

Abstract
Background
To compare sports-related hip injuries based on sex and age in a cohort of young athletes.
Methods
5% random probability sample of all new patients’ charts over a ten-year time period was selected for investigation. The most common hip injury diagnoses, sport at time of injury, mechanism (acute/traumatic versus overuse), and types (bony versus soft tissue) were compared by sex and age (pre-adolescent versus adolescent). Descriptive and chi-square analyzes were performed. The interaction of sex and age with regard to hip injury over time was examined by a two-way (sex, age) analysis of variance (ANOVA).
Results
2,133 charts were reviewed; N=87 hip injuries. Leading diagnoses for males included labral tear (23.1%), avulsion fracture (11.5%), slipped capital femoral epiphysis (11.5%), dislocation (7.7%) and tendonitis (7.7%). Leading diagnoses for females were labral tear (59.0%), tendonitis (14.8%), snapping hip syndrome (6.6%), strain (4.9%) and bursitis (4.9%). Five most common sports/activities at time of hip injury were dancing/ballet (23.0%), soccer (18.4%), gymnastics (9.2%), ice hockey (8.1%), and track and fields (6.9%). Growth/maturation by sex showed a greater proportion of the total hip injuries (38.5%) compared to females (8.2%) during pre-adolescence (5-12 years). However, in adolescence (13-17 years), hip injury proportion was significantly greater in females (91.8%), as compared to males (61.5%; P<0.001). Injury mechanism and type differed by sex with females sustaining more chronic/overuse (95.1%) and soft tissue type injuries (93.4%), as compared to males (50.0% and 53.8%, respectively; P<0.001). Females were found to have a sharper increase in hip injury proportion as they progress through puberty as compared to males (ANOVA sex-by-age interaction; P<0.001).
Conclusions
Hip injury mechanism and type differed significantly between males and females during growth. Notably, the proportion of hip injuries in the young female athletes showed a significantly greater increase with advancing age as compared to males. Hip injuries in children and the interplay with growth, as it relates to injury predisposition, requires further investigation in order to facilitate efforts aimed at prevention.
Keywords: Children, Athletic Injury, Maturation, Sex Differences, Puberty
INTRODUCTION
The anatomic and biomechanical considerations for hip injuries in athletes are among the most complex in the musculoskeletal system, making clinical decisions surrounding the diagnosis and treatment of these injuries very challenging. Hip disorders in young athletes are increasingly recognized as a cause of dysfunction and disability.1 Skeletally immature and actively growing athletes present the clinician with an added layer of diagnostic difficulty surrounding hip injuries. These athletes may be at increased risk of injury due to imbalances among neuromuscular control, strength, and flexibility. Micheli originally discussed this phenomenon, stating that children may be more susceptible to overuse injury than adults due to ongoing bone development, the presence of growth cartilage and the physical maturation process itself.2-4 Notably, between the ages of 6 and 14 years, the increase in limb mass is double the increase in limb length, which may contribute to an imbalance of forces resulting in decreased lower extremity control and function.5-8 Young, actively growing female athletes, have additional biomechanical risk factors that set them apart from males with regard to injury risk stratification. Several investigations have demonstrated that post-pubertal female athletes exhibit different mechanics compared to males during landing and pivoting movements that likely increase injury risk.9-18 A working knowledge of the injury spectrum of hip pathology afflicting young athletes, along with an understanding of the biomechanical changes of the morphing body during puberty, is required to accurately appreciate the injury profile and pathophysiology inherent to hip injuries in youth sports.
Along with the developmental changes that occur during childhood, a potentially unsafe new trend in the culture of youth sports is emerging which adds to injury risk. Young children are playing sports with increased intensity and specialization, starting as early as age 6 to 8 years. In the United States, participation in organized sports has increased from approximately 9% of children 6 years and younger in 1997, to 12% in 2008.19 No evidence currently exists in support of the notion that intense sports participation, specialization, and practice before puberty are necessary to achieve elite status.20 Increased sports involvement of children from an early age, particularly through the years of growth and development, raises a concern about the risk and severity of injury during this formative period of time. A new report has shown that early sport specialization of female adolescents is associated with increased risk of anterior knee pain disorders, when compared to multi-sport athletes.21 Additionally, early sport specialization was found to be an independent factor for increased athletic injury risk in young athletes.22 However, reliable epidemiological data focusing on hip injuries in children is very sparse in the literature at this time.
Athletically related hip and groin injuries are not as common as other lower extremity injuries, especially the knee and ankle joints.23 Epidemiological studies of high school athletes have shown that hip injuries comprised approximately 5% to 9% of the total athletically related injuries.24,25 Another recent study, which included 268 female middle school athletes, showed that hip injures made up only 1% of the total injuries in this particular cohort.26 Athletic injuries associated with the hip, especially in the pediatric population, have not been studied in detail. Therefore, the primary purpose of this study is to investigate the effect of gender and growth in a cohort of young athletes with hip injuries abstracted from a larger data-base of athletes with all types of injuries presenting to a pediatric based sports medicine clinic over a ten year time period.
