

Abstract
A 38-year-old male who sustained blunt abdominal trauma at work presented to the emergency department with complaints of abdominal pain localized primarily in the peri-umbilical region. The patient was discharged home after a brief uneventful hospitalization only to return 13 days later with signs and symptoms of acute bowel obstruction. Following clinical and radiological workup, a computed tomography (CT) scan was obtained which revealed markedly dilated and thickened bowel, induration and vascular congestion seen along the adjacent mesentery with fat stranding. The patient was taken emergently to the operating room (OR) where a small mesenteric defect was found, secondary to trauma, facilitating an internal hernia precipitating a small bowel obstruction. We urge the surgeon to maintain a low index of suspicion for acute bowel obstruction in the blunt trauma population. A CT scan is essential in evaluating this patient population and we cannot underscore enough the importance and value of this modality in radiologic imaging. We further recommend resection of the compromised bowel and associated mesentery.
Abbreviations: ER, emergency room; CT, computed tomography; OR, operating room; EAST, Eastern Association for the Surgery of Trauma
Case Report
A 38-year-old male presented to the emergency room (ER) with a chief complaint of abdominal pain. Onset of pain was three days prior, when he sustained an occupational accident. The patient was a tree cutter, and upon cutting down a large tree, his safety strap became entangled with the superior aspect of the falling tree trunk. The patient was pulled flush against the stump with the majority of the tree suspended from his safety strap, torquing his abdomen and back. He complained of nausea and a single episode of vomiting. He denied fever, chills, and dysuria. He did complain of a single episode of dark stool, although his stool was heme negative. Abdominal exam revealed focal tenderness in the peri-umbilical region without evidence of guarding or rebound. His laboratory data, which consisted of serum electrolytes and white blood cell counts, was normal. A computed tomography (CT) scan (Figure 1) was obtained which revealed a focal loop of thickened bowel alongside mild vascular congestion. However, the oral contrast was not impeded. He was admitted for observation based on his history and presenting symptoms; however, his constellation of clinical and radiological findings precluded him from emergent laparotomy.
Figure 1.
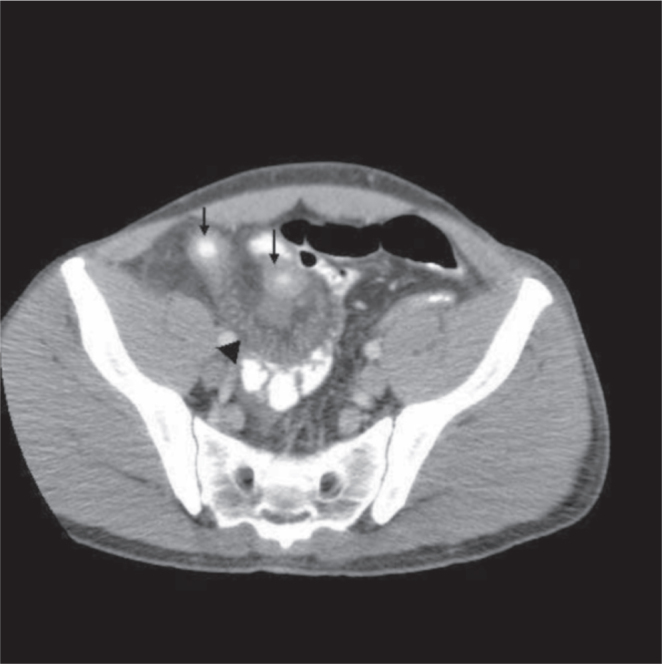
Contrast enhanced CT scan of the abdomen/pelvis in the axial plane showing thickened bowel (arrows) and mesenteric congestion (arrowhead). The contrast progressed distally. [Powerpoint Slide]
The patient's clinical course was essentially uncomplicated. He was closely monitored, gradually started on a diet and advanced progressively. Bowel activity was completely normal, and his pain was controlled with oral medication. He was subsequently discharged home on hospital day number three.
Thirteen days following his initial presentation, he presented back to the ER with complaints of abdominal pain and nausea, with four episodes of vomiting. He denied passing flatus and although he was afebrile in the ER, he reported fever spikes at home. His abdominal exam revealed a distended abdomen with tenderness appreciated predominantly in the peri-umbilical region. His white blood cell count was elevated to 14.6 thou/mcL. An abdominal x-ray (Figure 2) was obtained which showed markedly dilated bowel loops indicative of a bowel obstruction. This was followed by a CT scan (Figure 3) which depicted acute small bowel obstruction alongside mesenteric congestion and inflammation coupled with bowel wall enhancement and thickening, suggestive of bowel ischemia, acute infection and/or an acute inflammatory process. Based upon the history, constellation of physical findings and pertinent radiology, the patient was taken to the operating room (OR).
