

Abstract
Objective
Informed consent forms that are used prior to administering anaesthesia inform patients before any proposed surgical procedure or treatment. They should provide patients with sufficient information about the operation and treatment. Readibility refers to whether it is easy or hard for a reader to read and understand an available text, and this is evaluated via various formulas. The aim of this study was to evaluate the readability of different informed consent forms commonly used in the anaesthesiology departments of different hospitals in our country using different readability formulas.
Methods
After obtaining ethics committee approval, the readability of different consent forms used in the anaesthesiology departments of university hospitals (n=15), Ministry of Health (MOH) education and research hospitals (n=15), and public hospitals (n=15) was analysed. Each consent form was displayed electronically in “Microsoft Word” and the number of words contained was counted automatically. The first 100 words on the first page of the forms were evaluated using the Gunning Fog, Flesch-Kincaid and Ateşman readability formulations. The rate of medical terms detected within these 100 words was determined as a percentage (%).
Results
Different consent forms obtained from 45 anaesthesia departments were assessed using various readability formulas. According to the Gunning Fog index, the readability of the consent forms obtained from MOH education and research and public hospitals was relatively low. The Flesch-Kincaid index measured very low levels of readability in all institutions. The Ateşman index displayed very low readability levels for the consent forms used in university hospitals, and low levels in other institutions.
Conclusion
We conclude that the readability of the anaesthesia informed consent forms is low. The level of education in our country should be considered in the preparation of anaesthesia consent forms. We believe that physicians should pay more attention to this medical and legal issue.
Keywords: Informed consent forms, anaesthesia, medical legislation
Introduction
Readability is a concept specific to language, and was developed in the early 19th century in the United States of America (1).
Briefly, readability gives information on the characteristics of syllables, words and sentences of the relevant language as well as whether the text is easily understandable by a reader with a certain level of intelligence by introducing some quantitative data concerning the texts. In the past, this concept had been mostly used in interacademic correspondence, military institutions and health organizations (2). The factors that influence readability include mean word length, word frequency, number of words with multiple syllables, mean sentence length, number of words with multiple meanings and mean number of syllables. Readability of a sentence decreases as the number of words in the sentence increases (3).
Readability formulas have been developed to assess the readability using measures such as length of words and sentences and number of syllables in a word. There are more than 40 formulas to analyse readability. The most commonly used readability formulas include Gunning fog index, Flesch-Kincaid readability formula, and Ateşman readability formula.
Literature review in English and Turkish revealed no study that investigated the readability level of anaesthesia consent forms.
The present study aimed to assess the readability level of informed consent forms that are used prior to anaesthesia in Turkey, using readability formulas.
Methods
The present study was carried out between 01.01.2013 and 05.06.2013 with the approval of “Dokuz Eylül University Medical Faculty, Ethics Committee for Non-interventional Research”.
In Turkey, each hospital has anaesthesia consent forms, developed according to certain standards. Anaesthesia consent forms used in the anaesthesiology departments of the universities (n=15), ministry of health training and research hospitals (n=15) and state hospitals (n=15) in Turkey were obtained and readability index for each form was calculated. Anaesthesiology chairman of each institution was contacted via e-mail or phone call and was informed about the study. Pre-anaesthesia consent forms were requested from the institutions participated in the study.
Each consent form was visualized by “Microsoft Word” program and the words were automatically counted. Readability level of each consent form was assessed by Gunning Fog index, Flesch-Kincaid Readability Formula and Ateşman Readability Formula. The first 100 words of the consent forms was automatically analysed by an “online calculator”. Calculations were made also manually to check the accuracy of the results obtained.
For Gunning Fog index measurement, the first 100 words of the text was taken and the proportion of three-syllable words and mean word count were calculated; the results were entered in the Gunning Fog Formula. Assessment according to education levels is a characteristic of Fog index.
Fog Index= 0.4× (proportion of words with three syllables + mean word count)
Proportion of words with three syllables=(number of words with three and more syllables/number of words remained) ×100
Mean Word count=number of words/number of sentences.
A result between 8 and 10 indicates that it is an easy text, but a result higher than 11 indicates that it is a difficult text (4).
For the Flesch-Kincaid formula, the first 100 words of the text were taken and calculation was made by determining word length and sentence length (Table 1).
Table 1.
