalizing symptoms.
Acknowledgments
The production of this manuscript was supported by grants from the National Institute of Drug Abuse (R01 DA030385; R01 DA012237). We have no conflicts of interest to declare.
Footnotes
While lesbian and bisexual girls were examined together as SMGs, chi-square tests demonstrated that both subgroups were equally represented in each substance use class (p’s: .30–.90). Furthermore, t-tests and chi-square tests demonstrated that lesbian and bisexual girls did not differ in their levels of alcohol use (p=.28), cigarette use (p=.82), marijuana use (p=.78), and occurrence of binge drinking (p=.41).
Declaration of Interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Angold A, Costello EJ, Erkanli A. Comorbidity. Journal of Child Psychology and Psychiatry. 1999;40(1):57–87. [PubMed] [Google Scholar]
- Austin SB, Ziyadeh N, Fisher LB, Kahn JA, Colditz GA, Frazier AL. Sexual orientation and tobacco use in a cohort study of US adolescent girls and boys. Archives of Pediatrics & Adolescent Medicine. 2004;158(4):317. doi: 10.1001/archpedi.158.4.317. [DOI] [PubMed] [Google Scholar]
- Bandura A, McClelland DC. Social learning theory. Englewood Cliffs, NJ: Prentice-Hall; 1977. [Google Scholar]
- Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, Neer SM. The screen for child anxiety related emotional disorders (SCARED): Scale construction and psychometric characteristics. Journal of the American Academy of Child & Adolescent Psychiatry. 1997;36(4):545–553. doi: 10.1097/00004583-199704000-00018. [DOI] [PubMed] [Google Scholar]
- Bollen KA, Barb KH. Pearson’s r and coarsely categorized measures. American Sociological Review. 1981:232–239. [Google Scholar]
- Bostwick WB, Boyd CJ, Hughes TL, McCabe SE. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. American Journal of Public Health. 2010;100(3):468–475. doi: 10.2105/AJPH.2008.152942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpiano RM, Kelly BC, Easterbrook A, Parsons JT. Community and drug use among gay men the role of neighborhoods and networks. Journal of Health and Social Behavior. 2011;52(1):74–90. doi: 10.1177/0022146510395026. [DOI] [PubMed] [Google Scholar]
- Chung T, Kim KH, Hipwell AE, Stepp SD. White and black adolescent females differ in profiles and longitudinal patterns of alcohol, cigarette, and marijuana use. Psychology of Addictive behaviors. 2013 doi: 10.1037/a0031173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cochran BN, Stewart AJ, Ginzler JA, Cauce AM. Challenges faced by homeless sexual minorities: Comparison of gay, lesbian, bisexual, and transgender homeless adolescents with their heterosexual counterparts. American Journal of Public Health. 2002;92(5):773–777. doi: 10.2105/Ajph.92.5.773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colby SM, Tiffany ST, Shiffman S, Niaura RS. Are adolescent smokers dependent on nicotine? A review of the evidence. Drug and alcohol dependence. 2000;59(Supplement 1):83–95. doi: 10.1016/s0376-8716(99)00166-0. http://dx.doi.org/10.1016/S0376-8716(99)00166-0. [DOI] [PubMed] [Google Scholar]
- Conway KP, Vullo GC, Nichter B, Wang J, Compton WM, Iannotti RJ, Simons-Morton B. Prevalence and patterns of polysubstance use in a nationally representative sample of 10th graders in the united states. Journal of Adolescent Health. 2013;52(6):716–723. doi: 10.1016/j.jadohealth.2012.12.006. http://dx.doi.org/10.1016/j.jadohealth.2012.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper ML, Russell M, George WH. Coping, expectancies, and alcohol abuse: a test of social learning formulations. Journal of Abnormal Psychology. 1988;97(2):218. doi: 10.1037//0021-843x.97.2.218. [DOI] [PubMed] [Google Scholar]
- Corliss HL, Rosario M, Wypij D, Wylie SA, Frazier AL, Austin SB. Sexual orientation and drug use in a longitudinal cohort study of US adolescents. Addictive behaviors. 2010;35(5):517–521. doi: 10.1016/j.addbeh.2009.12.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corliss HL, Rosario M, Wypij D, Fisher LB, Austin SB. Sexual orientation disparities in longitudinal alcohol use patterns among adolescents: findings from the Growing Up Today Study. Archives of Pediatrics & Adolescent Medicine. 2008;162(11):1071–1078. doi: 10.1001/archpedi.162.11.1071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corliss HL, Wadler BM, Jun HJ, Rosario M, Wypij D, Frazier AL, Austin SB. Sexual-orientation disparities in cigarette smoking in a longitudinal cohort study of adolescents. Nicotine & Tobacco Research. 