Figure 2.

Single anteroposterior abdominal radiograph showing markedly dilated small bowel. [Powerpoint Slide]
Figure 3.
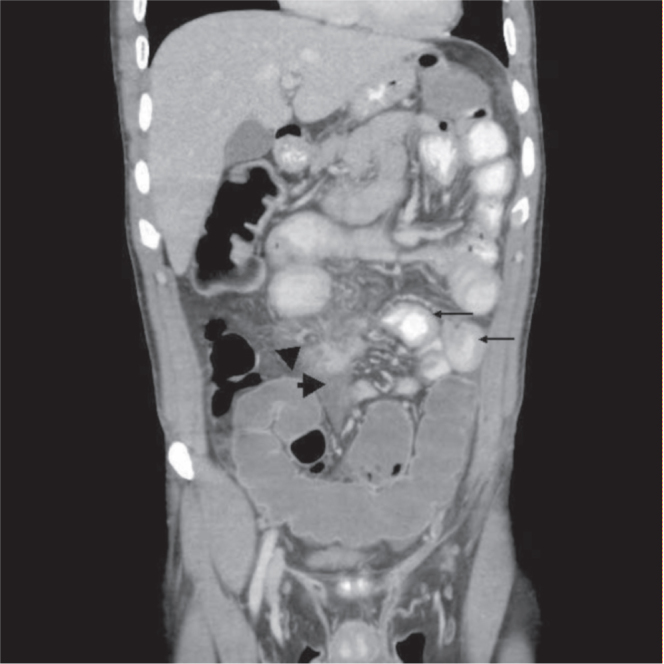
Coronal reformatted, contrast enhanced CT images of the abdomen/pelvis revealing thickened small bowel (arrows), induration and vascular congestion (arrowheads) seen along the adjacent mesentery with fat stranding, and dilated bowel. [Powerpoint Slide]
Upon entry into the abdomen there was some free fluid encountered. The small bowel was eviscerated from the abdominal cavity and the pathology was identified. Approximately 10 centimeters (cm) proximal from the ileocecal valve there was mesentery that was ecchymotic with a respective segment of bowel markedly thickened. A 3 cm mesenteric tear had been created where the patient had subsequently developed an internal hernia (Figure 4). Loops of small bowel and omentum had herniated through the defect with a single piece of omentum that had become compromised, compounding the small bowel obstruction (Figure 5). The inflamed small bowel was deemed nonviable, resected along with the ecchymotic mesentery and a primary anastamosis was created. The patient did well and was eventually discharged home on post operative day number four. His latest follow up, six weeks from initial surgery, did not reveal any complications, and he has since returned to his job.
Figure 4.
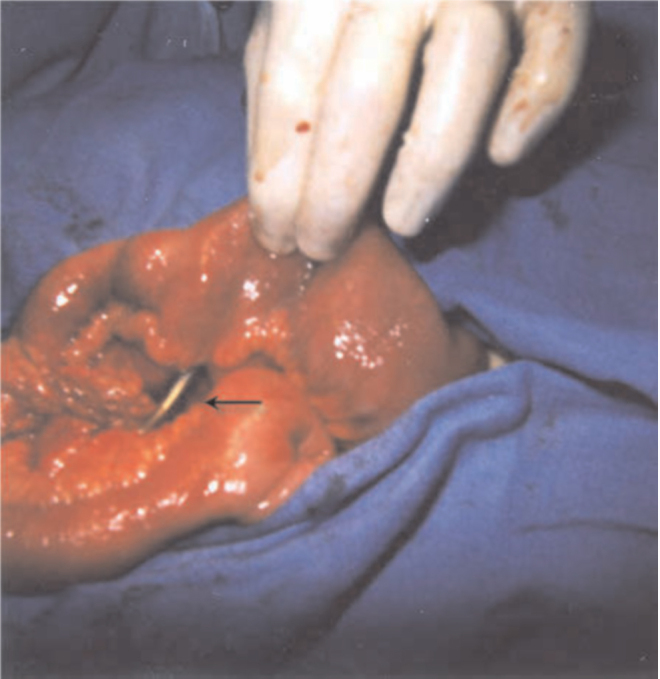
Gross image depicting the defect found in the mesentery where bowel had herniated through (arrow). [Powerpoint Slide]
Figure 5.