MATERIALS AND METHODS
Participants
All 5 -17 year old patients who visited the Division of Sports Medicine between 2000 and 2010 (10 years; 1/1/00 -12/31/09) were initially identified. There were a total of 121,047 patient visits from which a 5% probability sample was randomly selected. To obtain the 5% of probably random sample, “sample” command in Stata (StataCorp, College Station, Texas) was used. Due to time and money constraints, roughly two-thirds of the 5% sample of charts were reviewed and coded. Six research assistants performed a medical chart review from the identified subjects. The inter-coder reliability was examined using Krippendorff α to ensure quality of search and coding process, and the observed α value was 0.721, which was above the level of acceptability.27
Data Inclusion, Exclusion, and Extraction Process
For a patient's injury to be included, the injury had to be coded as “hip” for body part/location and sustained during sports participation. The medical chart had to contain all variables under study purposes: sex, age, diagnosis, sports, injury mechanism (acute/traumatic versus overuse), and injury type (bony versus soft tissue). In cases when the final diagnosis was questionable, medical records were further reviewed, and the final diagnosis was confirmed by a primary care sports medicine physician. Exclusion criteria included all injuries sustained as a result of accidents that occurred during activities of daily living (e.g., falling down the stairs or falling off a bike while riding recreationally), injuries for which the activity at the time of injury was not specified, and cases where the patient had an underlying congenital disorder (e.g., Osteogenesis Imperfecta or Sickle Cell Disease). Injuries in this study cohort that were coded as “pelvis” were excluded from this analysis. Based on the inclusion and exclusion described above, those eligible medical charts were extracted for the data analysis.
Data Reduction
Anthropometric measures such as age, height, and weight were also extracted from the reviewed medical records, and body mass index (BMI) was calculated from the height and weight recording in the medical record as weight in kg/height in m2. BMI categories were created using cutoffs for children and teens provided by the Centers for Disease Control and Prevention.28 To investigate growth by sex comparison of hip injuries, age was used to characterize the patient as either 5-12 years or 13 -17 years. Age categories were selected based upon national data on pubertal status in children and adolescents.29,30 Additionally, to examine mechanism and type of hip injury based on sex, mechanisms were categorized as acute/traumatic versus overuse, and type of hip injury was stratified by bony versus soft tissue.
Statistical Analysis
The frequency of common hip injuries and sport participated in at the time of injury were analyzed by descriptive statistics. The top five diagnoses of hip injuries were reported for males and females separately. To investigate the frequency of hip injuries based on defined categorical variables including age group, mechanism of injury (acute/traumatic versus overuse), and type of injury (bony versus soft tissue), chi-square (χ2) was used. Hip injuries for children ages 5 -17 years were compared between females and males using a generalized linear model (GLM) with a binomial distribution and logit link function. This model was selected because the study cohort of hip injuries was abstracted from a larger data set of all types of injuries sampled over a ten year time period from sports medicine clinic. Therefore, data for this calculation represent counts of hip injuries to total sports injuries × 100%.31 A two-way analysis of variance (ANOVA) was used to compare the proportion of hip injuries to total injuries between males and females across the range of ages (sex, age), and the interaction of sex and age with regard to hip injury over time was examined. Goodness-of-fit of the two-way ANOVA model was judged by the Akaike information criterion and the slope comparison was assessed by the sex-by-age interaction term using the Wald chi-square test on one degree of freedom.32 Age was treated as a covariate in the model and 95% confidence intervals were calculated for the proportion of hip injuries to total injuries based on age for each sex. Statistical analysis was performed using IBM SPSS Statistics (version 21.0, IBM, Armonk, NY). Statistical significance was established using a priori criteria of two-tailed P<0.05.
RESULTS
From the 121,047 total patient visits over the study time period, a total of 2,133 charts were reviewed from which 87 hip injuries were aggregated and analyzed (Figure 1). Mean and standard deviation by sex were calculated for anthropometric information including age, height, weight, and BMI (Table 1). The leading hip injury diagnosis for both the females and males in this study cohort of young athletes was acetabular labral tear. Fifty-nine percent of the injuries in female athletes were labral tears as compared to 23% in male athletes. Other leading diagnoses for the females included tendonitis (15%), snapping hip syndrome (6%), muscle strain (5%), and bursitis (5%) (Figure 2). The other leading diagnoses for the males were bony in nature including avulsion fracture (11%), slipped capital femoral epiphysis (11%), hip dislocation (8%) and tendonitis (8%) (Figure 3). The top five hip injuries in both females and males are labral tear (48%), tendonitis (12%), snapping hip syndrome (6%), strain (6%), and bursitis (5%) (Figure 4). The five most common sports participated in at the time of hip injury for males and females were dance/ballet (23.0%), soccer (18.4%), gymnastics (9.2%), ice hockey (8.1%), and track and field (6.9%).
