

Abstract
Introduction:
Prevalence of diabetes and its complications have been a burden to the society from the ancient times, in the present and also will be in the future unless proper measures are taken to prevent its manifestation. There have been an increasing number of death associated-amputation cases which are mainly caused by nonhealing wounds. These facts urge researchers to develop new, more effective wound treatments for diabetic patients.
Aim:
To evaluate and compare the effect of Katupila Kalka (Securinega leucopyrus [Willd.] Muell. leaf paste) and Tila Taila (Sesamum indicum oil) in Madhumehajanya Vrana (diabetic wounds/ulcers) with Betadine ointment.
Materials and Methods:
A total of 23 patients of Madhumehajanya Vrana were chosen and randomly divided into two groups (Group A and B). Patients of Group A were treated with local application of Katupila Kalka with Tila Taila, whereas, in Group B, Betadine ointment was applied on the affected parts, once a day in the morning for 30 days. The relief in signs and symptoms were assessed on scoring pattern.
Results:
In Group A, diabetic wounds treated with Katupila paste got healed within 28 days with minimal scar formation without any complications, whereas in Group B, wound was healed completely only in two patients within 28 days. In both the groups, no patients reported any adverse drug reaction during the entire course of treatment as well as in follow-up period.
Conclusion:
Study concluded that the drug Katupila Kalka possesses Vrana Ropana (wound healing) activity with fine scaring.
Keywords: Betadine, diabetic foot ulcer, Katupila Kalka, Madhumehajanya Vrana, Ropana, Securinega leucopyrus, Tila Taila, wound healing
Introduction
In 2011, it was estimated that 366 million people worldwide had diabetes, representing roughly 8.3% of the adult population (20–79 years of age group). The number is expected to reach 552 million by 2030, representing 9.9% of the adult population. Diabetes is associated with various short and long-term complications, many of which, if left untreated, can be fatal. All these also have the potential to reduce the quality of life of people with diabetes and their families. The most common long-term complications affect the heart, eyes, kidneys, and feet.[1] Foot infections in persons with diabetes are a common and complex.[2,3] In addition to causing severe morbidities, they now account for the largest number of diabetes-related hospital bed-days[4] and are the most common proximate, nontraumatic cause of amputations.[5,6] Diabetic foot infections require careful attention and coordinated management, preferably by a multidisciplinary foot-care team.[7]
Ayurveda has its own principles, but it is incorporating new theories and drugs in it and is presenting them according to its principles. Number of drugs known to Ayurveda since Vedic era is increasing with the time. Acharya Charaka says that a physician can add new drugs to these Mahakashayas by his own intelligence that will help him to treat the patients.[8] He also states that one should get the knowledge about plants from tribal people or cowherds as they know and use the plants in a better way.[9] However, after Acharya Bhavamishra, the process of addition of new drugs to science has diminished or somewhat ceased. It is said that the wounds/ulcers of the diabetic patient are cured with difficulty.[10] Even with the latest technology and modern medicine in hand, highly trained medical team around, yet the majority of the diabetic ulcers end up with more or less amputation of the concerned major or minor part of the lower limb.
Securinega leucopyrus (Willd.) Muell. is known as Humari in India, Katupila in Sri Lanka and Spinous Fluggea in English. It is a desert climatic plant used topically in paste form for the healing of chronic and nonhealing wounds.
Hence, in the light of the above references from classics, Katupila Kalka (paste) was selected for this study with an aim to assess its effect in the management of Madhumehajanya Vrana (diabetic ulcer).
Materials and Methods
Diagnosed patients of diabetic wounds were selected from outpatient and inpatient departments of Shalya Tantra irrespective of the age, sex, religion, caste, occupation, etc. The study was started after obtaining approval from the Institutional Ethics Committee (PGT/7-A/2012-2013/1964 dated 21/09/2012) and study has been registered under Clinical Trial Registry of India (No.: CTRI/2013/09/004020). Informed written consent from each patient was obtained before starting treatment course.
Inclusion criteria
Diagnosed cases of Madhumehajanya Vrana with Type I and Type II diabetes mellitus of 18–70 years age of either sex.
