

Abstract
We present the case of a rupture of the brachialis muscle in a 17-year-old male. We provide an overview of the current literature discussing previously reported cases, the clinical features, and recommended treatment. The anatomy and function of the brachialis muscle and possible mechanism of injury are also discussed.
Abbreviations: MRI, magnetic resonance imaging
Introduction
Injury to the brachialis muscle is a rare injury [1, 2]. To our knowledge, there have been only 3 cases reported in the literature. We report an isolated brachialis muscle tear in a young male who underwent a hyperextension injury to his right elbow. Magnetic resonance imaging (MRI) demonstrated a closed partial rupture of his brachialis muscle with an intramuscular hematoma
Case Report
A 17-year-old male was brought by ambulance to the emergency room with acute right elbow pain. The patient, a high school football player, was tackled and underwent hyperextension of his right elbow. He felt immediate pain and swelling, however did not note any popping sensation. The physical examination was limited due to pain and swelling in the anterior brachial portion of the arm, however no neurovascular abnormalities were present. Radiographs were taken which showed no fracture, dislocation, or elbow joint effusion. It was felt at the time that the patient had either a tear of the biceps brachii muscle, transient dislocation, or ligamentous injury. He was immobilized with a posterior splint, and instructed to undergo MRI four days later.
MRI of the right elbow demonstrated a large mass, with signal characteristics of a hematoma, measuring 31.2 mm in greatest diameter within the brachialis muscle (Fig. 1). There was significant edema within the surrounding muscle (Figure 1, Figure 2). The brachialis tendon insertion at the ulna was normal. The biceps brachii muscle and tendon, surrounding ligaments, and osseous structures were normal. Because of the initial suspicion of biceps tendon tear, MRI was centered on the distal biceps tendon and excluded the proximal portion of the intramuscular hematoma. A repeat MRI to include the full proximal extent of the hematoma was obtained 19 days after initial imaging, in order to exclude an underlying lesion. This showed interval decrease in size of the hematoma to 18.0 mm, with no evidence of underlying lesion (Fig. 3).
Figure 1.

17-year-old male with brachialis muscle rupture. (A) Coronal T1-weighted MRI of the elbow in flexion. The distal aspect of a mass shows intermediate signal with high signal rim consistent with an acute hematoma (H) within the substance of the brachialis muscle (Br). Brt: Brachialis tendon, Bt: Biceps tendon, Ra: Radius. (B) Sagittal T1-weighted MRI of the elbow shows similar findings. (C) Corresponding sagittal STIR-weighted MRI shows high signal within the muscle fibers of the brachialis muscle, consistent with hemorrhage, and intermediate to high signal mass with surrounding rim of low signal consistent with hematoma (H).
Figure 2.
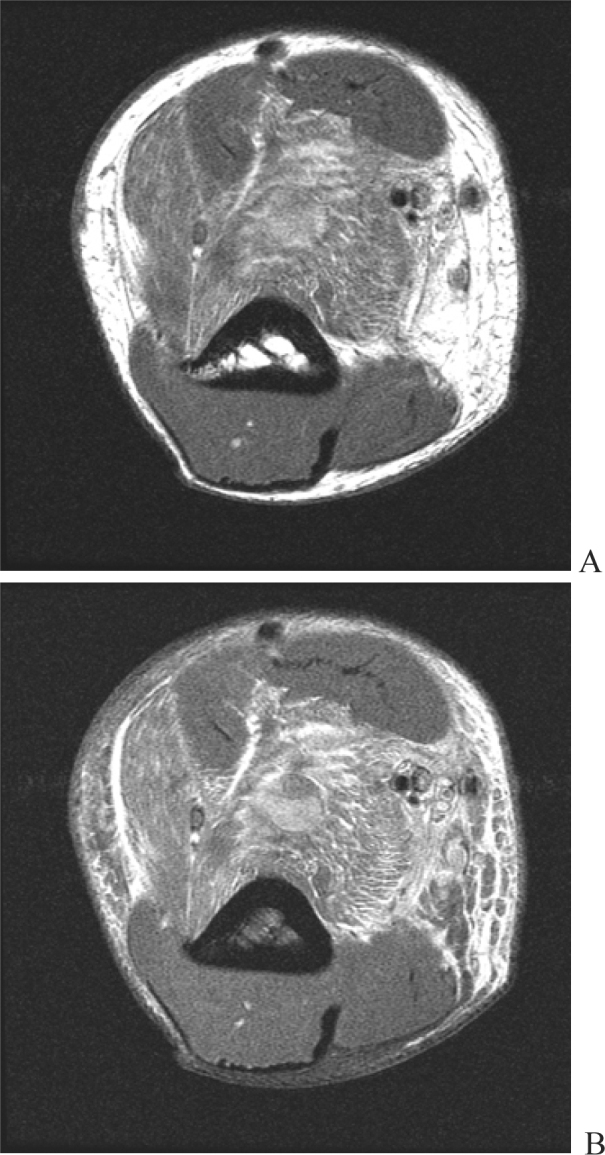
17-year-old male with brachialis muscle rupture. (A) Intermediate-weighted axial MRI through the upper arm showing hemorrhage within the deep portion (D) of the brachialis muscle (presumed deep head) with sparing of the superficial head (S). Margins of the brachialis muscle are outlined in black. (B) Mixed signal-intensity hematoma within the substance of the brachialis muscle (white arrow). Note mild strain in the brachioradialis muscle (black arrow).