Figure 1.
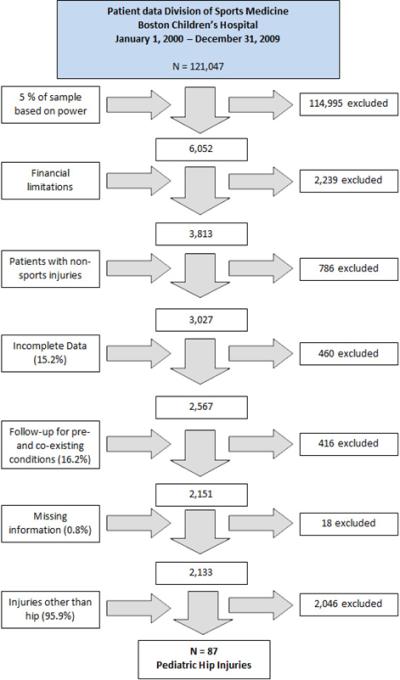
Flow chart of data processing
Table 1.
Age, height, weight, and BMI of patients with hip injuries (N=87) by sex
| Female (N = 61) | Male (N = 26) | |
|---|---|---|
| Age (years) | 15.3 ± 1.8 | 13.4 ± 3.2 |
| Height (cm) | 162.5 ± 7.8 | 166.8 ± 16.7 |
| Weight (kg) | 56.0 ± 8.4 | 63.8 ± 20.6 |
| BMI | 21.1 ± 3.1 | 23.8 ± 4.1 |
Figure 2.
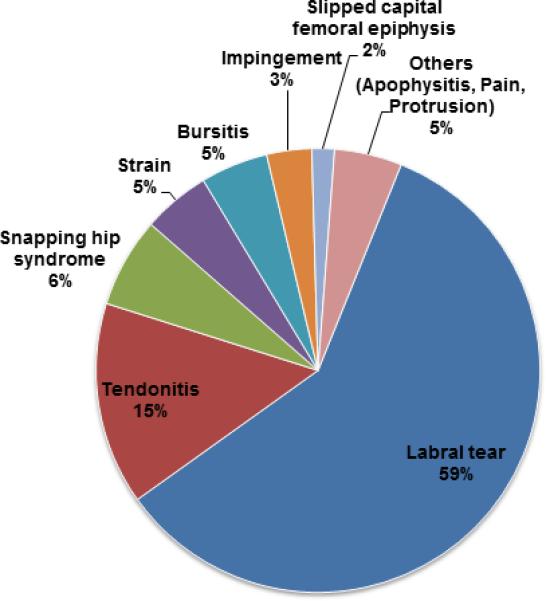
Distribution of female hip injuries
Figure 3.
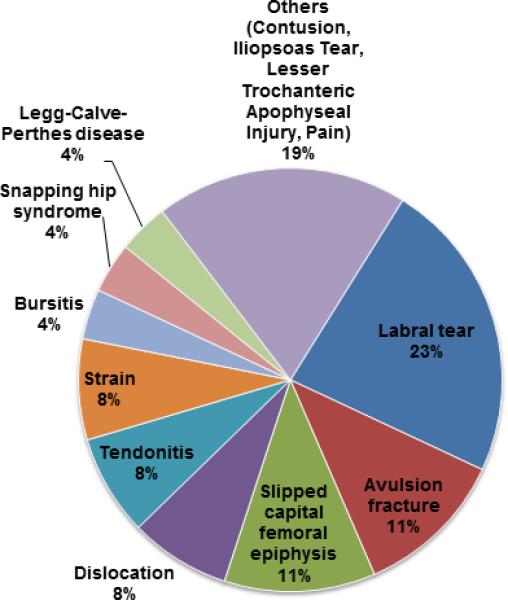
Distribution of male hip injuries
Figure 4.