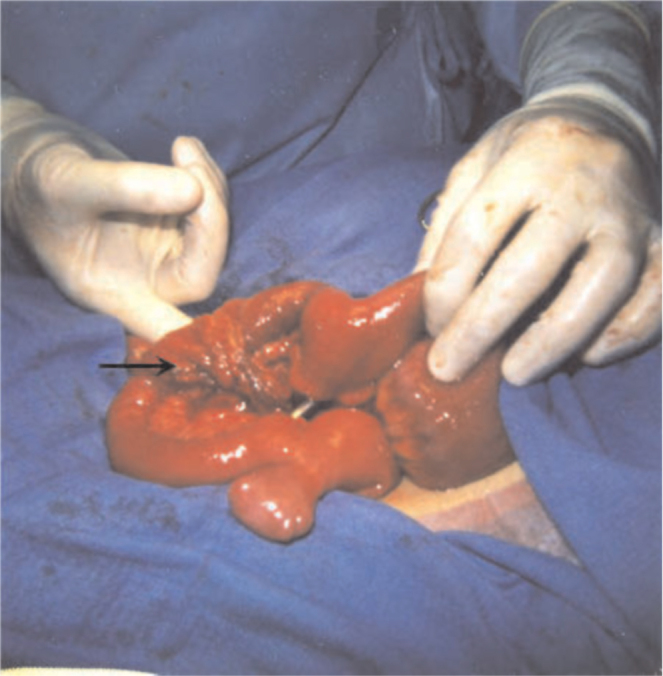
Internal hernia contents consisting of both bowel and omentum (arrow). [Powerpoint Slide]
Discussion
Small bowel injury does present as a possible complication from blunt abdominal trauma. The use of vehicular passenger restraints have been shown to contribute to small bowel injury with some reports revealing a 4.38 fold increase when compared to unrestrained passengers (1, 2). The “seat belt” sign was coined specifically to describe the ecchymosis in the abdomen outlining the position of the restraints (1). Small bowel perforation was higher in the restrained patients, however it must be underscored that restrained passengers presenting with seat belt signs and/or small bowel perforation would most certainly have died on the scene had they been unrestrained (3). The Eastern Association for the Surgery of Trauma (EAST) multi-institutional study associated seat belt sign with a 4.7 fold increase in the relative risk of bowel perforation (4). Mesenteric injuries, facilitating traumatic transmesenteric hernias, have been documented following blunt abdominal trauma secondary to a mesenteric rent (5).
Occult small bowel injury manifesting as delayed small bowel obstruction secondary to blunt abdominal trauma is uncommon. First reported in 1958, it was postulated that an underlying congenital defect in the mesentery was augmented by blunt trauma subsequently leading to symptomatic internal hernia formation (6). Currently, there exist several theories that have been added to explain the etiology of asynchronous small bowel obstruction. Mesenteric vascular injury can compromise a segment of bowel leading to a focal stenosis causing bowel obstruction (7). Subclinical bowel perforation, predisposing an acute inflammatory reaction and subsequent stricture formation, can precipitate a bowel obstruction (8). Direct injury to the small bowel wall can compromise the blood supply causing inflammation followed by stricture formation leading to a consequential bowel obstruction. Mesenteric tears from blunt abdominal trauma with small bowel herniations leading to bowel obstruction have also been reported (9).
Mesenteric hernias in the adult population stem primarily from gastrointestinal surgery, intraperitoneal inflammation and abdominal trauma (10). Surgical cases are attributed to iatrogenic complications especially following Roux-en-Y gastric bypass surgery where the hernia occurs through the transverse colon mesentery. Pre-operative diagnosis is difficult to ascertain because the clinical symptoms vary from mild intermittent discomfort to an acute onset of unrelenting abdominal pain (11).
Radiologically, the mesenteric defect is difficult to visualize. Diagnosis of asynchronous bowel obstruction hinges on the clinical exam and radiological data. The injury mechanism must be identified. However, it is the CT scan that confirms the diagnosis. A transition zone coupled with stenotic bowel loops, bowel wall thickening, and mesenteric congestion heighten the suspicion of bowel compromise. Mesenteric hematomas present with mural thickening indicative on computed tomography (7). Clustering of small bowel loops along with an engorged and congested mesenteric pedicle are suggestive of a tranmesenteric hernia, but are not pathognomonic (11). Small bowel barium evaluations have also been reported to depict the small bowel obstruction by outlining the focal stricture (12).
