

Abstract
We present the case of a 35-year-old man with a hemangioma in the iliac wing that simulated an aggressive bone lesion on CT, MRI, and bone scintigraphy. On CT, the lesion, 12 cm in in maximum dimension, was expansile and septated. On MRI, the lesion was isointense with respect to muscle on T1 weighted images, and hyperintense on T2 images, with focal regions of cortical breach. Radionuclide bone scan showed increased tracer accumulation. The diagnosis was made following surgical biopsy, and the lesion was treated conservatively.
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging
Introduction
Hemangioma is frequently detected and diagnosed by cross-sectional imaging as incidental finding in the thoracic and lumbar spine. Less frequently, hemangiomas are found in the calvaria, and rarely in the appendicular skeleton. We present a case of hemangioma in the iliac wing that simulated an aggressive bone lesion on CT, MRI, and bone scintigraphy.
Case Report
A 35-year-old man presented with a four-year history of right hip pain and disability exacerbated by physical activity and weightbearing. The patient denied any prior trauma. He did not have any fever, chill, night sweat or weight loss. Right hip radiographs showed an expansile and septated lesion affecting the right acetabulum. Pelvic CT confirmed the large and aggressively appearing acetabular lesion with diffuse trabecular destruction. The tumor had cortical bone expansion with multiples foci of osseous erosion and disruption (Figure 1A, Figure 1B, Figure 1C, arrows). The tumor measured 8 × 5 × 12 cm extending from the inferior ilium to the ischium without definite adjacent soft tissue invasion. MRI showed a large lesion of the left iliac bone involving the acetabulum and ischium (Fig. 2, arrows). The mass was isointense to muscles on T1-weighted images and hyperintense on T2-weighted sequences. Cortical breaches were detected at the medial aspect of the acetabulum and iliac bone. There was no hip joint mass or effusion. Since CT and MRI showed features of an aggressive tumor, bone scan was obtained for search of potential metastasis. The whole body technetium-99m MDP scintigraphy showed increased radiotracer uptake of the right acetabulum and right ischium (Fig. 3, arrows) but did not detect any additional osseous lesion. An initial CT-guided bone biopsy showed rare fragments of reactive woven bone, several irregular aggregates of spindle cells with round to oval shaped nuclei, bland-appearing chromatin patterns and no apparent mitotic figures. The spindle cells were in a fibromyxoid matrix with presence of scattered thin-walled blood vessels and rare giant cells. There was no histologic evidence of plasmacytoma or giant cell tumor. This CT-guided biopsy was not diagnostic but favored a low-grade neoplasm. A subsequent surgical open biopsy reached the diagnosis of iliac bone hemangioma. Due to the large size of the tumor, a conservative approach was observed. Close follow-up for two years showed continuously increasing pain requiring radiation therapy. Additional two-year posttherapeutic monitoring witnessed clinical improvement with stability of the iliac hemangioma on cross-sectional imaging.
Figure 1A.

35-year-old man with hemangioma of the right iliac wing. A, Axial CT-guided biopsy image of the right pelvis showed an expansile and septated lesion involving the iliac bone. There are foci of cortical erosion and destruction at the medial aspect of the right acetabulum (arrows).
Figure 1B.
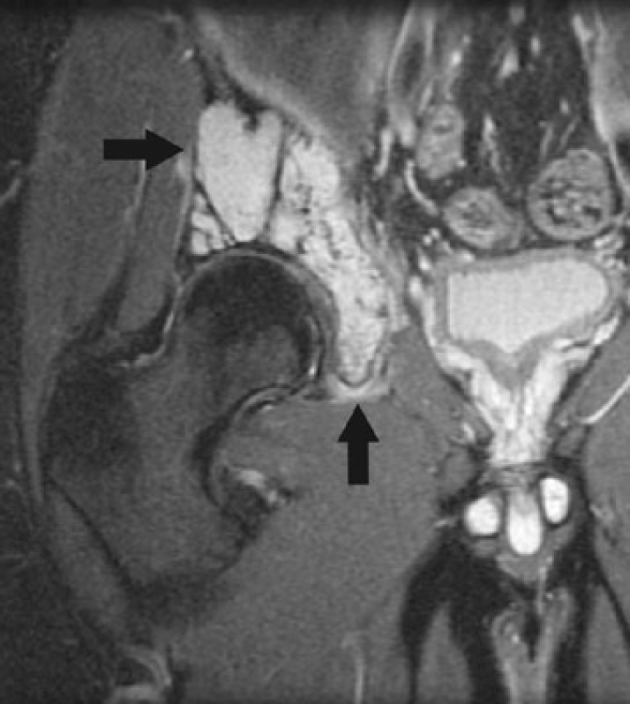
35-year-old man with hemangioma of the right iliac wing. B, Coronal MR T2-weighted fat-suppressed image of the right pelvis showed high signal intensity of the hemangioma extending from the low ilium to the ischium without invasion of the right hip joint (arrows)
Figure 1C.