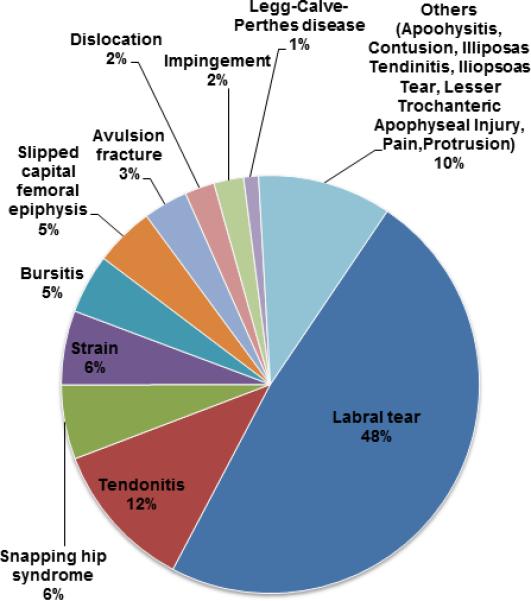
Distribution of male and female hip injuries
Growth by sex comparison revealed that males showed a greater proportion of the total hip injuries during the younger 5-12 year range. However, during adolescence females sustained a significantly greater proportion of the hip injuries (Table 2). Injury mechanism and type differed by sex with females sustaining more overuse and soft tissue type injuries, as compared to males (Table 2).
Table 2.
Comparison of hip injury age category and type (acute/traumatic versus overuse; bony versus soft tissue) by sex
| Female | Male | |
|---|---|---|
| Age category (%) | ||
| 5-12 years old | 5 (8.2%) | 10 (38.5%) |
| 13-17 years old | 56 (91.8%) | 16 (61.5%) |
| Chi2(df), p-value | 11.702(1), <.001 | |
| Injury type (%) | ||
| Acute/Traumatic | 3 (4.9%) | 13 (50.0%) |
| Overuse | 58 (95.1%) | 13 (50.0%) |
| Chi2(df), p-value | 24.686(1), <.001 | |
| Bony/soft tissue (%) | ||
| Bony | 4 (6.6%) | 10 (38.5%) |
| Soft tissue | 57 (93.4%) | 14 (53.8%) |
| Other | 0 (0.0%) | 2 (7.7%) |
| Chi2(df), p-value | 19.726(2), <.001 | |
| Total N | 61 | 26 |
The GLM model indicated an interaction between sex and age. Although the proportion of hip injuries (hip injury / total injury ratio) in males ranged from 2-4% over the years, hip injuries in females showed a steady increase as they become older. (Wald chi-square = 10.94 on one degree of freedom, P<0.001). The change in the slope of hip injury / total injury ratio as age advances through puberty into adolescence shows that females have a steeper increase over this time period when compared to the males with hip injuries (Figure 5).
Figure 5.
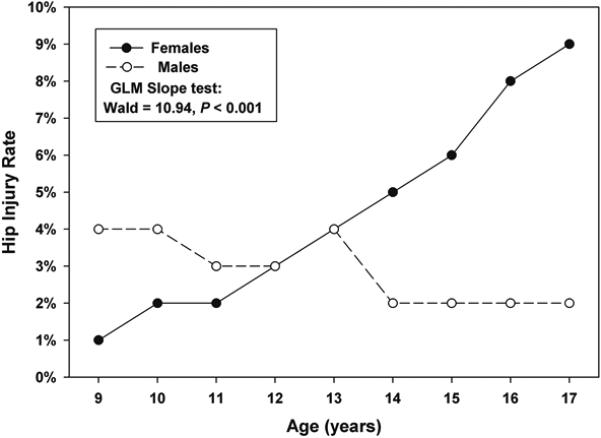
Hip injury rate by age and sex
The correlation coefficient analysis between BMI and number of hip injuries showed a weak correlation (r=0.43 and r2=0.19)33 and no statistical significance (P=0.33).
DISCUSSION
The current literature is sparse in regards to reliable epidemiologic studies on hip injuries in skeletally immature athletes. The current study of a cohort of young athletes aged 5-17 years with sports related hip injuries, supports the notion that injury patterns are sex specific throughout growth and maturation.
Hip injuries sustained by the males in this study cohort tended to be more bony and acute in nature when compared to the females (Figure 2, 3). Avulsion fractures and slipped capital femoral epiphysis were the second and third leading diagnoses for the males respectively (Figure 3). These bone related diagnoses for females, in comparison, did not make the list of leading hip injuries (Figure 2). Avulsion fractures are a common injury type in skeletally immature athletes and are most common in the pelvis and lower extremities.34 The classic injury pattern in adolescents results from a sudden forceful contraction of the musculotendinous unit during sport when kicking, running, or changing direction. Consistently, approximately one third of all hip injuries in this cohort were from participation in soccer, ice hockey, or track and field, sports that require rapid starts and stops. Within these three sports, the majority of hip injuries sustained were by the males. This injury profile in young males is likely reflective of the strength and flexibility imbalances that develop during the pubertal growth spurt.
