

Abstract
Background & Aims
It is not clear how intake of gluten during infancy affects subsequent risk of celiac disease. We investigated whether gluten intake before 2 years of age increases risk for celiac disease in genetically susceptible children.
Methods
We performed a case–control study of 436 pairs of children, generated from a database of 2525 children with genetic susceptibility to celiac disease in Sweden, matched for sex, birth year, and HLA genotype from September 2004 and February 2010. Children were screened annually for celiac disease using an assay for tissue transglutaminase autoantibodies (tTGA). Intestinal biopsies were collected from children who tested positive for tTGA to confirm the presence of celiac disease. Gluten intake was calculated from 3-day food records collected when the children were 9, 12, 18 and 24 months old.
Results
Breastfeeding duration (median 32 weeks) and age at first introduction to gluten (median 22 weeks) did not differ between cases and tTGA-negative children (controls). At the visit prior to tTGA seroconversion, cases reported a larger intake of gluten (median 4.9 g/day) than controls (median 3.9 g/day) (odds ratio [OR], 1.28; 95% confidence interval [CI], 1.13–1.46; P=.0002). More cases consumed amounts of gluten in the upper 3rd tertile (i.e. >5.0 g/day) before they tested positive for tTGA seroconversion than controls (OR, 2.65; 95% CI, 1.70–4.13; P<.0001). This increase in risk was similar for children homozygous for DR3-DQ2 (OR, 3.19; 95% CI, 1.61–6.30; P=.001), heterozygous for DR3-DQ2 (OR, 2.24; 95% CI, 1.08≥4.62; P=.030), and for children not carrying DR3-DQ2 (OR, 2.43; 95% CI, 0.90–6.54; P=.079).
Conclusions
Intake of gluten before 2 years of age increases risk of celiac disease at least 2-fold in children with genetic risk factors for this disease. This association did not differ among HLA-DR3-DQ2 haplotypes. These findings may be taken into account for future infant feeding recommendations.
Keywords: pediatric, TEDDY study, diet, wheat
Introduction
Celiac disease (CD) is an emerging public health disorder affecting 1–3% of the general population with variations between ethnic groups and geographic regions.1 Both gluten exposure and carrying any of the HLA-risk haplotypes DR3-DQ2 and DR4-DQ8 are necessities for the risk of CD.2,3 However, gluten is a universally consumed food antigen and half of the Caucasian population possesses at least one of these two risk haplotypes4, suggesting that additional environmental factors determine whether lifelong gluten intolerance develops in an individual at genetic risk.
The role of time to first introduction to gluten in the risk of CD has long been debated. Retrospective data generated in Sweden indicated that introducing gluten in small amounts between 4 and 6 months of age while being breastfed reduces the risk of celiac disease compared with introducing gluten in larger amounts at older ages.5,6 The hypothesis of an optimal time window for inducing tolerance to gluten was recently questioned by results of prospective cohort studies.7–8 Furthermore, two recent randomized controlled intervention studies failed to show an effect of timing of gluten introduction on risk of CD, and neither directly examined the impact of quantity of gluten intake.9, 10 Although retrospective data from Sweden pointed to the importance of quantity of gluten intake for risk of CD11, no prospective studies free of recall bias have been performed so far.
The Environmental Determinants of Diabetes in the Young (TEDDY) study is an international prospective birth cohort study following genetically susceptible children in search of environmental factors associated with type 1 diabetes and CD.12 TEDDY has previously confirmed that the risk for celiac disease by five years of age is dependent on HLA genotype, and that children with the highest risk group (i.e. homozygous for DR3/DQ2) develop CD associated autoantibodies to tissue transglutaminase (tTGA) much earlier compared to children carrying a single or no DR3-DQ2 haplotype.13 Additionally, Swedish TEDDY participants are at the highest risk for CD at an early age compared to participants in other TEDDY countries.13 Swedish infants traditionally receive gluten-containing follow-up formulas and porridge during the first two years of life.14 Although Swedish TEDDY participants are introduced to gluten earlier than children in the other countries, the age at which gluten was introduced did not explain why Swedish children were at increased risk for CD in TEDDY.8 In this study, we investigated if the amount of gluten intake during the first two years of life is a risk factor for CD.