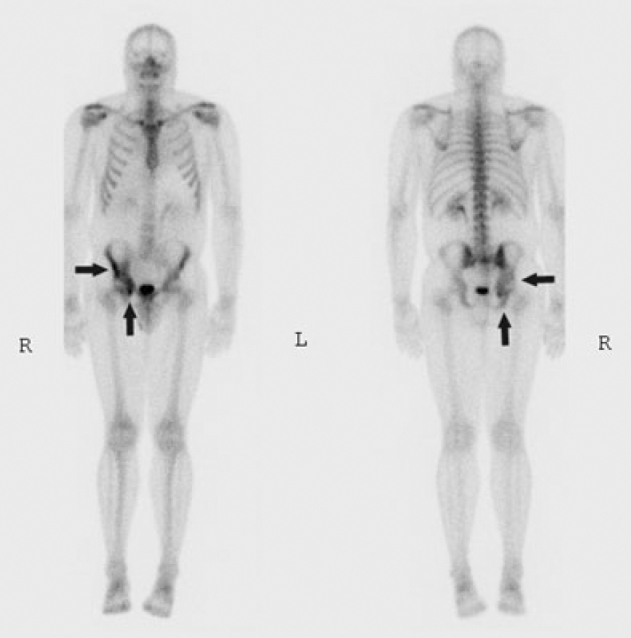
35-year-old man with hemangioma of the right iliac wing. C, Technetium-99m MDP whole body bone scintigraphy in the anterior and posterior projections showed a large focus of radiotracer uptake at the lower aspect of the right iliac wing, acetabulum and ischium (arrows).
Discussion
Osseous hemangiomas are rare and represent about 1% of all bone tumors [1, 2]. The majority of these benign bone lesions, close to 80%, are encountered in the spine especially thoracic and lumbar, and cranio-facial bones. Tubular and long bone sites account for 10% of the total. Pelvic bone hemangioma is uncommon, seen only in 3-4% of all cases [3, 4, 5, 6]. Intraosseous hemangiomas are usually seen in a middle-aged patient population with female gender predilection even though they can occur at extreme ages of both sexes. Their pathogenesis may be secondary to congenital, developmental or acquired vascular proliferations [7]. Incidental finding is frequent on cross-sectional imaging for the majority of osseous hemangiomas, which are asymptomatic. A small percentage of these benign tumors are detected secondary to pain symptomatology related to their weight-bearing location such as pelvic girdle and lower extremities [6, 8].
Classic radiographic patterns include bone demineralization with coarsely prominent vertical trabeculae and corduroy appearance. CT usually shows well-marginated focal areas of decreased bone attenuation with polka-dot or honeycomb appearance. MR frequently demonstrates high signal intensity on T2 weighted sequences and variable degrees of increased signal intensity on T1-weighted images depending of the vascular and fat components of the lesion [2]. Sunburst and spoke-wheel features may be seen with calvarial hemangiomas, which are multiple in 15% of the cases [3]. Similar to this case presentation, osseous hemangiomas may mimic malignant neoplasms with aggressive looking patterns of cortical bone expansion and destruction. The unusual pelvic and appendicular bone sites with atypical imaging features and pronounced clinical symptomatology would heighten the suspicion for malignancy. Technetium-99m MDP bone scintigraphy is non-specific with either variable degrees of radiotracer uptake or absence of tracer accumulation [9, 10, 11, 12].