In comparison to the males, the females sustained hip injuries from activities that fall within the performing arts category, such as dance/ballet and gymnastics. Approximately one third of the total hip injuries in this cohort were a result of participation in these two activities. The interplay between activities that use extreme ranges of motion of the hip and require exceptional flexibility, with regards to the injury profile in females, has yet to be investigated in great detail. The results of this study found that roughly 1/5 of the young females sustained injuries classified as tendonitis or snapping hip. The anterior and or lateral snapping hip of the dancer is an extremely common overuse injury in this population. This clinical sign of iliopsoas snapping is often painless, and viewed as harmless in nature, by most athletes. However, this ‘audible alert’ too often precedes a significant overuse injury, resulting in marked time loss from sports participation and competition.35,36
Acetabular labral tears were more common in females, as compared to males. This sex difference in hip injury patterns may not be entirely unexpected. Males and females have different hip anatomy, strength, movement and muscle activation patterns. Studies in healthy subjects have demonstrated sex-specific differences in normal acetabular and femoral structure.37-39 These structural sex-specific differences may contribute to hip impingement and subsequent labral pathology. In athletes with femoroacetabular impingement (FAI), cam impingement is more common in young males, whereas pincer impingement is more common in middle-aged females.40 Within the same category of FAI, Clohisy and colleagues reported that male hips with pincer FAI have decreased head-neck offset, and an aspherical femoral head, while female hips have increased acetabular inclination, and a cross-over sign.41 Sports such as dance, cheerleading, figure skating, and gymnastics are often female dominated, and consist of athletes who may have a mild amount of dysplasia and/or soft-tissue laxity, and subject their hips to supra-physiological motions because of the demands of their sports.42 Dynamic pincer impingement can occur in cases whereby the osseous morphology of both the femoral head and acetabulum are normal but the demands of motion are extreme, causing acetabular rim overload and labral injury.43,44
One of major findings of our analysis is that the proportion of hip injuries in the young female athletes showed a significantly greater increase with advancing age as compared to the males in this cohort. (Figure 5) The increased number of athletically related injuries in the female population during pubescence has been reported in the knee.45 During maturation, the females experience a series of anatomical and hormonal changes, and as a result, body composition changes. Two studies that focused on identifying risk factors for traumatic knee injury identified that BMI was a risk factor.46,47 Another study reported that increased body fat from pre-pubescence to pubescence in female athletes is associated with increased risk of future traumatic knee injury.48 However, there was no correlation between BMI and hip injury that we found in this study. This may be related to the high number of dancers who are habituated to maintain a low BMI to meet the demands of the discipline.
Differences in movement patterns between males and females may contribute to the different injury rate in adolescence. In general, females demonstrate greater peak hip adduction and internal rotation than males.18,49-51 These sex characteristics could stem from differences in muscle strength or muscle activation patterns. Females tend to have weaker hip abductors and external rotators52 indicating that they may be less able to control adduction and internal rotation. Females also demonstrate different hip muscle activation patterns compared to males.53-55 Biomechanically, this injury pattern may be related to widening and increased anterior tilt of the pelvis, weak abdominal musculature, and lengthening of the spine and lower extremities during growth and maturation. Although the current evidence for these differences is primarily in post-adolescent athletes, similar movement pattern differences may exist in adolescence.
Limitations
Several limitations are inherent in the study design. The current data was obtained from a division of a large, pediatric tertiary hospital. Thus, the results may not be generalizable for other clinical settings. A fairly large proportion of charts were discarded due to incomplete data (15.2%) and pre-and co-existing conditions (16.2%; Figure 1), limiting the extent of data analysis that was initially intended. The incidence of hip injuries cannot be determined due to the lack of athletic exposure data.
CONCLUSIONS
This project was designed to analyze a random sampling of pediatric hip injuries seen in a tertiary level pediatric medical center over a 10 year time period. The young males tended to sustain hip injuries that were bony in nature, in contrast to females whose injuries tended to be more soft tissue. The young female athletes with hip injuries in this study were found to have a propensity toward overuse hip injuries, as compared to the young males whose injuries tended to be more acute/traumatic. Additionally, the proportion of hip injuries in the young female athletes showed a significantly greater increase with advancing age as compared to males. Future research is needed to characterize the osseous anatomy, and investigate physical characteristics and biomechanical profiles in young athletes with hip pathology. Hip injuries in children, and the interplay with growth and activity choice, require further understanding in order to move prevention efforts forward.
Acknowledgments
Funding Source: Robert Wood Johnson Foundation, specifically the Health Policies Scholars Human Capital Program; NIH K23 AR063235
Abbreviations
- BMI
Body mass index
- GLM
Generalized linear model
- ANOVA
Analysis of variance
- FAI
Femoroacetabular impingement
Footnotes
Financial Disclosure: All authors have no financial relationships relevant to this study to report.