Figure 3.

17-year-old male with brachialis muscle rupture. MR images obtained 19 days after injury. (A) Axial T1-weighted MRI now shows larger peripheral area of high signal consistent with evolving hematoma. (B) Sagittal T1-weighted and (C) sagittal STIR-weighted MRI show consolidation and decrease in size of hematoma, with resolution of muscle edema.
Discussion
Injury to the brachialis muscle is a rare occurrence and is not well documented [1, 2]. Injury to the brachialis tendon is also very rare, and to our knowledge, has not been reported. On the other hand, injuries to the biceps brachii tendon are more common. A limited number of injuries to the biceps brachii muscle have also been reported [3], most notably in paratroopers [4], but also from other mechanisms of injury [3, 4, 5, 6].
There have been conflicting opinions regarding the basic morphology of the brachialis muscle in the major textbooks and literature [7, 8]. Gray’s Anatomy describes a normal variant being composed of two or more parts [7]. Most recently, Leonello et al demonstrated the consistent presence of two heads of the brachialis, a superficial and a deep head [8]. Figure 2a demonstrates a hematoma that has consolidated within what appears to be the deep head of the brachialis muscle while the superficial head remains intact.
Leonello et al proposed that the dual morphology of the muscle has dual functions [8]. Because of the insertion of the deep head proximally onto the coronoid process, it has a mechanical advantage because when the arm is fully extended, it is anterior to the axis of rotation and helps to initiate elbow flexion. The tendon of the superficial head of the brachialis muscle inserts distal to the deep head, along the coronoid process, providing its greatest mechanical advantage when the arm is at 90 degrees flexion and thus stabilizing an already flexed arm [8]. The brachialis muscle is also responsible for maintaining the stability of the elbow throughout concentric and eccentric contraction [9].
Kulig et al showed that the brachialis muscle is preferentially recruited over the biceps brachii when undergoing eccentric contraction [9]. In the cases reported by Nishida et al, it was precisely this motion that these particular athletes underwent. They proposed that eccentric contraction, during pronation of the forearm was responsible for the injuries to the brachialis muscle in their patients [2]. We are not certain of the mechanism of injury in our patient, however, if any resistance of hyperextension was involved, this would be consistent with the proposed mechanism [2].
Our review of the literature revealed a total of 3 traumatic injuries of the brachialis muscle reported since the 1950’s. The first report of a brachialis muscle rupture was by Van Den Berghe et al in 2001. They reported a case of a sixty seven year old male who had been lifting heavy objects the day before initial presentation. A tear of the biceps brachii muscle was the initial suspicion, however MRI revealed a tear in the distal aspect of brachialis near the musculotendinous junction. He was followed up by serial clinical examinations, an MRI in six weeks and was essentially healed in 10 months [1].
Nishida et al reported 2 cases of brachialis muscle tears, both within the muscle belly. Both were athletically active males, aged sixteen and sixty-seven, and attributed their injuries to specific physical activity. The sixteen year old was a Judo athlete that presented 7 days after pain and swelling in the left arm. The sixty-seven year old presented 7 days after noticing pain while practicing his golf swing. Due to the sub-acute presentation, of both patients, a neoplasm was originally suspected. After evaluation by MRI, both patients were diagnosed with partial tears of the brachialis muscle. Both patients were treated conservatively with range of motion exercises and returned to normal activity in 3 months [2].
An additional case of a brachialis hematoma was discovered during our literature review of muscle injury. A single MR image of a brachialis hematoma was published [10], which was quite similar to our case. However, details pertaining to this case were not provided.
Aside from traumatic injuries to the brachialis muscle, some unusual reports include a tuberculous abscess of brachialis and biceps [11], brachialis necrosis secondary to exercise [12], and atraumatic snapping of brachialis tendon [13, 14].