Subjects and Methods
Study population
The TEDDY study is conducted in six clinical centres in Finland, Germany, Sweden and the US, approved by local Institutional Review Boards and monitored by an External Advisory Board formed by the National Institutes of Health.15 Between September 2004 and February 2010, a total of 424,788 newborns were HLA genotyped at one of these six sites and were eligible if they had one of the following HLA-genotypes: DR3-DQ2/DR4-DQ8, DR4-DQ8/DR4-DQ8, DR4-DQ8/DR8, DR3-DQ2/DR3-DQ2, DR4-DQ8/DR4b, DR4-DQ8/DR1, DR4-DQ8/DR13, DR4-DQ8/DR9, and DR3-DQ2/DR9.16 Of the screened newborns, 48,140 were from the Swedish site of whom 3,723 (7.7%) were HLA-eligible and invited to a 15-year follow-up. Written informed consents were obtained from parents or primary caretakers in 2,525 of the 3,723 (68%).16
Annual screening for CD starts from the age of two years with tTGA using radiobinding assays as described elsewhere.17 Earlier blood samples collected from birth and onward were analyzed retrospectively to determine the age of seroconversion in cases with tTGA positivity.13 Children who tested positive for tTGA in two consecutive samples were defined as persistently tTGA positive and referred to their healthcare provider for evaluation of CD with intestinal biopsy. A biopsy showing Marsh score ≥2 in tTGA positive children proved CD.13 At time of this study, 2,062 of the Swedish children had been screened for tTGA of whom 330 were persistently tTGA positive and 147 were diagnosed with CD (Supplementary Figure 1).
Study design
A 1-to-3 matched nested case–control study was conducted on Swedish children screened for tTGA. Cases were defined as children with biopsy-confirmed CD. Given that the minimum time between planned study visits was 3 months, it was decided that controls for a case must be negative for tTGA within 45 days of the case’s age at seroconversion of tTGA and free of biopsy-confirmed CD within 45 days of the case’s age at biopsy. Age at seroconversion of tTGA was set as age when the first positive sample was drawn. Sex and HLA genotype (i.e. the number of DR3-DQ2 alleles) were chosen as matching factors.13 Controls were also matched to the cases on birth year, in order to control for changes in nutrient and food composition in commercial baby foods available on the Swedish market during follow-up. Three controls per case were randomly selected from subjects who met these matching criteria. Among the 147 children that were diagnosed with CD, one child did not have any eligible controls and another child had only one eligible control. In all, the analysis included 436 case–control pairs from 146 cases. Six cases (4%) and 13 (3%) controls had a first degree relative with CD. The median age of seroconversion to tTGA was 24 months (range 10–86 months), median age at diagnosis was 38 months (range 15–102 months).
Dietary assessment
Information about breastfeeding duration (exclusive and total breastfeeding) and timing of introduction of gluten-containing cereals were collected every 3 months through a booklet given to the parents at study entry, which has been described in detail elsewhere.8 Data on overall food consumption were collected by a 24-hour recall at the first clinic visit (age 3–4.5 months) and by 3-day food records at clinic visits at 6, 9, 12, 18 and 24 months of age.18 Parents were asked to keep a food record covering all foods and drinks consumed by the child for the given 3 days (ideally, 2 weekdays and 1 weekend day) prior to the scheduled visit. Parents were given instructions on how to fill out the records by trained study personnel. They were advised not to change the eating habits of the child during the time they were completing the food record. Written instructions and guidance where provided to the families. If the primary caregiver indicated that the child had started attending day-care, separate food records were provided for the day-care personnel to complete. At each clinical visit, the food records were reviewed by a study nurse. Probing about missing or unclear information was obtained by face-to-face interview during the visit. Brand names were requested for all commercial baby foods. Portion sizes were estimated using household measures, drawings and pictures from a booklet. Each set of photos of foods and dishes contained four to five portion sizes in increasing order. Drawings and shapes of other types of foods such as bread, cakes, and pizza were also included. For soft bread, drawings of real form bread slices and thicknesses where provided. The booklet was handed out to the families at study entry and used at home when keeping the food records.