Readability level according to Flesch-Kincaid Formula
| Level of the text | Mean sentence length | Mean number of syllables | Level of the text (numerical) | Estimated level |
|---|---|---|---|---|
| Very easy | 8 and lower | 123 and lower | 90–100 | 5 |
| Easy | 11 | 131 | 80–90 | 6 |
| Quite easy | 14 | 139 | 70–80 | 7 |
| Standard | 17 | 147 | 60–70 | 8–9 |
| Quite difficult | 21 | 155 | 50–60 | 10–11 |
| Difficult | 25 | 167 | 30–50 | 13–16 |
| Very difficult | 29 + | 192 + | 0–30 | adults |
Flesch-Kincaid Reading ease= (0.39× sentence length)+(1.18× word length)-15.59
Word length=number of syllables/number of words
Sentence length=number of words/number of sentences
The text is considered easy as the number of syllables for each word becomes closer to 1; whereas the text is considered difficult as the number of syllables for each word becomes closer to 10. The same is also valid for a sentence; the text is considered easy as the number of words becomes closer to 1, whereas the text is considered difficult as the number of words becomes closer to 10 (1).
Finally, for the calculation of Ateşman Readability Index, calculation was made over the formula by taking the first 100-words of the text. According to this formula, a text is easy as the readability level becomes closer to 100, but difficult as the readability level becomes closer to 0 (Table 2) (5).
Table 2.
Ateşman Turkish readability intervals
| Level | Readability interval |
|---|---|
| Very easy | 90–100 |
| Easy | 70–89 |
| Moderately difficult | 50–69 |
| Difficult | 30–49 |
| Very difficult | 1–29 |
RN=198.825-(40.175.X1)-(2.610.X2)
RN: readability number
X1: number of syllables/number of words
X2: number of words/number of sentences
Additionally, the proportion of medical terms was determined in percentages (%) by counting the number of medical terms in the first 100 words of the forms.
Statistical analysis
Results were analysed using statistical analysis and data evaluation programs, and mean readability index and mean proportion of medical terms were determined. Statistical Package for Social Sciences version 15 (SPSS 15.0, Chicago, IL, USA) program was used for statistical analysis. Data were presented as median and interquartile range (25%–75%). Groups were compared using Mann-Whitney U test. A p value <0.05 was considered significant for all analyses.
Results
The present study comprised informed consent forms of 45 institutions in Turkey. None of the consent forms was excluded. Data about consent forms are presented in Table 3. No significant difference was observed between the forms obtained from different types of institutions in terms of mean number of letters, syllables, words and sentences. The number of words with three and more syllables was significantly higher in forms obtained from university hospitals as compared to those obtained from state hospitals (p<0.05). According to Gunning fog index, readability level of university consent forms was significantly higher in comparison to that of state hospitals (p<0.05). However, readability level of the consent forms of research and training hospitals and state hospitals were also low. All forms displayed a very low readability level according to Flesch-kincaid formula. According to the Ateşman’s formula, readability level of university hospital forms was significantly lower as compared to that of the training hospitals (p<0.05). According to the Ateşman’s formula, the mean readability level of all forms was 33.2 (26.0–37.0). The rate of medical terms was 4% with no difference determined between the institutions.
Table 3.
Readability grades of consent forms [median (25%–75%)]
| Overall forms (n=45) | University Hospital (n=15) | Training and Research Hospital (n=15) | State Hospital (n=15) | |
|---|---|---|---|---|
| Number of sentences | 7 (6–9) | 7 (5–10) | 8 (6–8) | 7 (6–9) |
| Number of words with 3 and more syllables | 67 (62.5–70.5) | 69 (65–74) | 68 (61–70) | 65 (57–68) |
| Number of words | 100 (100–102) | 100 (100–104) | 100 (100–103) | 101 (99–102) |
| Number of letters | 732 (712–771) | 731 (710–781) | 722 (705–747) | 743 (716–772) |
| Number of syllables | 324 (311–340) | 325 (312–343) | 322 (311–330) | 331 (311–338) |
| Gunning fog index | 22.9 (8.2–25.2) | 9.9 (7.1–23.7)* | 19.5 (7.4–25) | 25.0 (23.1–25.9) |
| Flesch-kincaid index | 20.5 (18.9–21.9) | 19.9 (19–21.8) | 19.5 (17.7–21.5) | 21.4 (20.1–22.1) |
| Ateşman readability | 33.2 (26.0–37.0) | 28.3 (21.3–34.7) | 35.7 (29.9–37.2) | 34.4 (26–38.4) |
| Proportion of medical terms (%) | 4 (3.5–6.5) | 4 (4–6) | 4 (4–6) | 4 (2–7) |
p<0.016. Significant difference between University Hospitals and State Hospitals. Mann-Whitney U test
Discussion
Informed consent forms that are being used prior to anaesthesia are the forms prepared to inform the patient of a surgical procedure or intervention that he/she would undergo. They are one of the bases of relationship between patient and physician. Therefore, it is important that the informed consent forms are clearly understood by the patient. The present study investigated the readability level of anaesthesia consent forms used in the hospitals of Turkey.
