

Abstract
Technetium-99m (99mTc) sestamibi myocardial perfusion scintigraphy (MPI) is widely used for the diagnosis and assessment of prognosis in patients with suspected coronary artery disease. During these investigations, inspection of raw projected data for the purpose of quality control may occasionally yield incidental noncardiac findings that suggest the presence of another primary noncardiac disease. We present a 66-year-old HIV patient with a tissue diagnosis of lymphoid interstitial pneumonitis (LIP), who demonstrated a diffuse increase of 99mTc sestamibi in bilateral lung fields both in rest and stress MPI.
Abbreviations: MPI, Technetium-99m sestamibi myocardial perfusion scintigraphy; CT, computed tomography; MRI, magnetic resonance imaging; LIP, lymphoid interstitial pneumonitis; SPECT, single-photon-emission computed tomography; HRCT, high-resolution computed tomography
Case report
A 66-year-old male, scheduled for an elective thyroidectomy following a recently diagnosed papillary thyroid carcinoma, presented with progressive dyspnea. His past medical history was significant for type-II diabetes, hyperlipidemia, HIV, and hepatitis C-related cirrhosis. His management included diabetic diet, atorvastatin, and highly active anti-retroviral therapy (HAART). He denied any prior cardiac history or coronary interventions. Given his cardiac risk factors and limited exercise tolerance, he was referred for myocardial SPECT imaging as a part of the pre-operative workup. Rest images were obtained 30 minutes following the administration of 12.5 mCi of 99mTc sestamibi, and then stress images were obtained 45 minutes after injection of 36.5 mCi of 99mTc sestamibi during a dipyridamole infusion.
A review of the raw projected cine images demonstrated diffusely increased pulmonary uptake of the radiotracer both at both rest and under stress (Figure 1, Figure 2).
Figure 1.
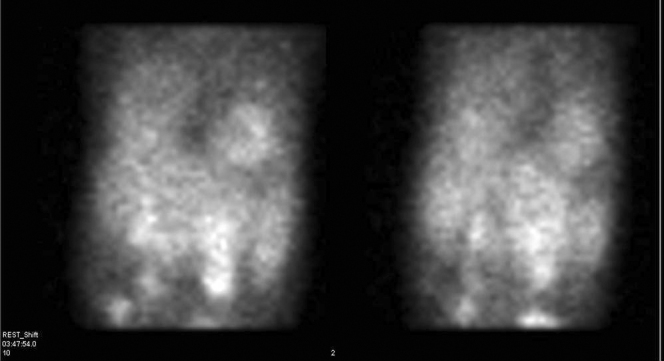
66-year-old male with HIV-associated lymphocytic interstitial pneumonitis. 99mTc sestamibi resting images of the heart, showing diffusely increased pulmonary uptake of the radiotracer.
Figure 2.
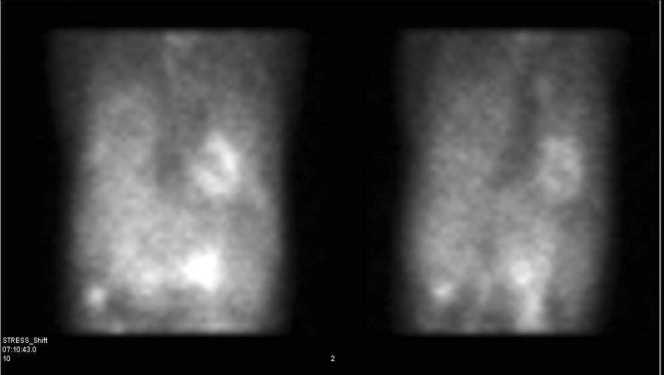
66-year-old male with HIV-associated lymphocytic interstitial pneumonitis. 99mTc sestamibi stress images of the heart, showing diffusely increased pulmonary uptake of the radiotracer.