Gluten-containing foods included products and composite dishes (such as pizza, sandwiches) with wheat, rye and barley, but not oats. Oats consists of proteins that will not lead to the same intestinal damage as wheat, rye and barley and were therefore treated as a non-gluten containing cereal.19 The food database and connected software enables the summarization of intake of each food and food group.20 Recipes are created to describe ingredients in dishes. For commercial baby foods containing gluten, specific recipes were created for each brand name based on the ingredient list. The Swedish National Food Composition Database was used as source for nutrient content and standard recipes of foods such as bread, sweet bakery, pancakes, and pizza, etc.21 Unique user recipes provided by the parents were added and used in the local database. All recipes were broken down to ingredients and intakes of gluten-containing flours were summarized and mean intake of the 3-day recording period was calculated as gram per day. Daily gluten intake was calculated from the amount of vegetable protein in gluten-containing flours and then multiplied by factor 0.8.22 At the age of 6 months, 97% of the children’s families had submitted complete food records, while 84% of the food records were submitted at the age of 24-months.
Statistical analyses
The Kruskal-Wallis test was used to compare the age of tTGA seroconversion in the cases by sex, birth year and HLA. Conditional logistic regression was used to compare characteristics in cases with those in matched controls. Gluten intake was estimated from the 3-day food records at the visit prior to when the cases seroconverted to tTGA. The estimate at the visit prior to the tTGA seroconversion was analyzed, as well as total intake, which was defined as the sum of the estimates from all visits up to the visit prior to the tTGA seroconversion. For cases whose age of seroconversion was older than 24 months, the visit at 24 months of age was used as the visit prior to seroconversion. The estimated amount of gluten intake at the visit prior to the tTGA seroconversion was analyzed both as a continuous variable (g/day) and as a trichotomous variable based on tertiles of quantity [i.e., low (<3.4 g/day), medium (3.4–5.0 g/day), and high (>5.0 g/day)]. The Kaplan-Meier estimates of time to tTGA seroconversion for cases, stratified by tertile of amount of gluten intake, were plotted. For controls currently negative for tTGA, censored time was the age at collection of the last sample negative for tTGA. For controls currently positive for tTGA, censored time was the age at collection of the initial sample positive for tTGA. All statistical analyses were performed using SAS, Version 9.4 (SAS Institute Inc. Cary, NC, USA). All reported p-values are two-sided without multiple testing correction and p-value<0.05 were considered to represent statistical significance.
Results
Age at first introduction to gluten, breastfeeding duration or having a first-degree relative with CD were considered as potential confounders, but none of the variables had an impact on the results and therefore not included in the final analysis. Matching factors and age of seroconversion are described in Table 1.
Table 1.
Matching factors and age of tTGA seroconversion in the TEDDY Swedish birth cohort and in children with celiac disease.
| Birth cohort | Celiac disease | Age of tTGA seroconversion | ||
|---|---|---|---|---|
|
| ||||
| Matching factor | N=2062 | N=146 | Median months (Q1, Q3) | p-valuec |
| Sex: | N (%) | N (%) | ||
| -Boys | 1055 (51) | 49 (34) | 29 (21,48) | 0.066 |
| -Girls | 1007 (49) | 97 (66) | 24 (18,36) | |
| Birth year: | ||||
| -2004 | 91 (4) | 8 (6) | ||
| -2005 | 366 (18) | 37 (25) | 28 (18,48) | 0.066* |
| -2006 | 377 (18) | 22 (15) | 30 (21,59) | |
| -2007 | 412 (20) | 31 (21) | 24 (20,37) | |
| -2008 | 363 (18) | 25 (17) | 30 (22,36) | |
| -2009 | 385 (19) | 19 (13) | 21 (17,24) | |
| -2010 | 68 (3) | 4 (3) | ||
| HLA-genotype: | ||||
| -DR3-DQ2/DR3-DQ2 | 438 (21) | 70 (48) | 21.5 (17,28) | <.0001 |
| -DR3-DQ2/DR4-DQ8 | 868 (42) | 48 (33) | 36 (22.5,48.5)a | |
| -DR3-DQ2/DR9 | 1(<1) | |||
| -DR4-DQ8/DR4-DQ8 | 455 (22) | 26 (18) | 35 (21.5,37)b | |
| -DR4-DQ8/DR8 | 268 (13) | 2 (1) | ||
| -DR4-DQ8/DR1 | 18 (1) | |||
| -DR4-DQ8/DR13 | 13 (<1) | |||
| -DR4-DQ8/DR9 | 1 (<1) | |||
2004 and 2010 were not included due to small number of observations
Including DR3-DQ2/DR4-DQ8 and DR3-DQ2/DR9
Including DR4-DQ8/DR4-DQ8, DR4-DQ8/DR8, DR4-DQ8/DR1, DR4-DQ8/DR13 and DR4-DQ8/DR9
Kruskal-Wallis test p-value
Gluten intake in cases and controls
Total and exclusive breastfeeding duration and age at first introduction to gluten-containing cereals (wheat, rye or barley) did not differ between cases and controls (Table 2). Cases reported higher gluten intake than the matched controls (Table 3). If cases and controls with a first degree relative with CD were excluded, the results were in the same direction (data not shown).