REFERENCES
- 1.Byrd JW. Femoroacetabular impingement in athletes: current concepts. Am J Sports Med. 2014;42(3):737–751. doi: 10.1177/0363546513499136. [DOI] [PubMed] [Google Scholar]
- 2.Micheli LJ. Overuse injuries in children's sports: the growth factor. The Orthopedic clinics of North America. 1983;14(2):337–360. [PubMed] [Google Scholar]
- 3.Micheli LJ, Fehlandt AF., Jr. Overuse injuries to tendons and apophyses in children and adolescents. Clin Sports Med. 1992;11(4):713–726. [PubMed] [Google Scholar]
- 4.Micheli LJ. Preventing injuries in team sports : what the team physician needs to know In: FIMS Team Physician Manual. CD Concepts; Hong Kong: 2006. [Google Scholar]
- 5.Ford KR, Shapiro R, Myer GD, et al. Longitudinal sex differences during landing in knee abduction in young athletes. Med Sci Sports Exerc. 2010 Oct;42(10):1923–1931. doi: 10.1249/MSS.0b013e3181dc99b1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hewett TE, Myer GD, Ford KR, et al. Preparticipation physical examination using a box drop vertical jump test in young athletes: the effects of puberty and sex. Clin J Sport Med. 2006 Jul;16(4):298–304. doi: 10.1097/00042752-200607000-00003. [DOI] [PubMed] [Google Scholar]
- 7.Quatman CE, Ford KR, Myer GD, et al. Maturation leads to gender differences in landing force and vertical jump performance: a longitudinal study. Am J Sports Med. 2006 May;34(5):806–813. doi: 10.1177/0363546505281916. [DOI] [PubMed] [Google Scholar]
- 8.Ford KR, Myer GD, Hewett TE. Longitudinal effects of maturation on lower extremity joint stiffness in adolescent athletes. Am J Sports Med. 2010 Sep;38(9):1829–1837. doi: 10.1177/0363546510367425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ford KR, Myer GD, Smith RL, et al. A comparison of dynamic coronal plane excursion between matched male and female athletes when performing single leg landings. Clin Biomech (Bristol, Avon) 2006 Jan;21(1):33–40. doi: 10.1016/j.clinbiomech.2005.08.010. [DOI] [PubMed] [Google Scholar]
- 10.Malinzak RA, Colby SM, Kirkendall DT, et al. A comparison of knee joint motion patterns between men and women in selected athletic tasks. Clin Biomech. 2001 Jun;16(5):438–445. doi: 10.1016/s0268-0033(01)00019-5. [DOI] [PubMed] [Google Scholar]
- 11.Hewett TE, Myer GD, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Joint Surg Am. 2004;86-A(8):1601–1608. doi: 10.2106/00004623-200408000-00001. [DOI] [PubMed] [Google Scholar]
- 12.Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003 Oct;35(10):1745–1750. doi: 10.1249/01.MSS.0000089346.85744.D9. [DOI] [PubMed] [Google Scholar]
- 13.Chappell JD, Yu B, Kirkendall DT, Garrett WE. A comparison of knee kinetics between male and female recreational athletes in stop-jump tasks. Am J Sports Med. 2002 Mar-Apr;30(2):261–267. doi: 10.1177/03635465020300021901. [DOI] [PubMed] [Google Scholar]
- 14.McLean SG, Huang X, Su A, van den Bogert AJ. Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clin Biomech. 2004;19:828–838. doi: 10.1016/j.clinbiomech.2004.06.006. [DOI] [PubMed] [Google Scholar]
- 15.Kernozek TW, Torry MR, H. VH, et al. Gender differences in frontal and sagittal plane biomechanics during drop landings. Med Sci Sports Exerc. 2005 Jun;37(6):1003–1012. discussion 1013. [PubMed] [Google Scholar]
- 16.Zeller BL, McCrory JL, Kibler WB, et al. Differences in Kinematics and Electromyographic Activity Between Men and Women during the Single-Legged Squat. Am J Sport Med. 2003;31(3):449–456. doi: 10.1177/03635465030310032101. [DOI] [PubMed] [Google Scholar]
- 17.Pappas E, Hagins M, Sheikhzadeh A, et al. Biomechanical differences between unilateral and bilateral landings from a jump: gender differences. Clin J Sport Med. 2007 Jul;17(4):263–268. doi: 10.1097/JSM.0b013e31811f415b. [DOI] [PubMed] [Google Scholar]
- 18.Hewett TE, Ford KR, Myer GD, et al. Gender differences in hip adduction motion and torque during a single-leg agility maneuver. J Orthop Res. 2006 Mar;24(3):416–421. doi: 10.1002/jor.20056. [DOI] [PubMed] [Google Scholar]