Importance of CT scans must be stressed, particularly once blunt trauma to the abdomen has been identified in the recent past. Management entails operative exploration once a diagnosis of small bowel obstruction is made. It is well documented that early operation improves survival and decreases morbidity (6, 13, 14). Our patient benefited from immediate CT scans and operative intervention by minimal bowel resection with subsequent discharge to his normal environment and occupation. We cannot underscore enough the importance of CT scanning and clinical examination in this cohort of patients that have suffered blunt abdominal trauma with a delayed presentation of symptoms.
Footnotes
Competing interests: The authors have declared that no competing interests exist.
Published: June 4, 2007
References
- 1.Appleby JP, Nagy AG. Abdominal injuries associated with the use of seatbelts. Am J Surg. 1989;157:457–458. doi: 10.1016/0002-9610(89)90633-8. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Anderson PA, Rivara FP, Maier RV, Drake C. The epidemiology of seatbelt-associated injuries. J Trauma. 1991;31:60–67. doi: 10.1097/00005373-199101000-00012. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Chandler CF, Lane JS, Waxman KS. Seatbelt sign following blunt trauma is associated with increased incidence of abdominal injury. Am Surg. 1997;10:885–888. [PubMed] [PubMed] [Google Scholar]
- 4.Watts DD, Fakhry SM, EAST Multi-Institutional Hollow Viscus Injury Research Group Incidence of hollow viscus injury in blunt trauma: an analysis from 275,557 trauma admissions from the East multi-institutional trial. J Trauma. 2003 Apr;54(4):749. doi: 10.1097/01.TA.0000046261.06976.6A. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Kuga T, Taniguchi S, Inoue T, Zempo N, Esato K. The occurrence of a strangulated ileus due to a traumatic transmesenteric hernia: report of a case. Surg Today. 2000;30(6):548–550. doi: 10.1007/s005950070126. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Mock CJ, Mock HE., Jr Strangulated internal hernia associated with trauma. AMA Arch Surg. 1958;77(6):881–886. doi: 10.1001/archsurg.1958.01290050051010. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Tsushima Y, Yamada S, Aoki J, Endo K. Ischaemic ileal stenosis following blunt abdominal trauma and demonstrated by CT. Br J Rad. 2001;74:277–279. doi: 10.1259/bjr.74.879.740277. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Maharaj D, Perry A, Ramdass M, Naraynsingh V. Late small bowel obstruction after blunt abdominal trauma. Postgraduate Medical Journal. 2003;79(297):57–58. doi: 10.1136/pmj.79.927.57. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Casey RG, Ryan J, Gillen P. Late presentation of small bowel obstruction following blunt abdominal trauma. Irish Journal of Medical Science. 2002;171(4):218–219. doi: 10.1007/BF03170285. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Hong SS, Kim AY, Kim PN, Lee MG, Ha HK. Current diagnostic role of CT in evaluating internal hernia. J Comput Assist Tomogr. 2005;29(5):604–609. doi: 10.1097/01.rct.0000168326.17363.b2. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Takeyama N, Gokan T, Ohgiya Y, Satoh S, Hashizume T, Hataya K, Kushiro H, Nakanishi M, Kusano M, Munechika H. CT of internal hernias. Radiographics. 2005;25(4):997–1015. doi: 10.1148/rg.254045035. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Chan SC, Chen HY, Lee CM, Tsai CH. Small bowel stenosis from blunt abdominal trauma. International Journal of Clinical Science. 1997;51(6):404–405. [PubMed] [PubMed] [Google Scholar]
- 13.Maull KI, Reath DB. Impact of early recognition on outcome in nonpenetrating wounds of the small bowel. 1984;77(9):1075–1077. doi: 10.1097/00007611-198409000-00004. [PubMed] [DOI] [PubMed] [Google Scholar]
- 14.Xeropotamos NS, Nousias VE, Ioannou HV, Kappas AM. Mesenteric injury after blunt abdominal trauma. European Journal of Surgery. 2001;167(2):106–109. doi: 10.1080/110241501750070547. [PubMed] [DOI] [PubMed] [Google Scholar]