2013;15(1):213–222. doi: 10.1093/ntr/nts114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dermody SS, Marshal MP, Cheong J, Burton C, Hughes T, Aranda F, Friedman MS. Longitudinal disparities of hazardous drinking between sexual minority and heterosexual individuals from adolescence to young adulthood. Journal of Youth and Adolescence. 2014;43(1):30–39. doi: 10.1007/s10964-013-9905-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dierker LC, Vesel F, Sledjeski EM, Costello D, Perrine N. Testing the dual pathway hypothesis to substance use in adolescence and young adulthood. Drug and alcohol dependence. 2007;87(1):83–93. doi: 10.1016/j.drugalcdep.2006.08.001. [DOI] [PubMed] [Google Scholar]
- Dishion TJ, Ha T, Veronneau MH. An ecological analysis of the effects of deviant peer clustering on sexual promiscuity, problem behavior, and childbearing from early adolescence to adulthood: an enhancement of the life history framework. Dev Psychol. 2012;48(3):703–717. doi: 10.1037/a0027304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doty ND, Willoughby BL, Lindahl KM, Malik NM. Sexuality related social support among lesbian, gay, and bisexual youth. J Youth Adolesc. 2010;39(10):1134–1147. doi: 10.1007/s10964-010-9566-x. [DOI] [PubMed] [Google Scholar]
- Fergusson DM, Horwood LJ, Ridder EM. Conduct and attentional problems in childhood and adolescence and later substance use, abuse and dependence: results of a 25-year longitudinal study. Drug and alcohol dependence. 2007;88:S14–S26. doi: 10.1016/j.drugalcdep.2006.12.011. [DOI] [PubMed] [Google Scholar]
- Friedman MS, Marshal MP, Guadamuz TE, Wei CY, Wong CF, Saewyc EM, Stall R. A meta-analysis of disparities in childhood sexual abuse, parental physical abuse, and peer victimization among sexual minority and sexual nonminority individuals. American Journal of Public Health. 2011;101(8):1481–1494. doi: 10.2105/Ajph.2009.190009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gadow K, Sprafkin J. Adolescent symptom inventory-4 norms manual. Stony Brook, NY: Checkmate Plus; 1998. [Google Scholar]
- Gadow K, Sprafkin J, Weiss M. Adult Self-Report Inventory 4 manual. Stony Brook, NY: Checkmate Plus; 2004. [Google Scholar]
- Goldbach JT, Tanner-Smith EE, Bagwell M, Dunlap S. Minority stress and substance use in sexual minority adolescents: A meta-analysis. Prevention Science. 2014:1–14. doi: 10.1007/s11121-013-0393-7. [DOI] [PubMed] [Google Scholar]
- Goldbach JT, Schrager SM, Dunlap SL, Holloway IW. The application of minority stress theory to marijuana use among sexual minority adolescents. Substance Use and Misuse. 2015;50(3):366–365. doi: 10.3109/10826084.2014.980958. [DOI] [PubMed] [Google Scholar]
- Greenwood GL, White EW, Page-Shafer K, Bein E, Osmond DH, Paul J, Stall RD. Correlates of heavy substance use among young gay and bisexual men: The San Francisco Young Men’s Health Study. Drug and alcohol dependence. 2001;61(2):105–112. doi: 10.1016/s0376-8716(00)00129-0. http://dx.doi.org/10.1016/S0376-8716(00)00129-0. [DOI] [PubMed] [Google Scholar]
- Hipwell AE, Loeber R, Stouthamer-Loeber M, Keenan K, White HR, Kroneman L. Characteristics of girls with early onset disruptive and antisocial behaviour. Criminal Behaviour and Mental Health. 2002;12(1):99–118. doi: 10.1002/cbm.489. [DOI] [PubMed] [Google Scholar]
- Hipwell AE, Stepp SD, Keenan K, Allen A, Hoffmann A, Rottingen L, McAloon R. Examining links between sexual risk behaviors and dating violence involvement as a function of sexual orientation. Journal of pediatric and adolescent gynecology. 2013;26(4):212–218. doi: 10.1016/j.jpag.2013.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussong AM, Jones DJ, Stein GL, Baucom DH, Boeding S. An internalizing pathway to alcohol use and disorder. Psychology of Addictive behaviors. 2011;25(3):390. doi: 10.1037/A0024519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Institute of Medicine. The health of lesbian, gay, bisexual, and transgender people: Building a foundation for better understanding. Washington DC: The National Academic Press; 2011. [PubMed] [Google Scholar]
- Johnson DR, Creech JC. Ordinal measures in multiple indicator models: A simulation study of categorization error. American Sociological Review. 1983:398–407. [Google Scholar]