The lung/heart ratio (LHR) was 0.62 at rest and 0.63 under stress (normal value: 0.42). The LHR is measured by drawing the region of interest over the anterolateral wall of the myocardium and over the mid to lower third of the lung. Further interpretation of the perfusion and gated tomographic images demonstrated a normal perfusion pattern under stress and at rest, normal LV wall motion, normal LV volumes, and an ejection fraction of 62% (normal > 55%).
Based on the normal MPI findings and the diffuse pulmonary uptake of the radiotracer, we investigated additional correlative imaging. A review of the patient's prior chest x-ray showed the presence of diffuse, bilateral reticulonodular lung opacities that were more prominent at the bases (Fig. 3).
Figure 3.

66-year-old male with HIV-associated lymphocytic interstitial pneumonitis. PA radiograph of the chest, showing diffuse, bilateral reticulonodular lung opacities most prominent at the bases.
Chest CT examination revealed a similar distribution of a patchy ground-glass appearance throughout both lungs (Fig. 4).
Figure 4.
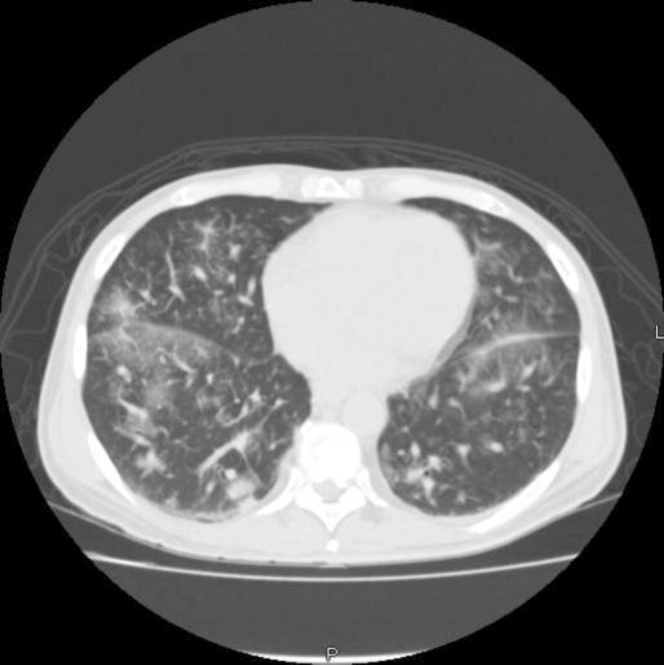
66-year-old male with HIV-associated lymphocytic interstitial pneumonitis. Axial CT of the chest, showing patchy ground-glass appearance throughout both lungs.
These findings were consistent with a generalized infectious/inflammatory pulmonary pathology. However, in this patient with primary thyroid carcinoma, radiological findings could not altogether rule out the presence of metastatic pulmonary disease. The patient subsequently underwent a transbronchial lung biopsy, which confirmed the findings of lymphoid interstitial pneumonitis (LIP) (Fig. 5). The cultures of the bronchial brushings obtained during the tissue biopsy were negative for infectious etiology, including bacterial and fungal organisms. Serum titers for Epstein Barr virus were also negative.
Figure 5.
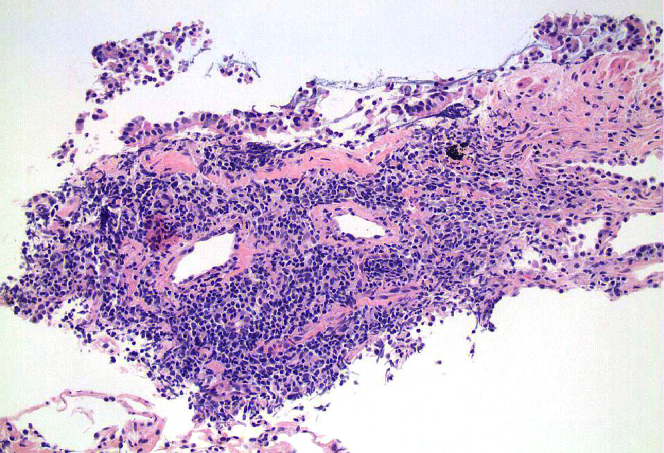
66-year-old male with HIV-associated lymphocytic interstitial pneumonitis. Low-power magnification view of transbronchial lung biopsy, showing features of LIP, with expansion of the alveolar interstitium by mononuclear inflammatory cell infiltrates.