Table 2.
Infant feeding characteristics in children with celiac disease and matched controls.
| Celiac disease N=146 |
Controls N=436 |
|||
|---|---|---|---|---|
|
| ||||
| Characteristic | Median (Q1, Q3) | Median (Q1, Q3) | OR (95% CI) | p-value |
| Breastfeeding duration (weeks): | ||||
| -Total | 31 (20, 40) | 33 (18, 43) | 0.99 (0.99, 1.00) | 0.361 |
| -Exclusive | 4 (1, 14) | 6 (1, 16) | 0.98 (0.96, 1.00) | 0.124 |
| Age at 1st introduction(weeks): | ||||
| -gluten-containing cereals* | 22 (18, 24) | 22 (18, 24) | 0.99 (0.95, 1.04) | 0.866 |
| -wheat | 22 (20, 25) | 22 (18, 25) | 1.00 (0.96, 1.05) | 0.888 |
| Energy intake (kcal)≠ | 1019 (840, 1164) | 1009 (858, 1156) | 1.00 (1.00, 1.00) | 0.450 |
Gluten-containing cereals (wheat, rye or barley)
Total energy intake (kcal) at the visit prior to the cases 1st positive tTGA test
Table 3.
Daily gluten intake in children with celiac disease and matched controls.
| Celiac disease N=146 |
Controls N=436 |
|||
|---|---|---|---|---|
|
| ||||
| Gluten intake | Median (Q1, Q3) | Median (Q1, Q3) | OR (95% CI) | p-value |
| Total gluten (g) intake prior to tTGA seroconversion* | 10.5 (7.6,14.2) | 9.9 (5.9,13.8) | 1.05 (1.01, 1.10) | 0.030 |
| Gluten (g) intake at the visit prior to tTGA seroconversion | 4.9 (3.5,5.9) | 3.9 (2.9,5.2) | 1.28 (1.13, 1.46) | 0.0002 |
Intake from all visits (sum of all visits) up to the visit prior to the cases 1st positive tTGA test
One unit (g per day) increase of gluten prior to seroconversion of tTGA was associated with a 28% increase in risk of CD (p=0.0002). As 14 cases were missing gluten intake data at the visit prior to seroconversion (2 cases at the 18 month visit and 12 cases at the 24 month visit), 385 pairs from 132 cases were analyzed for the gluten intake prior to seroconversion of tTGA (Table 4). Gluten intake reported by cases was higher at all ages beginning at 12 months, continuing with a trend towards higher intake at 18 months, and again significantly higher intake was seen at the age of 24 months. Moreover, children who received amounts of gluten in upper tertile (i.e. high gluten intake) were at more than 2-fold higher risk for CD than those consumed less (OR=2.65; 95% CI=1.70–4.13; p <.0001). Figure 1 shows the Kaplan-Meier plot by three groups categorized by tertiles (low, medium, high intake).
Table 4.
Daily gluten intake at the clinical visit prior to tTGA seroconversion in children with celiac disease and matched controls.
| Celiac disease N=132* |
Controls N=385 |
|||||
|---|---|---|---|---|---|---|
|
| ||||||
| Age at 3-day food record | N* | Median (g/day)a (Q1,Q3) | N | Median (g/day)a (Q1,Q3) | OR (95% CI) | p-value |
| 9 months | 6 | 1.6 (1.4, 1.8) | 17 | 1.9 (1.1, 2.4) | 0.63 (0.19, 2.05) | 0.444 |
| 12 months | 32 | 4.9 (3.5, 5.6) | 89 | 3.2 (2.5, 4.5) | 1.58 (1.17, 2.13) | 0.003 |
| 18 months | 37 | 4.9 (3.9, 5.9) | 103 | 3.9 (3.2, 5.2) | 1.22 (0.99, 1.51) | 0.077 |
| 24 months | 57 | 5.1 (3.7, 6.2) | 176 | 4.3 (3.3, 5.7) | 1.23 (1.01, 1.49) | 0.043 |
Children with data missing at the clinic visit prior to tTGA seroconversion were excluded (N=14)
Reported gluten intake prior to age of tTGA seroconversion in children
Figure 1.
