

Abstract
Thoracoscopy has major advantages over thoracotomy. We report a successful management of foregut duplication cyst thoracoscopically in a child with review of literature.
Keywords: Cyst, duplication, foregut, pediatric thoracoscopy
INTRODUCTION
Esophageal duplication cysts are infrequent anomalies of the gastrointestinal tract that are predominantly found in children. The conventional approach for removal of these cysts is an open surgery. However, more recently, these cysts have been excised thoracoscopically.[1] A case of complete thoracoscopic excision of esophageal duplication cyst is presented along with review of literature.
CASE REPORT
A 9 years male child was referred with suspected lesion on screening chest X-ray, which was ordered for persistent cough [Figure 1]. Contrast enhanced computerized tomography chest revealed well defined homogenously enhancing thin walled lesion in middle mediastinum and right paratracheal region suggestive of foregut duplication cyst. Thoracoscopic excision of cyst was planned. General anesthesia with single lung ventilation was used (selective occlusion of the right main bronchus by bronchial blocker under flexible bronchoscopy guidance). The child was placed in modified prone position. Three ports were inserted at posterior axillary, mid-axillary, and midway between spine and posterior axillary. Because of partial collapse of the lung, low-pressure insufflation (5 cm of water and flow at 0.5-1.0 L/min) was used. A 3 cm × 3 cm cyst in the right paratracheal region was seen. Cyst was dissected from the esophagus with hook cautery and Harmonic® as an energy source [Figure 2a and b]. Cyst was excised leaving back a part of cyst wall over the esophageal surface. The mucosa over the wall was ablated and the cyst was delivered out through one of the port sites. The esophageal wall was approximated and then air was pushed into the esophagus along with some saline into the thoracic cavity to see for any leak. None was seen. The bronchial blocker was deflated and pulled back. No air leak was identified and lung expanded. Intercostal drainage tube was placed as intraoperative single lung ventilation was used and also to identify any missed esophageal perforation. The patient was extubated immediately after surgery, and recovery was uneventful. Nasogastric tube and intercostal drainage tube was removed after 24 h and patient was gradually started on full oral diet by 2nd postoperative day. Chest X-ray after chest drain removal showed full lung expansion. Histopathology confirmed as esophageal duplication cyst.
Figure 1.
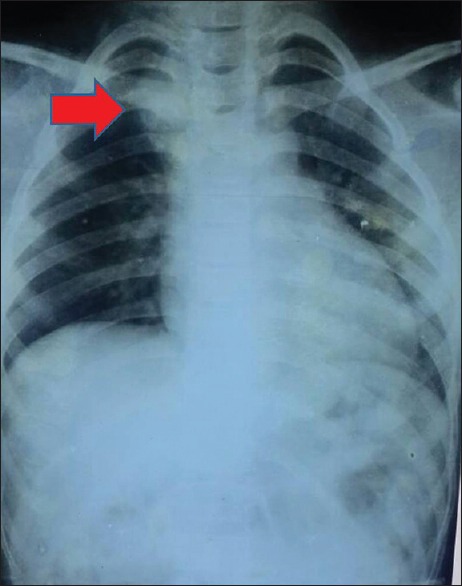
Chest X-ray showing right paratracheal mass
Figure 2.
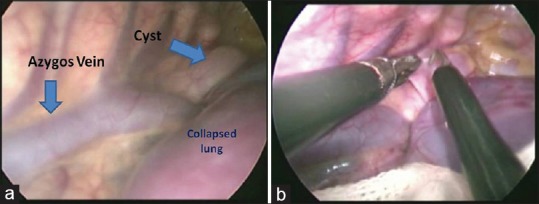
(a) Cyst in relation to azygos vein and lung. (b) Cyst being dissected
DISCUSSION
Open surgical resection via posterolateral thoracotomy has been the standard surgical approach for the excision of foregut duplication cyst. However, currently, video-assisted thoracoscopic surgery (VATS) has been a preferred approach.[2] VATS offers numerous advantages as compared to open procedure as it reduces postoperative pain, helps in early recovery, reduces hospital stay, and have better cosmetic outcomes.[3] One of the major advantages is the much more wide access to lesion, irrespective of the location, unlike open thoracotomy. This holds true despite the fact that computed tomography scan gives us more or less reliable information regarding location of the lesion. The minimal risk of iatrogenic scoliosis, which is reported to be as high as 22% in a series after thoracotomy, is another major long-term advantage.[4]
Though VATS offers numerous advantages, but working space is a major constraint. Unlike adults, there is also difficulty in using double lumen endotracheal tubes in this subset of patients, and thus, single lung ventilation becomes a challenge. Even insufflation of carbon dioxide under positive pressure may lead to hemodynamic compromise. However, sometimes to achieve adequate working space a low-pressure insufflation (5 cm of water and flow at 0.5-1.0 L/min) may be used. We have successfully used this strategy in this case.
For VATS in children, 5 mm and 10 mm Hopkins rod-lens telescopes are used. The standard trocars used in laparoscopy (10, 5, and 3 mm) can be used. However, short trocars without valves are specifically designed for VATS. These instruments in addition to hand instrument can be inserted through an open incision, and they have a gentle “S” shaped curve to adapt to the shape of thoracic cage.