Discussion
Although 99mTc-sestamibi was developed initially as an agent for MPI, several studies have shown that it accumulates in cardiac and extracardiac tissues, depending on the etiologic processes involved. An intense and discrete uptake of the radiotracer is commonly seen with viable tumors including thyroid (1), breast (2, 3), lung cancers, lymphomas (4, 5, 6), musculoskeletal sarcomas (7), and carcinoid tumors (8); focal inflammatory processes and pulmonary thromboembolism (PE) (9) also demonstrate a similar uptake. On the other hand, a diffuse increase in the pulmonary uptake of 99mTc sestamibi occurs in a variety of inflammatory and hypermetabolic processes affecting the myocardial and pulmonary tissues.
The exact mechanisms underlying the 99mTc sestamibi uptake in the different etiologies mentioned thus far are not clearly understood. They are thought to relate to the radiopharmaceuticals’ chemical characteristics, the cationic charge, the lipophilic properties, and the negative transmembrane potentials generated in the cytoplasm and mitochondria of metabolically active cells (10). In order to seek additional correlative tests and to establish a diagnosis, it is vital to have knowledge of the differential conditions that result in the increased uptake of 99mTc sestamibi as well as the pharmacokinetic characteristics of the MPI radiotracer used.
In the present case, diffusely increased lung uptake of 99mTc sestamibi was noted on routine MPI SPECT both under stress and at rest. The increased uptake can be easily quantified as lung-to-heart ratios (LHR) both under stress and at rest by drawing regions of interest in the upper lung field and the anterolateral wall of the myocardium in the anterior planar views. Elevated LHRs in patients referred for MPI with suspected or confirmed cardiac disease are known to correlate well with the degree and severity of left ventricular systolic dysfunction (LVSD) and angiographic coronary artery disease (CAD). In the absence of cardiac disease (11, 12, 13, 14), these findings may indicate the presence of underlying pulmonary processes. However, LHRs by MPI are nonspecific in discriminating between the various pulmonary etiologies.
Some of these etiologies include chronic smoking (15), chemical pneumonitis (16), atypical pneumonias (P. carinii, MAC), and interstitial pneumonitis secondary to systemic sclerosis (17), all of which were ruled out in our patient. Rarely, HIV is known to cause LIP, which is an inflammatory reaction of the lung interstitium to the virus. In the absence of the aforementioned etiologies and the presence of HIV infection, the radiotracer uptake in both the lungs as seen in our patient may most likely represent LIP.
LIP is an inflammatory, lymphoproliferative, nonneoplastic process representing a pulmonary reaction to various external stimuli or systemic diseases. It appears that a transient lymphocytic alveolitis develops in some HIV-positive patients as an immune response to the HIV virus, which in a certain percentage of individuals evolves into LIP (18). The classical radiograph presentation is of bilateral, predominantly lower-zone nodular or reticulonodular opacities with or without variable areas of consolidation. On HRCT, this corresponds to patchy bilateral and diffuse ground-glass opacities (19).
The imaging findings represent a summation of lymphoid cellular infiltrates noted histologically within the lung interstitium. Since 99mTc sestamibi is known to be taken up by inflammatory cells, the presence of lymphoid infiltrates in the interstitium of the lungs might explain the isolated findings of bilateral diffusely increased uptake of the radiotracer throughout both the lung fields with normal myocardial perfusion and function. However, neither the MPI findings nor the radiological image findings are specific, so a tissue biopsy and histologic examination is warranted to confirm the diagnosis of LIP (20). Thus, it is reasonable to conclude that the development of LIP in our patient may have been entirely due to his HIV infection, since all other possible etiologies have been excluded.