Exclusion criteria
The patients with a history of tuberculosis, wounds other than diabetic wounds, uncontrolled hypertension, cardiac diseases, such as myocardial infarction, coronary artery disease, and ischemic heart disease were excluded in this study. Patients with human immune virus (HIV), venereal disease research laboratory (VDRL) and hepatitis-B test positive were also excluded from the study.
Laboratory investigations
Routine hematological parameters such as hemoglobin percentage, total leukocyte count, differential leucocyte count, bleeding time, clotting time, erythrocyte sedimentation rate; blood biochemical parameters such as fasting blood sugar, postprandial blood sugar, hepatitis B surface antigen, VDRL, and HIV; urine examination (routine and microscopic) was done to find out any other pathological condition.
Radiological examination
X-ray of the affected foot (dorsoventral and lateral view) was done to rule out the osteomylitis of bone.
Grouping and posology
Totally 23 patients of the diabetic wound were allocated randomly into two groups (Group A and B).
Group A (n = 13): In this group, Katupila Kalka (paste of S. leucopyrus leaves) with Tila Taila (sesame oil) was applied locally on the affected part. The dressing was done once in the morning up to 1 month or healing of wound which is earlier
Group B (n = 10): In this group, patients were treated with dressing of Betadine ointment once daily in the morning and treated as the standard control group.
The leaves of Katupila were obtained from Sri Lanka and authenticated[11] at Pharmacognosy Laboratory, IPGT and RA, Jamnagar.
Patients were advised to continue their anti-diabetic and anti-hypertensive medications (Allopathic/Ayurvedic) during treatment.
Assessment of therapy
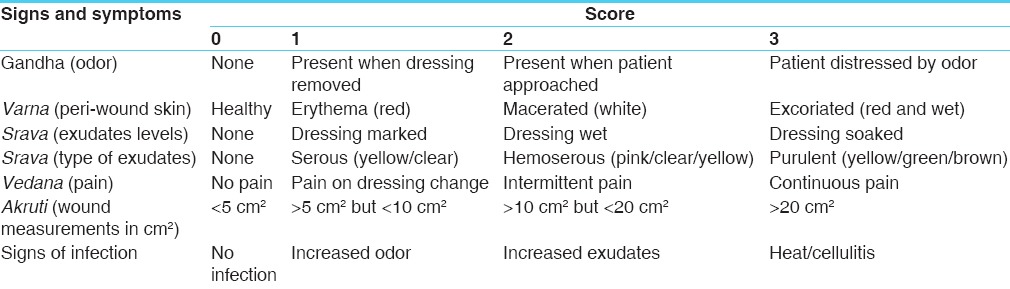
The assessment of results was carried out mainly on the basis of relief in the signs and symptoms of the ulcers that are odor (Gandha), peri-wound skin (Varna), exudates level (Srava), type of exudates, pain (Vedana), wound measurement in cm (Akruti), and signs of infection [Table 1].
Table 1.
Gradation for assessment of results
Effect of therapy was statistically analysed by using student ‘t’ test.
Overall effect of therapy
Cured: 100% improvement in subjective and objective parameters
Marked improvement: 70–99%
Moderate improvement: 50–69%
Mild improvement: 30–49%
Unchanged: <30%.
Observations
The demographic data reveal that maximum patients were from the age group of 46 to 65 years (57%). Male patients were more that is 78.3% may be due to their irregular eating habits, addiction, excess standing work, and less care. Maximum patients were following Hindu religion (78%) and married (87%). Socioeconomically middle-class patients were in the majority (78.2%). The 78.27% of patients were having a history of diabetes and 21.73% of patients found with a history of both diabetes and hypertension. The 69.5% of patients had family history of diabetes. For the management of diabetic wound, 39.1% of patients had received medical treatment in past and 52.1% of patients had undergone surgery, whereas 8.6% of patients had both medical and surgical treatment. The majority of the patients that is 56.5% were suffering from wounds since 1 to 6 months, 34.7% of patients noted traumatic onset and maximum 73.9% were found with single wound. The 82.6% of patients were having Puya Srava (purulent exudates) and 95.6% of patients had Ghana Srava with 43.4% were having moderate Srava (discharge). Maximum numbers of patients presented without pain whereas only 34.9% of patients were found with pain. Bad odor was noted in all wounds and fever was found in maximum 73.91% of patients. In maximum 47.81% of patients the location of wound was at foot, as this part of the body more often gets trauma.