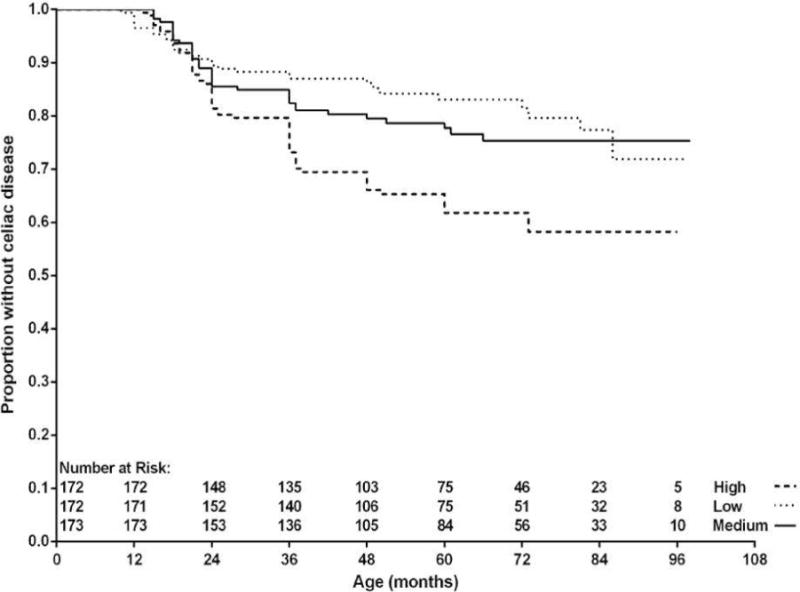
Time to tissue transglutaminase autoantibody (tTGA) positivity by gluten intake (g) at the visit closest prior to tTGA seroconversion. Gluten intake were categorized by tertiles of quantity [i.e., low (<3.4 g/day), medium (3.4–5.0 g/day), and high (>5.0 g/day)].
Gluten intake in cases according to HLA-genotype
Gluten intake at the visit prior to seroconversion of tTGA was not different among cases homozygous for DR3-DQ2 (median 4.8 g; Q1=3.2, Q3=5.9), heterozygous for DR3-DQ2 (median 5.1 g; Q1=3.8, Q4=6.3) or in those without DR3-DQ2 (median 4.9 g; Q1=3.5, Q3=5.9) (p=0.49). In order to examine whether the association between increased gluten intake and CD risk differed by genetic susceptibility to CD, we examined this association separately in case–control pairs that were homozygous for the matching variable DR3-DQ2, pairs that were heterozygous for DR3-DQ2, and pairs without DR3-DQ2. In DR3-DQ2 homozygotes, children who received gluten in the upper tertile (high gluten intake) had a 3-fold higher risk for celiac disease than those who received less (OR= 3.19; 95% CI=1.61–6.30; p=0.001). A similar association was seen in DR3-DQ2 heterozygotes (OR=2.24; 95% CI=1.08–4.62; p=0.030) and in children negative for DR3-DQ2 (OR=2.43; 95% CI=0.90–6.54; p=0.079), albeit the latter did not reach statistical significance.
Discussion
In this nested case–control study, we demonstrated that a high overall intake of gluten during the first two years of life, and in particular at 12 months of age is associated with increased risk for CD during childhood. More importantly, this association did not differ between children at very high or increased genetic risk for the disease; a high quantity of gluten was still associated with CD in children with no, one or two copies of the major celiac disease risk HLA-DR3-DQ2 haplotype. These findings may contribute to a better understanding of why some but not all children at genetic risk develop CD.