- Kelly AB, Evans-Whipp TJ, Smith R, Chan GC, Toumbourou JW, Patton GC, Catalano RF. A longitudinal study of the association of adolescent polydrug use, alcohol use and high school non-completion. Addiction. 2015;110(4):627–635. doi: 10.1111/add.12829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keenan K, Hipwell A, Chung T, Stepp S, Stouthamer-Loeber M, Loeber R, McTigue K. The Pittsburgh Girls Study: overview and initial findings. Journal of Clinical Child & Adolescent Psychology. 2010;39(4):506–521. doi: 10.1080/15374416.2010.486320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- King SM, Iacono WG, McGue M. Childhood externalizing and internalizing psychopathology in the prediction of early substance use. Addiction. 2004;99(12):1548–1559. doi: 10.1111/j.1360-0443.2004.00893.x. [DOI] [PubMed] [Google Scholar]
- Lampinen TM, McGhee D, Martin I. Increased risk of “club” drug use among gay and bisexual high school students in British Columbia. Journal of Adolescent Health. 2006;38(4):458–461. doi: 10.1016/j.jadohealth.2005.04.013. http://dx.doi.org/10.1016/j.jadohealth.2005.04.013. [DOI] [PubMed] [Google Scholar]
- Lanza ST, Rhoades BL. Latent class analysis: An alternative perspective on subgroup analysis in prevention and treatment. Prevention Science. 2013;14(2):157–168. doi: 10.1007/s11121-011-0201-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lea T, Reynolds R, de Wit J. Alcohol and other drug use, club drug dependence and treatment seeking among lesbian, gay and bisexual young people in Sydney. Drug and Alcohol Review. 2013;32(3):303–311. doi: 10.1111/dar.12004. [DOI] [PubMed] [Google Scholar]
- Marshal MP, Burton CM, Chisolm DJ, Sucato GS, Friedman MS. Cross-sectional evidence for a stress-negative affect pathway to substance use among sexual minority girls. Clinical and Translational Science. 2013;6(4):321–322. doi: 10.1111/Cts.12052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Dermody SS, Shultz M, Sucato G, Stepp SD, Chung T, Hipwell AE. Mental health and substance use disparities among urban adolescent lesbian and bisexual girls. Journal of the American Psychiatric Nurses Assocation. 2013;19(5):271–279. doi: 10.1177/1078390313503552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Dietz LJ, Friedman MS, Stall R, Smith HA, McGinley J, Brent DA. Suicidality and depression disparities between sexual minority and heterosexual youth: a meta-analytic review. Journal of Adolescent Health. 2011;49(2):115–123. doi: 10.1016/j.jadohealth.2011.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Friedman MS, Stall R, King KM, Miles J, Gold MA, Morse JQ. Sexual orientation and adolescent substance use: a meta-analysis and methodological review. Addiction. 2008;103(4):546–556. doi: 10.1111/j.1360-0443.2008.02149.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, King KM, Stepp SD, Hipwell A, Smith H, Chung T, Markovic N. Trajectories of alcohol and cigarette use among sexual minority and heterosexual girls. Journal of Adolescent Health. 2012;50(1):97–99. doi: 10.1016/j.jadohealth.2011.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Sucato G, Stepp SD, Hipwell A, Smith HA, Friedman MS, Markovic N. Substance use and mental health disparities among sexual minority girls: Results from the Pittsburgh girls study. Journal of pediatric and adolescent gynecology. 2012;25(1):15–18. doi: 10.1016/j.jpag.2011.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKee SA, Weinberger AH. How Can We Use Our Knowledge of Alcohol-Tobacco Interactions to Reduce Alcohol Use? Annual review of clinical psychology. 2013;9:649–674. doi: 10.1146/annurev-clinpsy-050212-185549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLachlan G, Peel D. Finite mixture models 2000. NY: John Wiley and Sons; 1974. [Google Scholar]
- Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological bulletin. 2003;129(5):674. doi: 10.1037/0033-2909.129.5.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moss HB, Chen CM, Yi HY. Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample. Drug and alcohol dependence. 2014;136:51–62. doi: 10.1016/j.drugalcdep.2013.12.011. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Statistical analysis with latent variables. Mplus Version 7 User’s Guide 1998–2012 [Google Scholar]
- Nagin D. Group-based modeling of development. Harvard University Press; 2005. [Google Scholar]
- Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Structural Equation Modeling. 2007;14(4):535–569. [Google Scholar]