While LIP is known to be one of the criteria for defining acquired immunodeficiency syndrome (AIDS) in children, it is still considered unusual in HIV-positive adults (21). It is often an incidental finding rather than the patient’s presenting complaint, since the disease follows an indolent course, in stark contrast to the acute nature of HIV-related pulmonary infections. Thus, clinically this case is unique in that the patient presented with progressive dyspnea arising presumably from a HIV-associated LIP. Further, the presence of cardiac risk factors and an underlying primary malignancy complicated the diagnosis, requiring a complete workup including several imaging modalities before confirmation with tissue cultures and biopsy.
Conclusion
Although HIV-associated LIP in adults is unusual, knowledge of its presence is particularly important in interpretation of those subgroups undergoing 99mTc sestamibi MPI scans where HIV and cardiac risk factors are known to coexist. A careful and systematic review of the raw projection data in these patients is therefore essential both for the purpose of quality control and to detect noncardiac findings that may guide further workup for appropriate relevance (22).
Footnotes
Published: November 28, 2009
References
- 1.Sundram FX, Mack P. Evaluation of thyroid nodules for malignancy using 99mTc- sestamibi. Nucl Med Commun. 1995;16(8):687–693. doi: 10.1097/00006231-199508000-00011. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Waxman AD. The role of 99mTc methoxyisobutylisonitrile in imaging breast cancer. Semin Nucl Med. 1997;27(1):40–54. doi: 10.1016/s0001-2998(97)80035-9. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Khalkhali I, Cutrone J, Mena I, Diggles L, Venegas R, Vargas H. Technetium-99m-sestamibi scintimammography of breast lesions: clinical and pathological follow-up. J Nucl Med. 1995;36(10):1784–1789. [PubMed] [PubMed] [Google Scholar]
- 4.Nishiyama Y, Kawasaki Y, Yamamoto Y, Fukunaga K, Satoh K, Takashima H. Technetium-99m-MIBI and thallium-201 scintigraphy of primary lung cancer. J Nucl Med. 1997;38(9):1358–1361. [PubMed] [PubMed] [Google Scholar]
- 5.Bom HS, Kim YC, Song HC, Min JJ, Kim JY, Park KO. Technetium-99m-MIBI uptake in small cell lung cancer. J Nucl Med. 1998;39(1):91–94. [PubMed] [PubMed] [Google Scholar]
- 6.Matsui R, Komori T, Narabayashi I, Namba R, Nakata Y, Tabuchi K. 99mTc sestamibi uptake by malignant lymphoma and slow washout. Clin Nucl Med. 1995;20(4):352–356. doi: 10.1097/00003072-199504000-00013. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Söderlund V, Jonsson C, Bauer HC, Brosjö O, Jacobsson H. Comparison of technetium-99m-MIBI and technetium-99m-tetrofosmin uptake by musculoskeletal sarcomas. J Nucl Med. 1997;38(5):682–686. [PubMed] [PubMed] [Google Scholar]