Gluten-derived peptides are able to induce immune responses in individuals with DR3-DQ2 as well as with DR4-DQ8.23 The disease risk is furthermore modified by genotype where DR3-DQ2 homozygous individuals develop CD at an early age.24 It has been hypothesized that the threshold of tolerance to gluten is dependent on the HLA genotype.25 However, this proposed threshold model is only supported by in vitro studies demonstrating that the strongest T cell response is seen amongst DR3-DQ2 homozygous individuals who need only a small quantity of stimulatory gluten peptides to activate an immune response.26 In this study, time to seroconversion of tTGA occurred a median 12 months earlier amongst the high risk group (DR3-DQ2 homozygous) than amongst the remaining cases with standard risk. It is thus tempting to speculate that the gluten intake needed for triggering CD was dependent on HLA-risk genotype in this study. However, we found no indication that the gluten intake according to tertile distribution differed among cases carrying different HLA risk genotypes, indicating that the amount was an independent risk factor for CD to develop.
Only two important studies have reported on the amount of gluten intake and subsequent risk for CD. In the European PREVENTCD study, mean daily intake (after dose escalation) was not associated with increased risk for CD.9 In contrast, another study indicated that the risk of CD was increased in Swedish children before 2 years of age introduced to gluten in large amounts during weaning.11 Swedish feeding practices differ from other European countries and the US, also confirmed in the TEDDY cohort.27 It is traditional to feed infants with cereal-based foods in Sweden. Moreover, Swedish infants are first introduced to gluten-containing foods at an earlier age and in larger amounts as compared to other Nordic countries.8,14,28 By tradition, most common cereal-based foods given to Swedish infants are cereal in milk formulations (gruel) or spoon fed porridges, which are nutritionally similar products. At the age of 6 months, 60% of Swedish children were bottle-fed with 250–500 ml of gruel per day and almost all infants were given porridge.29 The major source of gluten in gluten-containing commercial baby foods comes from wheat and rye flour. In Sweden, gruels and porridges are available in numerous brands and for different age groups. The gluten-content in these types of products is between 0.3–0.7 g gluten per 100 g of prepared product (data based on the recipes created in the Swedish nutrient database). In our study, we showed a sharp increase in the reported amount of gluten between 9 to 12 months of age. This is typically the time when many infants are given gluten-containing commercial feeding products in Sweden. This could suggest that porridges and gruel given in large amounts modulate the risk of CD during early childhood in Sweden after controlling for HLA-risk genotype.13
The strength of the present study is the prospective design with the use of a 3-day food record for the dietary assessment of early childhood food consumption. This method provides a more accurate estimation about gluten intake compared to dietary assessment methods using standard portions such as food frequency questionnaires. During the first year of life, parents kept a food record frequently and with a very high compliance rate. The face-to-face visits made it possible to probe about missing portion sizes which maximized the efforts of collecting complete data. The prospective design of this birth cohort study enables us to get the diet information prior to seroconversion of tTGA as a marker of CD. This eliminates the risk of reporting biases or a change in feeding habits due to the knowledge of serology results or disease status. A potential weakness of the study is that we did not analyze information about the number of servings of gluten-containing foods per day. We cannot exclude the possibility for example that the number of portions given frequently during the course of the day may have different effects on disease risk.
In conclusion, this study demonstrates that a high intake of gluten during the first two years of life is associated with an increased risk of CD. This association was similar in children carrying any of the major HLA-risk genotypes for CD. Since these HLA-risk genotypes also are widely distributed in the general population, our findings may therefore have consequence for future infant feeding recommendations. Future studies from other countries are warranted to confirm if gluten intake during infancy triggers celiac disease in young children.
Supplementary Material
Acknowledgments
The authors express their gratitude to the families who participated in the study. This study is funded by U01 DK63829, U01 DK63861, U01 DK63821, U01 DK63865, U01 DK63863, U01 DK63836, U01 DK63790, UC4 DK63829, UC4 DK63861, UC4 DK63821, UC4 DK63865, UC4 DK63863, UC4 DK63836, UC4 DK95300, and UC4 DK100238, and Contract No. HHSN267200700014C from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), National Institute of Allergy and Infectious Diseases (NIAID), National Institute of Child Health and Human Development (NICHD), National Institute of Environmental Health Sciences (NIEHS), Juvenile Diabetes Research Foundation (JDRF), and Centers for Disease Control and Prevention (CDC). This work supported in part by the NIH/NCATS Clinical and Translational Science Awards to the University of Florida (UL1 TR000064) and the University of Colorado (UL1 TR001082).