Results
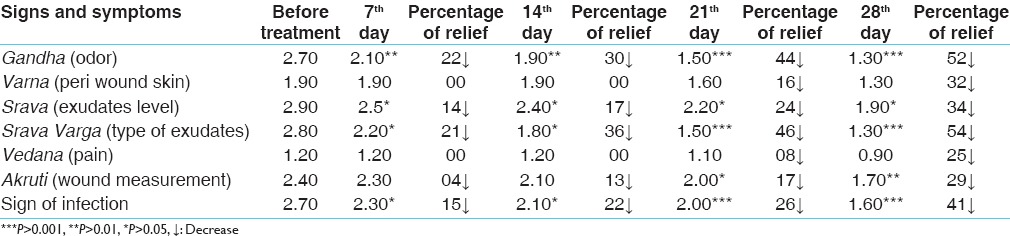
In this study, infection was controlled within 3–4 days and foul smell was controlled after 3 days in patients of Group A. In Group B, foul smell from ulcer continues until the wound was healed. The surrounded skin color became normal skin color within 7 days in maximum patients (76%) of Group A, whereas only 32% patients showed normal peri-wound skin color in Group B. In Group A, 55% of patients showed a complete cessation of discharge within 7 days whereas in Group B, exudation found reduced in 34% of patients at the end of 28th day. In all patients, pain sensation at wound site regained by 7th day in Group A, due to neo-vascularization and restored pain sensation in nerve fibers. In Group A, 12 patients wound size was reduced completely within 28 days, whereas in Group B, only 29% of patients wound size was reduced completely within 28 days. In Group A, signs of infections relieved 61% by the 7th day and totally relieved at the end of 28th day, whereas in Group B, patients infection was relieved 41% by the end of 28th day [Tables 2 and 3].
Table 2.
Effect of therapy on signs and symptoms of wound in Group A
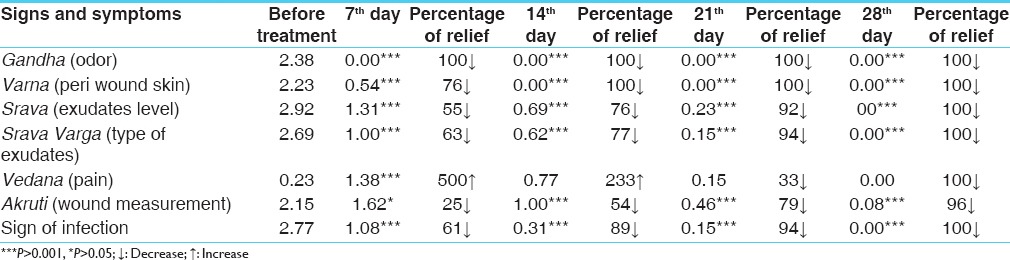
Table 3.
Effect of therapy on signs and symptoms of wound in Group B
In Group A, 92.3% of patients were completely cured, whereas in Group B, 20% of patients were completely cured [Figure 1]. Wound healing effect of Katupila in four cases is depicted in Figure 2.
Figure 1.
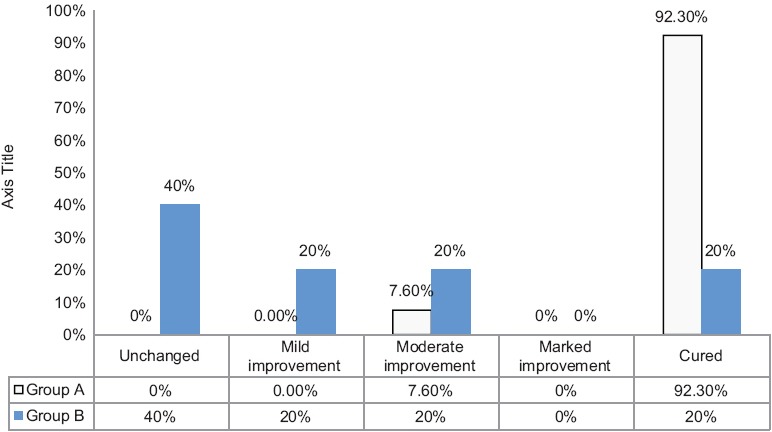
Overall effect of therapy
Figure 2.