As seen in other rare cases of hemangiomas around the hip joint, the differential diagnosis includes a large spectrum of expansile lytic lesions such as aneurysmal bone cyst, eosinophilic granuloma, fibrous dysplasia, giant cell tumor, plasmacytoma, brown tumor, malignant fibrous histiocytoma, and metastasis. Correct histological tumor identification is necessary for treatment. Routine biopsy may be challenging and non-contributory due to insufficient material. En-bloc open biopsy should provide adequate specimen showing dilated vascular channels lined with endothelial cells characteristic of hemangioma. Large skeletal hemangiomas may be prone to osseous deformities at weight-bearing sites, pathologic fractures, spontaneous bleed, iatrogenic hemorrhage secondary to biopsy or surgery, and malignant degeneration [6]. Treatment is conservative for asymptomatic and small hemangiomas. Surgery by curettage and bone graft is indicated for small symptomatic ones. Large symptomatic or incompletely resected hemangiomas may benefit from radiation therapy with long term improvement of symptoms and tumor shrinkage [13]. Other interventional options include embolization and ethanol tumor injection [1].
Footnotes
Published: August 13, 2007
References
- 1.Kaleem Z, Kyriakos M, Totty WG. Solitary skeletal hemangioma of the extremities. Skeletal Radiol. 2000 Sep;29(9):502–513. doi: 10.1007/s002560000251. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Ogose A, Hotta T, Morita T, Takizawa T, Ohsawa H, Hirata Y. Solitary osseous hemangioma outside the spinal and craniofacial bones. Arch Orthop Trauma Surg. 2000;120(5-6):262–266. doi: 10.1007/s004020050461. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Wenger DE, Wold LE. Benign vascular lesions of bone: radiologic and pathologic features. Skeletal Radiol. 2000 Feb;29(2):63–74. doi: 10.1007/s002560050012. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Puig J, Garcia-Pena P, Enriquez G, Huguet P, Lucaya J. Intraosseous haemangioma of the ilium. Pediatr Radiol. 2006 Jan;36(1):54–56. doi: 10.1007/s00247-005-0005-1. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Kozlowski K, Campbell J, Beluffi G. Rare, primary iliac, pubic and ischial tumours in children (report of 14 cases)–Part II. Australas Radiol. 1989 Nov;33(4):361–368. doi: 10.1111/j.1440-1673.1989.tb03313.x. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Rao SB, Crawford AH. Acetabular protrusion secondary to pelvic hemangioma. A case report and review of the literature. Clin Orthop Relat Res. 1994 Sep;(306):209–212. [PubMed] [PubMed] [Google Scholar]
- 7.Woertler K. Benign bone tumors and tumor-like lesions: value of cross-sectional imaging. Eur Radiol. 2003 Aug;13(8):1820–1835. doi: 10.1007/s00330-003-1902-z. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Chawla A, Singrakhia M, Maheshwari M, Modi N, Parmar H. Intraosseous haemangioma of the proximal femur: imaging findings. Br J Radiol. 2006 Oct;79(946):e129–e132. doi: 10.1259/bjr/53131368. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.Halkar RK, Motawy MM, Hebbar HG. Vertebral body hemangioma showing increased uptake of Tc-99m MDP and decreased Tc-99m labeled red blood cells. Clin Nucl Med. 1994 Sep;19(9):827–828. doi: 10.1097/00003072-199409000-00022. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Makhija M, Bofill ER. Hemangioma, a rare cause of photopenic lesion on skeletal imaging. Clin Nuc Med. 1988 Sep;13(9):661–662. doi: 10.1097/00003072-198809000-00012. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Han BK, Ryu JS, Moon DH. Bone SPECT imaging of vertebral hemangioma: correlation with MR imaging and symptoms. Clin Nucl Med. 1995 Oct;20(10):916–921. doi: 10.1097/00003072-199510000-00014. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Reader DW, Pozderac RV. Vertebral hemangioma presenting as a cold defect on bone scintigraphy. Clin Nucl Med. 2001 Oct;26(10):868–869. doi: 10.1097/00003072-200110000-00016. [PubMed] [DOI] [PubMed] [Google Scholar]
- 13.Schild SE, Buskirk SJ, Frick LM, Cupps RE. Radiotherapy for large symptomatic hemangiomas. Int J Radiat Oncol Biol Phys. 1991 Aug;21(3):729–735. doi: 10.1016/0360-3016(91)90693-x. [PubMed] [DOI] [PubMed] [Google Scholar]