It is not sufficient for physicians to only follow the most recent medical information while performing their skills. Medical jurisprudence and medical ethics, which are the other components of medical practices, are also the determinants of practice (6).
Knowing professional legislation is as important as acting in accordance with standard practices pre-specified in anaesthesia and reanimation field.
The legal dimension of patient-physician relationship begins with the referral of the patient to physician and the initiation of diagnostic testing and treatment. In this case, legally, an invisible proxy agreement develops between patient and physician. The physician performs his/her profession in diagnosis, treatment and any kind of intervention within “permitted risk”, i.e. certain rates of “complication”, as long as he/she follows all these rules in the proxy agreement (7–9). It is necessary to inform the patient about “complications” that might occur during anaesthesia and reanimation procedures and to obtain the patient’s consent separately for each intervention. Informed consent form is a mandatory form that should be completed in accordance with the article 17 of the Constitutional Law, articles No. 26, 90, 91, 99 and 101 of the Turkish Criminal Law (TCL) No. 5237, article No. 70 of the “The Law on the Practice of Medicine and Related Arts” no 1219, articles No. 6 and 7 of the law No. 2238 on “Removing, Keeping Inoculating and Transplanting Organs and Tissues”, article No. 8 of the law on the “Regulation of Drug Research”, article No. 14 of “Regulation on Medical Deontology”, articles No. 26 and 27 of “Medical Practice Ethics Code”, articles No. 7, 15, 18, 19, 20, 22, 24, 25, 26, 27, 28, 29, 31, 32, 33, 34, and 35 of “Regulations on Patient Rights”, annex No. 4 of “Regulation on the Treatment Centres for Assisting Reproduction” and annex No. 3 of “Regulation on Genetic Diseases Diagnoses Centres”.
With the informed consent form, the physician must obtain the written consent of the patient after informing the patient about patient’s current health status, recommended treatment methods, likelihood of success of treatment methods, duration and risks, the use of medications and potential side effects, alternative ways of treatment and probable consequences in case recommended treatment is not accepted, and intervention and surgery that the patient would undergo. In case of emergency conditions where the patient is unable to give written consent, in unconscious patients, and in case the patient has not attained majority; written consent must be obtained from the legal guardian or legal representative of the patient (6, 7, 9–12).
Consent forms should be written in a simple, plain but understandable language and should include adequate information. Therefore, the patient needs to understand well the point in this form and to decide whether he/she would give consent or not.
Today, readability has become a universal concept, on which linguists study intensively (4).
According to Chall (13), readability studies have been made for the language to become more understandable. If a text comprises numerous unknown words and if these words are frequently repeated in that text, the text becomes difficult to read.
The Gunning Fog index is an assessment tool that is based on sentence length and the ratio of the percentage of words with multiple syllables (14). The present study found the readability level of university consent forms to be easy and that of training and state hospitals to be difficult according to the Gunning fog formula (Figure 1).
Figure 1.
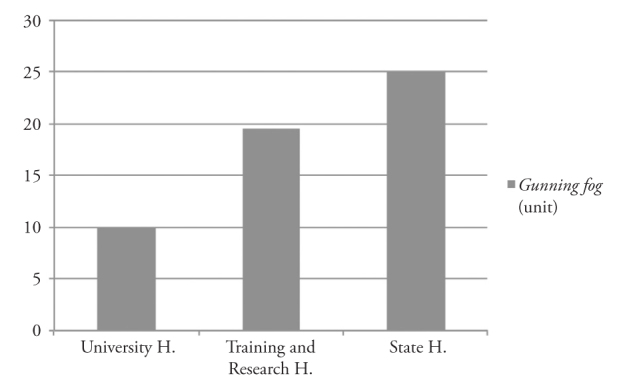
Readability grades of consent forms determined by Gunning fog formula according to institutions (the readability of the text gradually becomes difficult in texts >10 units)
H: hospital
This result was not consistent with the results that we obtained using other readability formulas. Chall (13) reported that a formula that was developed structurally for a different language might not give the same results for another language.