- 19.Malina RM. Early sport specialization: roots, effectiveness, risks. Curr Sports Med Rep. 2010 Nov-Dec;9(6):364–371. doi: 10.1249/JSR.0b013e3181fe3166. [DOI] [PubMed] [Google Scholar]
- 20.Jayanthi N, Pinkham C, Dugas L, et al. Sports specialization in young athletes: evidence-based recommendations. Sports health. 2013 May;5(3):251–257. doi: 10.1177/1941738112464626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hall R, Barber Foss K, Hewett TE, et al. Sports Specialization is Associated With an Increased Risk of Developing Anterior Knee Pain in Adolescent Female Athletes. Journal of sport rehabilitation. 2014 Mar 12; doi: 10.1123/jsr.2013-0101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jayanthi NA, LaBella CR, Fischer D, et al. Sports-Specialized Intensive Training and the Risk of Injury in Young Athletes: A Clinical Case-Control Study. Am J Sports Med. 2015 Feb 2; doi: 10.1177/0363546514567298. [DOI] [PubMed] [Google Scholar]
- 23.Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001 Jul-Aug;29(4):521–533. doi: 10.1177/03635465010290042501. [DOI] [PubMed] [Google Scholar]
- 24.DeLee JC, Farney WC. Incidence of injury in Texas high school football. Am J Sports Med. 1992 Sep-Oct;20(5):575–580. doi: 10.1177/036354659202000515. [DOI] [PubMed] [Google Scholar]
- 25.Gomez E, DeLee JC, Farney WC. Incidence of injury in Texas girls' high school basketball. Am J Sports Med. 1996 Sep-Oct;24(5):684–687. doi: 10.1177/036354659602400521. [DOI] [PubMed] [Google Scholar]
- 26.Barber Foss KD, Myer GD, Hewett TE. Epidemiology of basketball, soccer, and volleyball injuries in middle-school female athletes. Phys Sportsmed. 2014 May;42(2):146–153. doi: 10.3810/psm.2014.05.2066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Content Analysis: An introduction to its methodology. 2nd ed. Sage; Beverly Hills, CA: 2004. Krippendorff. [Google Scholar]
- 28.Division of Nutrition PA, and Obesity, National Center for Chronic Disease Prevention and Health Promotion at the Centers for Disease Control and Prevention [January 2015]; Available at http://www.cdc.gov/healthyweight/assessing/bmi/childrens_BMI/about_childrens_BMI.html.
- 29.Rogol AD, Clark PA, Roemmich JN. Growth and pubertal development in children and adolescents: effects of diet and physical activity. The American journal of clinical nutrition. 2000 Aug;72(2 Suppl):521S–528S. doi: 10.1093/ajcn/72.2.521S. [DOI] [PubMed] [Google Scholar]
- 30.Euling SY, Herman-Giddens ME, Lee PA, et al. Examination of US puberty-timing data from 1940 to 1994 for secular trends: panel findings. Pediatrics. 2008 Feb;121(Suppl 3):S172–191. doi: 10.1542/peds.2007-1813D. [DOI] [PubMed] [Google Scholar]
- 31.Nelder JA WR. Generalized linear models. J Roy Statist Soc A. 1972;135(3):370–384. [Google Scholar]
- 32.Hauck WH DA. Wald's test as applied to hypotheses in logit analysis. J Am Statist Assoc. 1977;72:851–853. [Google Scholar]
- 33.Taylor R. Interpretation of the Correlation Coefficient: A Clinical Review. JDMS. 1990;1:35–39. [Google Scholar]
- 34.Rossi F, Dragoni S. Acute avulsion fractures of the pelvis in adolescent competitive athletes: prevalence, location and sports distribution of 203 cases collected. Skeletal radiology. 2001 Mar;30(3):127–131. doi: 10.1007/s002560000319. [DOI] [PubMed] [Google Scholar]
- 35.Teitz C. Hip and knee injuries in dancers. Journal of Dance Medicine and Science. 2000;4:23–29. [Google Scholar]
- 36.Micheli LJ, Curtis C. Stress fractures in the spine and sacrum. Clin Sports Med. 2006 Jan;25(1):75–88, ix. doi: 10.1016/j.csm.2005.08.001. [DOI] [PubMed] [Google Scholar]
- 37.Kohnlein W, Ganz R, Impellizzeri FM, et al. Acetabular morphology: implications for joint-preserving surgery. Clin Orthop Relat Res. 2009 Mar;467(3):682–691. doi: 10.1007/s11999-008-0682-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Nakahara I, Takao M, Sakai T, et al. Gender differences in 3D morphology and bony impingement of human hips. J Orthop Res. 2011 Mar;29(3):333–339. doi: 10.1002/jor.21265. [DOI] [PubMed] [Google Scholar]