The foregut duplication cysts arise within the wall of esophagus and it is essential that esophageal integrity is maintained during excision. Although they can be enucleated easily, sometimes it is essential to perform partial resection of the duplication cyst with stripping of the remaining mucosa from the contiguous esophageal wall so that there is no esophageal perforation. The other differential diagnosis of the cystic lesions, bronchogenic cysts, often needs ablation of mucosa with diathermy, if it cannot be fully excised.[1] We have also left a part of duplication attached to wall of esophagus and cauterized the overlying mucosa. This could be performed more easily by thoracoscopy because of the magnification offered.
Although most of the children are asymptomatic, long-term follow-up is needed because of the chances of reflux esophagitis and pseudodiverticulum formation.[5] As the cyst arises in wall of esophagus, suture repair is essential after complete excision of cyst to prevent pseudodiverticulum formation. However, after partial excision in a small cyst, repair may not be needed.[6]
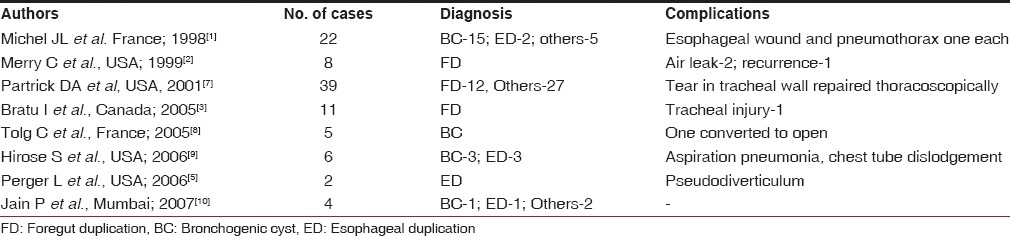
A table containing literature review of all published case series of pediatric thoracoscopic foregut cyst excision along with their major complications is shown in Table 1.
Table 1.
Major publications of pediatric thoracoscopic foregut duplication cyst excision
Newer modalities in terms of robotic surgery had also been reported in literature for excision of cysts. However, availability, cost, and experience are major constraints.
CONCLUSION
Thoracoscopy should be considered for treatment for cysts and duplications of the esophagus.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.[10]
REFERENCES
- 1.Michel JL, Revillon Y, Montupet P, Sauvat F, Sarnacki S, Sayegh N, et al. Thoracoscopic treatment of mediastinal cysts in children. J Pediatr Surg. 1998;33:1745–8. doi: 10.1016/s0022-3468(98)90276-7. [DOI] [PubMed] [Google Scholar]
- 2.Merry C, Spurbeck W, Lobe TE. Resection of foregut-derived duplications by minimal-access surgery. Pediatr Surg Int. 1999;15:224–6. doi: 10.1007/s003830050561. [DOI] [PubMed] [Google Scholar]
- 3.Bratu I, Laberge JM, Flageole H, Bouchard S. Foregut duplications: Is there an advantage to thoracoscopic resection? J Pediatr Surg. 2005;40:138–41. doi: 10.1016/j.jpedsurg.2004.09.025. [DOI] [PubMed] [Google Scholar]
- 4.Van Biezen FC, Bakx PA, De Villeneuve VH, Hop WC. Scoliosis in children after thoracotomy for aortic coarctation. J Bone Joint Surg Am. 1993;75:514–8. doi: 10.2106/00004623-199304000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Perger L, Azzie G, Watch L, Weinsheimer R. Two cases of thoracoscopic resection of esophageal duplication in children. J Laparoendosc Adv Surg Tech A. 2006;16:418–21. doi: 10.1089/lap.2006.16.418. [DOI] [PubMed] [Google Scholar]
- 6.Agarwal P, Bagdi R. Thoracoscopic removal of oesophageal duplication cyst. J Minim Access Surg. 2011;7:147–50. doi: 10.4103/0972-9941.78350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Partrick DA, Rothenberg SS. Thoracoscopic resection of mediastinal masses in infants and children: An evaluation of technique and results. J Pediatr Surg. 2001;36:1165–7. doi: 10.1053/jpsu.2001.25740. [DOI] [PubMed] [Google Scholar]
- 8.Tölg C, Abelin K, Laudenbach V, de Heaulme O, Dorgeret S, Lipsyc ES, et al. Open vs thorascopic surgical management of bronchogenic cysts. Surg Endosc. 2005;19:77–80. doi: 10.1007/s00464-003-9328-x. [DOI] [PubMed] [Google Scholar]
- 9.Hirose S, Clifton MS, Bratton B, Harrison MR, Farmer DL, Nobuhara KK, et al. Thoracoscopic resection of foregut duplication cysts. J Laparoendosc Adv Surg Tech A. 2006;16:526–9. doi: 10.1089/lap.2006.16.526. [DOI] [PubMed] [Google Scholar]
- 10.Jain P, Sanghvi B, Shah H, Parelkar SV, Borwankar SS. Thoracoscopic excision of mediastinal cysts in children. J Minim Access Surg. 2007;3:123–6. doi: 10.4103/0972-9941.38905. [DOI] [PMC free article] [PubMed] [Google Scholar]