Before and after treatment wound status of Katupila treated cases
Discussion
In this study, foul smell was controlled after 3 days in Group A patients, which was found statistically significant (P < 0.001). In Group B, foul smell from ulcer continues until the wound was healed. The Krimighna, Vishaghna, Rakshoghna (antimicrobial) properties of the Katupila helped to control the local infection and ultimately the bad odor.[12]
In Group A, 100% normal skin coloration was achieved which was found statistically significant (P < 0.001). In 32% of patients of Group B, peri-wound skin color became normal which was found statistically significant (P > 0.05). Katupila may have Rakta Shodhana, Pittashamana, Varnya, Twaka Prasadana properties which helped to improve the surrounding wound skin color.
Complete cessation of discharge within 7 days was observed in 55% of patients of Group A, while in remaining patients discharge was reduced by 28th day which was statistically significant (P < 0.001). Krimighna property of drug helped to control the infection. Hence, it can be said that Katupila paste had a better role than Betadine to reduce exudates level.
In Group A, 77% of patients presented without pain while the pain was reported in 23% of patients due to diabetic neuropathy. After treating with Katupila, pain sensation regained by 7th day due to neo-vascularization and restored pain sensation in nerve fibers. The statistically insignificant result in pain relief was seen due to the restoration of pain sensation by correcting neuropathy. The Snigdha Guna of Tila Taila helped in control the vitiation of Vata and helped to relief in pain.[13] In Group B, there was minimal neovascularization, but the pain was relieved in 25% of patients due to the healed wounds which were statistically significant (P > 0.05). Hence, it can be inferred that Katupila is better than Betadine ointment to regain pain sensation (initial stage) as well as to relieve pain (in later stage).
Complete wound healing was observed within 28 days in 92% cases so wound size reduction was found statistically highly significant (P < 0.001) which may be due to Katupila which may have Lekhana (scraping), Shodhana (cleaning) and Ropana (healing) properties. Madhura Rasa, Prinana (nourishment), Dhatuvardhana (tissue strength) and Dhatuposhana (nutrition) actions of Katupila helped to reduce the wound size by promoting healing and the rate of contraction. The infection at the wound site was assessed on the basis of odor, exudate level, local temperature, and swelling in both the groups. In Group A, signs of infections relieved 61% by the 7th day and totally relieved at the end of 28th day. Local application of Katupila reduces the discharge, swelling, pain by controlling the bacterial load, so wound became Shuddha (clean or healthy). Whereas in Group B, infection was relieved in 41% by the end of 28th day. Both drugs have shown statistically highly significant (P < 0.001) result in controlling infection. However, on the comparison, the duration of infection control by Katupila paste (that is 1st week) was found earlier than Betadine which took longer duration in controlling infections. The strength and positive finding of this study is Katupila Kalka had the potential to cure the diabetic wounds early than Betadine ointment. Findings in previously published case reports also showed the good potential in wound healing by Katupila.[14,15] None of the adverse drug reaction noted during the treatment period.
A reverse pharmacological study in the suitable animal model is a further scope of this work. As this drug is being used by traditional people and of herbal origin, there is a need to generate safety and toxicity profile of Katupila. The limitation of this research work is less number of patients due to the limited time of the postgraduate study.
Conclusion
The study concluded that Katupila Kalka (paste) possesses highly qualitative efficacy in “Vrana Ropana” with fine scaring. Therefore, it may be recommended that this low cost, easily preparable application may be prescribed for continuous use for the healing purposes.