- Operario D, Choi KH, Chu P, McFarland W, Secura G, Behel S, Valleroy L. Prevalence and Correlates of Substance Use Among Young Asian Pacific Islander Men Who Have Sex with Men. Prevention Science. 2006;7(1):19–29. doi: 10.1007/s11121-005-0018-x. [DOI] [PubMed] [Google Scholar]
- Pandina RJ, Labouvie EW, White HR. Potential contributions of the life span developmental approach to the study of adolescent alcohol and drug use: The Rutgers Health and Human Development Project, a working model. Journal of Drug Issues. 1984;14(2):253–268. [Google Scholar]
- Pardini D, White HR, Stouthamer-Loeber M. Early adolescent psychopathology as a predictor of alcohol use disorders by young adulthood. Drug and alcohol dependence. 2007;88:S38–S49. doi: 10.1016/j.drugalcdep.2006.12.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ramo DE, Liu H, Prochaska JJ. Tobacco and marijuana use among adolescents and young adults: A systematic review of their co-use. Clinical Psychology Review. 2012;32(2):105–121. doi: 10.1016/j.cpr.2011.12.002. http://dx.doi.org/10.1016/j.cpr.2011.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rhemtulla M, Brosseau-Liard PE, Savalei V. When can categorical variables be treated as continuous? A comparison of robust continuous and categorical SEM estimation methods under suboptimal conditions. Psychological Methods. 2012;17(3):354. doi: 10.1037/a0029315. [DOI] [PubMed] [Google Scholar]
- Robin L, Brener ND, Donahue SF, Hack T, Hale K, Goodenow C. Associations between health risk behaviors and opposite-, same-, and both-sex sexual partners in representative samples of Vermont and Massachusetts high school students. Archives of Pediatrics & Adolescent Medicine. 2002;156(4):349. doi: 10.1001/archpedi.156.4.349. [DOI] [PubMed] [Google Scholar]
- Rostosky SS, Owens GP, Zimmerman RS, Riggle ED. Associations among sexual attraction status, school belonging, and alcohol and marijuana use in rural high school students. Journal of Adolescence. 2003;26(6):741–751. doi: 10.1016/j.adolescence.2003.09.002. [DOI] [PubMed] [Google Scholar]
- Rudolph KD, Lansford JE, Agoston AM, Sugimura N, Schwartz D, Dodge KA, Bates JE. Peer victimization and social alienation: predicting deviant peer affiliation in middle school. Child development. 2014 doi: 10.1111/cdev.12112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saewyc EM, Homma Y, Skay CL, Bearinger LH, Resnick MD, Reis E. Protective factors in the lives of bisexual adolescents in North America. American Journal of Public Health. 2009;99(1):110–117. doi: 10.2105/AJPH.2007.123109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith A, Lindsay J, Rosenthaly DA. Same-sex attraction, drug injection and binge drinking among Australian adolescents. Australian and New Zealand Journal of Public Health. 1999;23(6):643–646. doi: 10.1111/j.1467-842X.1999.tb01552.x. [DOI] [PubMed] [Google Scholar]
- Thiede H, Valleroy LA, MacKellar DA, Celentano DD, Ford WL, Hagan H, Shehan DA. Regional patterns and correlates of substance use among young men who have sex with men in 7 US urban areas. American Journal of Public Health. 2003;93(11):1915–1921. doi: 10.2105/Ajph.93.11.1915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torra V, Domingo-Ferrer J, Mateo-Sanz JM, Ng M. Regression for ordinal variables without underlying continuous variables. Information Sciences. 2006;176(4):465–474. [Google Scholar]
- U.S. Department of Health and Human Services. Healthy People 2020. 2012 Retrieved March 12, 2014, 2014, from http://www.hhs.gov/ash/oah/resources-and-publications/healthy-people-2020.html.
- Van De Ven M, Greenwood P, Engels R, Olsson C, Patton G. Patterns of adolescent smoking and later nicotine dependence in young adults: a 10-year prospective study. Public health. 2010;124(2):65–70. doi: 10.1016/j.puhe.2009.11.009. [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Chen X, Hoyt DR, Tyler KA, Johnson KD. Mental disorder, subsistence strategies, and victimization among gay, lesbian, and bisexual homeless and runaway adolescents. Journal of Sex Research. 2004;41(4):329–342. doi: 10.1080/00224490409552240. [DOI] [PubMed] [Google Scholar]
- Williams T, Connolly J, Pepler D, Craig W. Peer victimization, social support, and psychosocial adjustment of sexual minority adolescents. Journal of Youth and Adolescence. 2005;34(5):471–482. doi: 10.1007/s10964-005-7264-x. [DOI] [Google Scholar]
- Zumbo BD, Zimmerman DW. Is the selection of statistical methods governed by level of measurement? Canadian Psychology/Psychologie canadienne. 1993;34(4):390. [Google Scholar]