Therefore, in the present study, we mainly considered “Ateşman readability formula” of Flesch, which was adapted into Turkish by Ateşman (5), although we also used the other formulas.
According to Ateşman (5), readability is the texts’ being easy or difficult to understand for the reader. However, there are some differences between readability and understandability. Both qualitative and quantitative characteristics should be considered while scrutinizing the texts. Text content is of great importance for understandability, i.e. the order of the words and the way the idea is explained is important. Short and clear words with generally known meaning should be used and the words should not be repeated frequently.
In readability, grammatical characteristics of texts and length of words and sentences are taken into account. In the present study, readability level according to the Ateşman formula was very low in the university consent forms and low in the training and state hospital consent forms. The present study took the Ateşman formula, the unique readability formula adapted into Turkish, as the basis. This indicates that consent forms in the university hospitals, which are at certain academic level, have been prepared at academic level.
Flesch-kincaid index is one of the most frequently used methods; length of words and sentences is important and it indicates education level. For example, if the result is 8.6, it means that the text addresses the individuals with an education level of 8 years (15).
According to this formula, the present study determined very low readability levels for all consent forms. This was consistent with the results obtained by Ateşman’s formula (Figure 2). It was determined that anaesthesia consent forms address the individuals at academic education level. Sharp (16) reported that oncological information forms are too long and difficult for patients to understand what they read.
Figure 2.
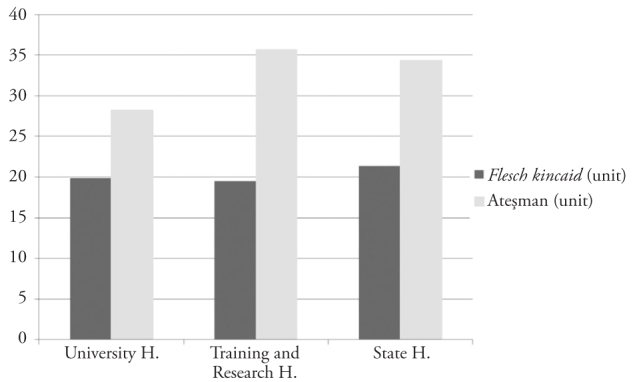
Readability grades of consent forms determined by Flesch kincaid and Ateşman formulas according to institutions (0–30 units: very difficult; 30–50 units: difficult)
H: hospital
In general, studies suggest a relation between education and comprehension level. Identifying the education level at which a text is written gives certain information about its understandability. Anaesthesia consent forms must be understandable for patient population of all education levels. A cancer institution in the USA recommended preparation of information forms according to 8-year education level (17).
Information forms may lead to misunderstanding for an individual that is not familiar with medical terms even though she/he has a high education level. Therefore, consent forms should not include medical terms as far as possible. In the present study, the rate of medical terms was very low as 4%.
According to 2010 data from Turkey, the mean education level of the population aged over 15 years was reported to be 7.18 years, whereas the mean education level of females over the age of 15 years was 6.33 years (18).
While preparing anaesthesia consent forms, attention must be paid for the forms to be understandable in the way to comprise patient population of the lowest education level.
The present study comprised 45 institutions from Turkey. Therefore, the results of this study hardly reflect the situation in Turkey. It would be appropriate to give information on the general status in our country by further large-scale studies.
Conclusion
Although readability tests do not give definite results on understandability of the text, they give some idea on the level of text. In conclusion, the present study determined that readability levels of anaesthesia consent forms used in Turkey are quite low. Education level in Turkey must also be taken into account while preparing anaesthesia consent forms. We think that care must be taken about this subject, which medically and legally binds the physicians.