Abbrevations
- CD
celiac disease
- HLA
human leukocyte antigen
- tTGA
tissue transglutaminase autoantibodies
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosures:
The authors have indicated they have no potential conflicts of interest to disclose. Also, the authors have indicated they have no financial relationships to this work to disclose.
Author contributions:
Ms Aronsson worked with the data collection, drafted the initial manuscript, interpreted the data, and completed all subsequent revisions until submission. Dr Lee conducted the statistical analyses and critically reviewed the manuscript. Drs. Uusitalo, Yang, Koletzko, Liu, and Lernmark interpreted the data and reviewed and revised the manuscript. Drs. Virtanen, Norris, and Agardh conceptualized the present analysis, advised in presentation of analysis results, and revised the drafts critically for important intellectual content. All authors approved the final manuscript as submitted, and all authors have agreed to be accountable for all aspects of the work, ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
References
- 1.Ludvigsson JF, Green PH. Clinical management of coeliac disease. J Intern Med. 2011;269(6):560–571. doi: 10.1111/j.1365-2796.2011.02379.x. [DOI] [PubMed] [Google Scholar]
- 2.Catassi C, Gatti S, Fasano A. The new epidemiology of celiac disease. J Pediatr Gastroenterol Nutr. 2014;59:S7–9. doi: 10.1097/01.mpg.0000450393.23156.59. [DOI] [PubMed] [Google Scholar]
- 3.Sollid LM, Thorsby E. HLA susceptibility genes in celiac disease: genetic mapping and role in pathogenesis. Gastroenterology. 1993;105(3):910–922. doi: 10.1016/0016-5085(93)90912-v. [DOI] [PubMed] [Google Scholar]
- 4.Hunt KA, Zhernakova A, Turner G, et al. Newly identified genetic risk variants for celiac disease related to the immune response. Nat Genet. 2008;40(4):395–402. doi: 10.1038/ng.102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ivarsson A, Persson LA, Nyström L, et al. Epidemic of coeliac disease in Swedish children. Acta Paediatr. 2000;89:165–171. doi: 10.1080/080352500750028771. [DOI] [PubMed] [Google Scholar]
- 6.Ivarsson A, Myléus A, Norström F, et al. Prevalence of childhood celiac disease and changes in infant feeding. Pediatrics. 2013 Mar;131(3):e687–94. doi: 10.1542/peds.2012-1015. [DOI] [PubMed] [Google Scholar]
- 7.Stördal K, White RA, Eggesbö M. Early feeding and risk of celiac disease in a prospective birth cohort. Pediatrics. 2013;132:e1202–e1209. doi: 10.1542/peds.2013-1752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aronsson CA, Lee H, Liu E, et al. Age at gluten introduction and risk for celiac disease. Pediatrics. 2015;135(2):239–45. doi: 10.1542/peds.2014-1787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Vriezinga SM, Auricchio R, Bravi E, et al. Randomized feeding intervention in infants at high risk for celiac disease. N Eng J Med. 2014;371:1304–1315. doi: 10.1056/NEJMoa1404172. [DOI] [PubMed] [Google Scholar]
- 10.Lionetti E, Castellaneta S, Francavilla R, et al. Introduction of gluten, HLA status and the risk of celiac disease in children. N Eng J Med. 2014;371(14):1295–1303. doi: 10.1056/NEJMoa1400697. [DOI] [PubMed] [Google Scholar]
- 11.Ivarsson A, Hernell O, Stenlund H, Persson LA. Breast-feeding protects against celiac disease. Am J Clin Nutr. 2002;75:914–921. doi: 10.1093/ajcn/75.5.914. [DOI] [PubMed] [Google Scholar]
- 12.TEDDY Study group. The Environmental determinants of Diabetes in The Young (TEDDY) study: study design. Pediatric Diabetes. 2007;8:286–298. doi: 10.1111/j.1399-5448.2007.00269.x. [DOI] [PubMed] [Google Scholar]
- 13.Liu E, Lee H, Aronsson CA, et al. HLA Haplotype and country and the risk of celiac disease in early childhood. N Eng J Med. 2014;371:42–49. doi: 10.1056/NEJMoa1313977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Weile B, Cavell B, Nivenius K, Krasilnikoff PA. Striking differences in the incidence of childhood celiac disease between Denmark and Sweden: a plausible explanation. J Pediatr Gastroenterol Nutr. 1995;21(1):64–68. doi: 10.1097/00005176-199507000-00011. [DOI] [PubMed] [Google Scholar]