Financial support and sponsorship
IPGT & RA, Gujarat Ayurved University, Jamnagar.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Belgium: International Working Group on the Diabetic Foot (IWGDF) and International Diabetes Federation Diabetic Foot Program (IDF DFP); [Last Accesssed on 2014 Apr 25]. Available from: http://www.iwgdf.org/ [Google Scholar]
- 2.Lipsky BA. International Consensus Group on Diagnosing and Treating the Infected Diabetic Foot. A report from the international consensus on diagnosing and treating the infected diabetic foot. Diabetes Metab Res Rev. 2004;20(Suppl 1):S68–77. doi: 10.1002/dmrr.453. [DOI] [PubMed] [Google Scholar]
- 3.Tennvall GR, Apelqvist J, Eneroth M. Costs of deep foot infections in patients with diabetes mellitus. Pharmacoeconomics. 2000;18:225–38. doi: 10.2165/00019053-200018030-00003. [DOI] [PubMed] [Google Scholar]
- 4.Reiber GE. The epidemiology of diabetic foot problems. Diabet Med. 1996;13(Suppl 1):S6–11. [PubMed] [Google Scholar]
- 5.Reiber GE, Vileikyte L, Boyko EJ, del Aguila M, Smith DG, Lavery LA, et al. Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care. 1999;22:157–62. doi: 10.2337/diacare.22.1.157. [DOI] [PubMed] [Google Scholar]
- 6.Pecoraro RE, Reiber GE, Burgess EM. Pathways to diabetic limb amputation. Basis for prevention. Diabetes Care. 1990;13:513–21. doi: 10.2337/diacare.13.5.513. [DOI] [PubMed] [Google Scholar]
- 7.Crane M, Werber B. Critical pathway approach to diabetic pedal infections in a multidisciplinary setting. J Foot Ankle Surg. 1999;38:30–3. doi: 10.1016/s1067-2516(99)80085-4. [DOI] [PubMed] [Google Scholar]
- 8.Sharma RK, Dash B, editors. Charaka Samhita of Agnivesha, Sutrasthana. Reprint Edition. Ch 4, Ver 20. Varanasi: Chaukhambha Sanskrita Series; 2009. p. 101. [Google Scholar]
- 9.Sharma RK, Dash B, editors. Charaka Samhita of Agnivesha, Sutrasthana. Reprint Edition. Ch 1, Ver 128-129. Varanasi: Chaukhambha Sanskrita Series; 2009. p. 60. [Google Scholar]
- 10.Singhal GD, editor. Sushruta Samhita of Susruta, Sutrasthana. 2nd ed. Ch 23, Ver 7. Delhi: Chaukhamba Sanskrit Pratishthan; 2007. p. 209. [Google Scholar]
- 11.Ajmeer AS, Harisha CR, Dudhamal TS, Gupta SK. Micromorphological and micrometric evaluation of Securinega leucopyrus (willd.) Muell. Leaf and stem-unexplored drug. Int J Sci Invent Today. 2013;2:140–9. [Google Scholar]
- 12.Bakshu LM, Jeevan RA, Venkata RR. Antimicrobial activity of Securinega leucopyrus by environmental sciences. Fitoterapia. 2001;72:930–3. doi: 10.1016/s0367-326x(01)00341-0. [DOI] [PubMed] [Google Scholar]
- 13.Acharya YT, editor. Susrutha Samhitha of Sushruta, Sutra Sthana. 12th ed. Ch 45, Ver 112. Varanasi: Chaukhambha Sanskrita Sansthan; 2001. p. 178. [Google Scholar]
- 14.Ajmeer AS, Dudhamal TS, Gupta SK, Mahanta V. Katupila (Securinega leucopyrus) as a potential option for diabetic wound management. J Ayurveda Integr Med. 2014;5:60–3. doi: 10.4103/0975-9476.128872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ajmeer AS, Dudhamal TS, Gupta SK, Mahanta V. Topical application of Katupila (Securinega leucopyrus) in Dushta Vrana (chronic wound) showing excellent healing effect: A case study. Ayu. 2014;35:175–8. doi: 10.4103/0974-8520.146238. [DOI] [PMC free article] [PubMed] [Google Scholar]