The clinical features of a brachialis muscle injury are pain and swelling in the anterior mid arm [1, 2]. Unlike a biceps muscle injury, in which a palpable gap may be felt on physical examination [3], injury to the brachialis muscle would be difficult to palpate due to its position deep to the overlying biceps brachii. As always, plain films should be taken to verify that other more common causes can be ruled out. Additional imaging should depend on the history and physical examination. If the patient’s pain is out of proportion, or simply, a confirmation of an injury to musculoskeletal structures is desired, then further imaging can be used to evaluate for soft tissue injury.
All three cases of traumatic brachialis muscle injuries reported were treated non-operatively and responded well to conservative treatment [1, 2]. It was proposed by Nishida et al, that conservative treatment could be used for brachialis muscle injuries because it was successful in their cases in addition to the case reported by Van der Burghe et al. Conservative treatment also proved to be successful in our reported case.
In conclusion, tear of the brachialis muscle, although rare, should be considered in the differential for elbow pain after injury. The presentation may mimic other injuries such as biceps tendon tears. MRI is helpful in evaluating this injury and monitoring its resolution.
Footnotes
Published: December 10, 2008
Contributor Information
James Bret Winblad, Email: jwinblad@kumc.edu.
Eva Escobedo, Email: eva.escobedo@ucdmc.ucdavis.edu.
John C. Hunter, Email: john.hunter@ucdmc.ucdavis.edu.
References
- 1.Van den Berghe GR, Queenan JF, Murphy DA. Isolated rupture of the brachialis: a case report. J Bone Joint Surg Am. 2001 Jul;83-A(7):1074–1075. doi: 10.2106/00004623-200107000-00015. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Nishida Y, Tsukushi S, Yamada Y, Hosono K, Ishiguro N. Brachialis muscle tear mimicking an intramuscular tumor: a report of two cases. J Hand Surg [Am] 2007 Oct;32(8):1237–1241. doi: 10.1016/j.jhsa.2007.06.002. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Chen HW, Chew FS. Complete rupture of both heads of the biceps brachii muscle belly by blunt trauma. Radiology Case Reports. [Online] 2006;4:145–148. doi: 10.2484/rcr.v1i4.28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Heckman JD, Levine MI. Traumatic closed transaction of the biceps brachii in the military parachutist. J Bone Joint Surg Am. 1978 Apr;60(3):369–372. [PubMed] [PubMed] [Google Scholar]
- 5.Carmichael KD, Foster L, Kearney JP. Biceps muscle rupture in a water skier. Orthopedics. 2005 Jan;28(1):35–37. doi: 10.3928/0147-7447-20050101-11. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Safran MR, Graham SM. Distal biceps tendon ruptures: incidence, demographics, and the effect of smoking. Clin Orthop Relat Res. 2002 Nov;(404):275–283. [PubMed] [PubMed] [Google Scholar]
- 7.Gray H, Clemente CD. Gray's Anatomy. 29th Edition. Lea & Febiger; Philadelphia, PA: 1985. p. 528. [Google Scholar]
- 8.Leonello DT, Galley IJ, Bain GI. Brachialis muscle anatomy. A study in cadavers. J Bone Joint Surg Am. 2007 Jun;89(6):1293–1297. doi: 10.2106/JBJS.F.00343. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.Kulig K, Powers CM, Shellock FG, Terk M. The effects of eccentric velocity on activation of elbow flexors: evaluation by magnetic resonance imaging. Med Sci Sports Exerc. 2001 Feb;33(2):196–200. doi: 10.1097/00005768-200102000-00004. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Elsayes KM, Lammle M, Shariff A, Totty WG, Habib IF, Rubin DA. Value of magnetic resonance imaging in muscle trauma. Curr Probl Diagn Radiol. 2006 Sep-Oct;35(5):206–212. doi: 10.1067/j.cpradiol.2006.06.003. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Abdelwahah IF, Kenan S. Tuberculous abscess of the brachialis and biceps brachii muscles without osseous involvement. A case report. J Bone Joint Surg Am. 1998;80(1):1521–1524. doi: 10.2106/00004623-199810000-00014. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Farmer KW, McFarland EG, Sonin A. Isolated necrosis of the brachialis muscle due to exercise. Orthopedics. 2002;25(6):196–203. doi: 10.3928/0147-7447-20020601-20. [PubMed] [DOI] [PubMed] [Google Scholar]
- 13.Coonrad RW, Spinner RJ. Snapping brachialis tendon associated with median neuropathy: a case report. J Bone Joint Surg Am. 1995;77(12):1891–1893. doi: 10.2106/00004623-199512000-00015. [PubMed] [DOI] [PubMed] [Google Scholar]
- 14.Rudy BS, Armstrong AD. Atraumatic snapping brachialis in a 37-year-old woman. JAAPA. 2007 Jan;20(1):48. doi: 10.1097/01720610-200701000-00010. [PubMed] 50-1. [DOI] [PubMed] [Google Scholar]