- 15.TEDDY Study group. The Environmental Determinants of Diabetes in The Young (TEDDY) study. Ann NY Acad Sci. 2008;1150:1–13. doi: 10.1196/annals.1447.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hagopian WA, Erlich H, Lernmark Å, et al. The Environmental Determinants of Diabetes in The Young (TEDDY): genetic criteria and international diabetes risk screening of 410 000 infants. Pediatric Diabetes. 2011;12:733–743. doi: 10.1111/j.1399-5448.2011.00774.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Vehik K, Fiske SW, Logan CD, et al. Methods, quality control and specimen management in an international multi-center investigation of type 1 diabetes: TEDDY. Diabetes Metab Res Rev. 2013;29(7):557–67. doi: 10.1002/dmrr.2427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yang J, Lynch KF, Uusitalo U, et al. Factors associated with longitudinal food record compliance in a paediatric cohort study. Public Health Nutr. 2015 Jun 19;:1–10. doi: 10.1017/S1368980015001883. [Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Koskinen O, Villanen M, Korponay-Szabo I, Lindfors K, Mäki M, Kaukinen K. Oats do not induce systemic or mucosal autoantibody response in children with coeliac disease. J Pediatr Gastroenterol Nutr. 2009;48:559–565. doi: 10.1097/MPG.0b013e3181668635. [DOI] [PubMed] [Google Scholar]
- 20.Uusitalo U, Kronberg-Kippilä C, Andren Aronsson C, et al. Food composition database harmonization for between-country comparisons of nutrient data in the TEDDY Study. J Food Compost Anal. 2011;24(4–5):494–505. doi: 10.1016/j.jfca.2011.01.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.National Food Agency, Uppsala, Sweden. The Swedish Food Composition Database. Available at: http://www.slv.e/en-gb/Group1/Food-and-Nutrition/The-Food-Database/ Assessed November 20,2014.
- 22.van Overbeek FM, Uil-Dieterman IG, Mol IW, Köhler-Brands L, Heymans HS, Mulder CJ. The daily gluten intake in relatives of patients with coeliac disease compared with that of the general Dutch population. Eur J Gastroenterol Hepatol. 1997;9(11):1097–1099. doi: 10.1097/00042737-199711000-00013. [DOI] [PubMed] [Google Scholar]
- 23.Arentz-Hansen H, McAdam SN, Molberg Ö, et al. Celiac lesion T cells recognize epitopes that cluster in regions of gliadines rich in proline residues. Gastroenterology. 2002;123(3):803–809. doi: 10.1053/gast.2002.35381. [DOI] [PubMed] [Google Scholar]
- 24.Mearin ML, Biemond I, Peña AS, et al. HLR-DR phenotypes in Spanish coeliac children: their contribution to the understanding of the genetics of the disease. Gut. 1983;24(6):532–537. doi: 10.1136/gut.24.6.532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tjon J, van Bergen J, Koning F. Celiac disease: how complicated can it get? Immunogenetics. 2010;62:641–651. doi: 10.1007/s00251-010-0465-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Vader W, Stepniak D, Kooy Y, et al. The HLA-DQ2 gene dose effect in celiac disease is directly related to the magnitude and breadth of gluten-specific T cell responses. Proc Natl Acad Sci USA. 2003;100(21):12390–5. doi: 10.1073/pnas.2135229100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Andrén Aronsson C, Uusitalo U, Vehik K, et al. Age at first introduction to complementary foods is associated with sociodemographic factors in children with increased genetic risk of developing type 1 diabetes. Matern Child Nutr. 2013 Sep 13; doi: 10.1111/mcn.12084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ascher H, Holm K, Kristiansson B, Mäki M. Different features of coeliac disease in two neighbouring countries. Arc Dis Child. 1993;69:375–380. doi: 10.1136/adc.69.3.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Almquist-Tangen G, Dahlgren J, Rosvall J, Berman S, Alm B. Milk cereal drink increases BMI risk at 12 and 18 months, but formula does not. Acta Paediatrica. 2013;102:1174–1179. doi: 10.1111/apa.12418. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.