- 39.Sayers A, Marcus M, Rubin C, et al. Investigation of sex differences in hip structure in peripubertal children. The Journal of clinical endocrinology and metabolism. 2010 Aug;95(8):3876–3883. doi: 10.1210/jc.2009-2446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lavigne M, Parvizi J, Beck M, et al. Anterior femoroacetabular impingement: part I. Techniques of joint preserving surgery. Clin Orthop Relat Res. 2004 Jan;(418):61–66. [PubMed] [Google Scholar]
- 41.Clohisy JC, Dobson MA, Robison JF, et al. Radiographic structural abnormalities associated with premature, natural hip-joint failure. J Bone Joint Surg Am. 2011 May;93(Suppl 2):3–9. doi: 10.2106/JBJS.J.01734. [DOI] [PubMed] [Google Scholar]
- 42.Hamilton D, Aronsen P, Loken JH, et al. Dance training intensity at 11-14 years is associated with femoral torsion in classical ballet dancers. Br J Sports Med. 2006 Apr;40(4):299–303. doi: 10.1136/bjsm.2005.020941. discussion 303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Charbonnier C, Kolo FC, Duthon VB, et al. Assessment of congruence and impingement of the hip joint in professional ballet dancers: a motion capture study. Am J Sports Med. 2011 Mar;39(3):557–566. doi: 10.1177/0363546510386002. [DOI] [PubMed] [Google Scholar]
- 44.Kolo FC, Charbonnier C, Pfirrmann CW, et al. Extreme hip motion in professional ballet dancers: dynamic and morphological evaluation based on magnetic resonance imaging. Skeletal radiology. 2013 May;42(5):689–698. doi: 10.1007/s00256-012-1544-9. [DOI] [PubMed] [Google Scholar]
- 45.LaBella CR, Hennrikus W, Hewett TE. Anterior cruciate ligament injuries: diagnosis, treatment, and prevention. Pediatrics. 2014 May;133(5):e1437–1450. doi: 10.1542/peds.2014-0623. [DOI] [PubMed] [Google Scholar]
- 46.Nilstad A, Andersen TE, Bahr R, et al. Risk factors for lower extremity injuries in elite female soccer players. Am J Sports Med. 2014 Apr;42(4):940–948. doi: 10.1177/0363546513518741. [DOI] [PubMed] [Google Scholar]
- 47.Evans KN, Kilcoyne KG, Dickens JF, et al. Predisposing risk factors for non-contact ACL injuries in military subjects. Knee Surg Sports Traumatol Arthrosc. 2012 Aug;20(8):1554–1559. doi: 10.1007/s00167-011-1755-y. [DOI] [PubMed] [Google Scholar]
- 48.Myer GD, Faigenbaum AD, Foss KB, et al. Injury initiates unfavourable weight gain and obesity markers in youth. Br J Sports Med. 2013 May 14; doi: 10.1136/bjsports-2012-091988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Chumanov ES, Wall-Scheffler C, Heiderscheit BC. Gender differences in walking and running on level and inclined surfaces. Clin Biomech (Bristol, Avon) 2008 Dec;23(10):1260–1268. doi: 10.1016/j.clinbiomech.2008.07.011. [DOI] [PubMed] [Google Scholar]
- 50.Ferber R, Osternig LR, Woollacott MH, et al. Gait perturbation response in chronic anterior cruciate ligament deficiency and repair. Clin Biomech (Bristol, Avon) 2003 Feb;18(2):132–141. doi: 10.1016/s0268-0033(02)00182-1. [DOI] [PubMed] [Google Scholar]
- 51.Ferber R, Davis IM, Williams DS., 3rd. Gender differences in lower extremity mechanics during running. Clin Biomech (Bristol, Avon) 2003 May;18(4):350–357. doi: 10.1016/s0268-0033(03)00025-1. [DOI] [PubMed] [Google Scholar]
- 52.Cowan SM, Crossley KM. Does gender influence neuromotor control of the knee and hip? J Electromyogr Kinesiol. 2009 Apr;19(2):276–282. doi: 10.1016/j.jelekin.2007.07.009. [DOI] [PubMed] [Google Scholar]
- 53.Landry SC, McKean KA, Hubley-Kozey CL, et al. Gender differences exist in neuromuscular control patterns during the pre-contact and early stance phase of an unanticipated side-cut and cross-cut maneuver in 15-18 years old adolescent soccer players. J Electromyogr Kinesiol. 2009 Oct;19(5):e370–379. doi: 10.1016/j.jelekin.2008.08.004. [DOI] [PubMed] [Google Scholar]
- 54.Lewis CL, Sahrmann SA. Muscle activation and movement patterns during prone hip extension exercise in women. J Athl Train. 2009 May-Jun;44(3):238–248. doi: 10.4085/1062-6050-44.3.238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Zazulak BT, Ponce PL, Straub SJ, et al. Gender comparison of hip muscle activity during single-leg landing. J Orthop Sports Phys Ther. 2005 May;35(5):292–299. doi: 10.2519/jospt.2005.35.5.292. [DOI] [PubMed] [Google Scholar]