Footnotes
Ethics Committee Approval: Ethics committee approval was received for this study from the ethics committee of Dokuz Eylül University School of Medicine Non Interventional Research Ethics Commitee.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - V.H., N.B.; Design - V.H., N.B., A.G.; Supervision - A.G.; Funding - N.B.; Materials - V.H., N.B., S.Ö., Ş.Ö.; Data Collection and/or Processing - N.B., Ş.Ö., S.Ö., G.A., V.H.; Analysis and/or Interpretation - N.B., V.H., E.Ö.; Literature Review - N.B.; Writer - N.B., V.H.; Critical Review - A.G.; Other - G.A., E.Ö.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.DuBay WH. “The Principles of Readability”, Costa. Mesa, CA: 2004. [Google Scholar]
- 2.Hedman AS. Using the SMOG Formula to revise a health. Am J Health Edu. 2008;39:61–4. http://dx.doi.org/10.1080/19325037.2008.10599016. [Google Scholar]
- 3.Al-Ajlan AA, vd. Towards the development of an automatic readability measurements. 3rd Int Conf Digi Inf Mng (ICDIM); 2008. pp. 506–11. [Google Scholar]
- 4.Goldbort R. Readable writing by scientists and researchers. J Environ Health. 2001;63:40–1. [PubMed] [Google Scholar]
- 5.Ateşman E. Measuring readability in Turkish. A.U. Tömer Language Journal. 1997;58:171–4. [Google Scholar]
- 6.Güzeldemir ME. The importance of informing patients. Syndrome. 2005;17:36–53. [Google Scholar]
- 7.Atalay H, Hancı V. Ethical and legal responsibilities in intensive care infections. In: Yalçın AN, Erbay RH, editors. Infections in an intensive care unit. 1st Edition. Nobel Tıp Kitabevi; Istanbul: 2009. pp. 271–9. [Google Scholar]
- 8.Çelik M. Legal responsibilities of anaesthesia and reanimation specialist. Turkish Anest Rean Soc Journal. 2002;30:100–4. [Google Scholar]
- 9.Günerli A. Professional and Legal Responsibilities of Anaesthesiologists, Legal Decrees, Relevant Legislation and Bylaws. J Turk Anaesth Int Care. 2009;37:333–49. [Google Scholar]
- 10.Özaslan A. Sempozyum Kitabı. Istanbul: I. U Cerrahpaşa Medical Faculty Publications; 2006. Informed Consent. Legal and criminal liability of physicians in the context of new laws, medical malpractice and regulation of forensic report; pp. 43–54. [Google Scholar]
- 11.Elmacı İ, Balak N, Bozkuş H, Kaynar MY, Ulu O, Asan Z, et al. In: Guide for informed consent for neurosurgery. 1. Basım. Ak H, editor. Turkish Neurosurgical Society Publications, Buluş Press; Ankara: 2006. pp. 5–38. [Google Scholar]
- 12.Öztürk R. Legal responsibilities in nosocomial infections. Sağlıkta Nabız Dergisi. 2006;5:40–4. [Google Scholar]
- 13.Chall JS. In: Readibility: The Beginning Years. Zakaluk B, Samuels SJ, editors. International Reading Association Inc; 1988. pp. 3–4. [Google Scholar]
- 14.Ertem-Vehid H, Giresunlu M, Köksalan H. Evaluation of patients’ inform consent forms in oncology: readability of the information. Türk Onkoloji Dergisi. 2006;21:187–90. [Google Scholar]
- 15.Cherla DV, Sanghvi S, Choudhry OJ, Liu JK, Eloy JA. Readability assessment of Internet-based patient education materials related to endoscopic sinus surgery. Laryngoscope. 2012;122:1649–54. doi: 10.1002/lary.23309. http://dx.doi.org/10.1002/lary.23309. [DOI] [PubMed] [Google Scholar]
- 16.Sharp SM. Consent documents for oncology trials: does anybody read these things? Am J Clin Oncol. 2004;27:570–5. doi: 10.1097/01.coc.0000135925.83221.b3. http://dx.doi.org/10.1097/01.coc.0000135925.83221.b3. [DOI] [PubMed] [Google Scholar]
- 17.Simplification of informed consent documents: Recommendations. National Cancer Institute; Available at: www.nci.nig.gov/clinicaltrials/understanding/simplification-of-informed-consent-documents. [Google Scholar]
- 18.Barro R, Lee JW. Educational Attainment Dataset. [17 June 2013]. 2011. [Online] Available at: http://www.barrolee.com/