- 8.Arbab AS, Koizumi K, Arai T, Araki T, Ozawa K, Hashimoto R. 99mTc MIBI uptake in a bronchial carcinoid tumor. Clin Nucl Med. 1996;21(12):1005–1006. doi: 10.1097/00003072-199612000-00031. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.Wittram C, Jones SE, Scott JA. 99mTc sestamibi uptake by acute pulmonary embolism. AJR Am J Roentgenol. 2006;187(6):1611–1613. doi: 10.2214/AJR.05.0476. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Piwnica-Worms D, Kronauge JF, Chiu ML. Uptake and retention of hexakis (2-methoxyisobutyl isonitrile) technetium (I) in cultured chick myocardial cells: mitochondrial and plasma membrane potential difference. Circulation. 1990;82:1826–1838. doi: 10.1161/01.cir.82.5.1826. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Choy JB, Leslie WD. Clinical correlates of 99mTc sestamibi lung uptake. Journal of Nuclear Cardiology. Journal of Nuclear Cardiology. 2001;8:639–644. doi: 10.1067/mnc.2001.116854. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Giubbini R, Campini R, Milan E, Zoccarato O, Orlandi C, Rossini P. Evaluation of technetium-99m-sestamibi lung uptake: correlation with left ventricular function. J Nucl Med. 1995;36:58–63. [PubMed] [PubMed] [Google Scholar]
- 13.Hurwitz GA, Ghali SK, Husni M, Slomka PJ, Mattar AG, Reid RH. Pulmonary uptake of technetium-99m-sestamibi induced by dipyridamole-based stress or exercise. J Nucl Med. 1998;39:339–345. [PubMed] [PubMed] [Google Scholar]
- 14.Romanens M, Gradel C, Saner H, Pfisterer M. Comparison of 99mTc-sestamibi lung/heart ratio, transient ischaemic dilation and perfusion defect size for the identification of severe and extensive coronary artery disease. Eur J Nucl Med. 2001;28:907–910. doi: 10.1007/s002590100532. [PubMed] [DOI] [PubMed] [Google Scholar]
- 15.Kao CH, Shen YY, Lee JK. Effects of smoking on pulmonary uptake of technetium-99m methoxy-isobutyl-isonitrile during myocardial perfusion imaging. J Nucl Cardiol. 1999;6:29–32. doi: 10.1016/s1071-3581(99)90062-4. [PubMed] [DOI] [PubMed] [Google Scholar]
- 16.Pham R, Bellezuoli E. R. Diffuse pulmonary uptake of 99mTc sestamibi due to chemical pneumonitis. J Nucl Cardiol. 2006;13:127–129. doi: 10.1016/j.nuclcard.2005.12.006. [PubMed] [DOI] [PubMed] [Google Scholar]
- 17.Richard M, Cox D, Earle L, Varga J. Abnormal uptake of 99mTc MIBI, a novel myocardial imaging agent, in the lungs of patients with systemic sclerosis. J. Clin Nucl Med. 1998;23:19–25. doi: 10.1097/00003072-199801000-00007. [PubMed] [DOI] [PubMed] [Google Scholar]
- 18.Swigris JJ, Berry GJ, Raffin TA. Lymphoid interstitial pneumonia, a narrative review. Chest. 2002;122:2160–2164. doi: 10.1378/chest.122.6.2150. [PubMed] [DOI] [PubMed] [Google Scholar]
- 19.Oldham SA, Castillo M, Jacobson FL. HIV-associated lymphocytic interstitial pneumonia: Radiologic manifestations. and pathologic correlation. Radiology. 1989;170:83–87. doi: 10.1148/radiology.170.1.2909125. [PubMed] [DOI] [PubMed] [Google Scholar]
- 20.McGuinness G, Scholes JV, Jagirdar JS. Unusual lymphoproliferative disorders in nine adults with HIV or AIDS: CT and pathological findings. Radiology. 1995;197:59–65. doi: 10.1148/radiology.197.1.7568855. [PubMed] [DOI] [PubMed] [Google Scholar]
- 21.Das S, Miller RF. Lymphocytic interstitial pneumonitis in HIV infected adults. Sex Transm Infect. 2003;79:88–93. doi: 10.1136/sti.79.2.88. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jones SE, Aziz K, Yasuda T, Gewirtz H, Scott JA. Importance of systematic review of rotating projection images from 99mTc-sestamibi cardiac perfusion imaging for noncardiac findings. Nuclear medicine communications. 2008;29:607–613. doi: 10.1097/MNM.0b013e3282f813f3. [PubMed] [DOI] [PubMed] [Google Scholar]