

Abstract
Over the past few years, several studies have demonstrated favorable clinical outcomes and low complication rates using the ankle Tightrope® syndesmosis fixation system. The traditional surgical procedure of screw fixation for syndesmosis injury is associated with high complication rates of loosening, screw fracture, nonanatomic fixation, and postoperative syndesmotic diastasis. It is expected that the Tightrope® technique will become more common practice given the recent successful reports, so it is important for radiologists to be aware of this novel surgical technique and its imaging appearance.
Abbreviations: CT, computed tomography
Case report
A 59-year-old woman who sustained a right fibular Weber C fracture after a minor fall (Fig. 1) underwent open reduction, internal fixation, and syndesmosis repair at an outside institution using three syndesmotic screws and a 3.5-mm dynamic compression plate.
Figure 1.

59-year-old woman with right fibular fracture. AP radiograph of the right ankle demonstrates fracture of the distal one-third shaft of the fibula and widening of the distal tibiofibular joint with the tibia medially dislocated. Findings are consistent with a Weber C fracture with syndesmotic disruption.
Ten months later, the patient presented to our foot and ankle clinic with progressive, severe right ankle pain and inability to ambulate without assistance of a walker and boot. Plain radiographs of the ankle demonstrated widening of the lateral ankle mortise and lucency surrounding all three syndesmotic screws, concerning for hardware loosening (Fig. 2).
Figure 2.

59-year-old woman with right fibular fracture. Plain radiograph of the right ankle shows lateral plate and screw internal fixation of the distal fibula fracture, which has healed. There are also three syndesmotic screws with surrounding lucency, suggestive of loosening. Widening of the distal tibiofibular joint and heterotopic ossification is seen.
Noncontrast CT weight-bearing examination of the right ankle demonstrated heterotopic ossification of the distal tibiofibular joint and loosening of all three syndesmotic screws (Fig. 3).
Figure 3.

59-year-old woman with right fibular fracture. Coronal-plane weight-bearing CT of the right ankle in bone window demonstrates widening of the distal tibiofibular joint.
The patient subsequently underwent surgical revision to address her symptoms. Intraoperatively, all three syndesmotic screws were found to be loose and were removed. Heterotopic ossification of the distal tibiofibular joint was excised. Revision was performed using the ankle Tightrope® syndesmosis reconstruction technique. Postoperative radiographs demonstrated a lucent tunnel extending transversely across the syndesmosis, secured by metal buttons along the distal medial tibial and lateral fibular cortices (Fig. 4).
Figure 4.

59-year-old woman with right fibular fracture. AP radiograph of the right ankle demonstrates a new lateral fibular plate with one fibular screw and three syndesmotic screws. A radiolucent transverse tunnel is seen parallel to the plafond, consistent with the Tightrope® suture system. An oblong button is present along the medial tibia cortex, and a round button is present against the distal hole of the fibular plate. Widening of the distal tibiofibular joint has been reduced.
Postoperative CT demonstrated reduction of the lateral ankle mortise widening and a new lucent tunnel parallel to the ankle plafond, traversing the syndesmosis and secured by two metal buttons (Figure 5a, Figure 5b). No complications were evident two weeks postoperatively on clinical examination.
Figure 5a.

59-year-old woman with right fibular fracture. Axial CT of the right ankle in bone window demonstrates a round metal button along the medial tibial cortex and a low attenuation tunnel extending along the tibiofibular joint.
Figure 5b.

59-year-old woman with right fibular fracture. Coronal CT of the right ankle in bone window demonstrates the new Tightrope® tunnel and normal distal tibiofibular joint space.
Discussion
Disruption of the tibiofibular syndesmosis occurs in 10-15% of patients with ankle fractures, particularly Weber type B and C fractures (1, 2, 3, 4, 5). The syndesmosis is also injured in mechanisms of severe abduction or external rotation at the ankle joint (6, 7) or in cases of proximal fibula fracture with interosseus ligament disruption (Maisonneuve fracture). Surgical management of syndesmotic injury is imperative to prevent ankle instability and secondary osteoarthritis. Standard treatment involves placement of syndesmotic screws with or without lateral fibular plating. Unfortunately, this technique is associated with several issues, including nonanatomic reduction, screw fracture and loosening, rigidity at a normally mobile joint, revision surgery, and an extended postoperative period of protective weight-bearing (8, 9, 10, 11).
A novel technique of surgical management is the Arthrex syndesmosis Tightrope®, a nonabsorbable fiberwire suture looped twice through center holes of anchored cortical metal buttons (12). The suture resists diastasis of the joint, but under tension allows more movement than a metal screw. Because of the nonabsorbable material, a second surgery is not required to remove the Tightrope®; it is a permanent stabilization system. Prospective studies have demonstrated better American Orthopaedic Foot and Ankle Society scores, earlier return to work, and lower complication rates compared to traditional screw fixation (13, 14).
Intraoperatively, a syndesmosis disruption is corrected using internal rotation with mild plantar flexion while the syndesmosis is compressed (15). A drill hole is made through all four cortices in a parallel manner along the transmalleolar axis, 1-2 cm above the ankle joint. A needle containing the pull-through suture is advanced through the drilled hole from a lateral approach (Fig. 6).
Figure 6.
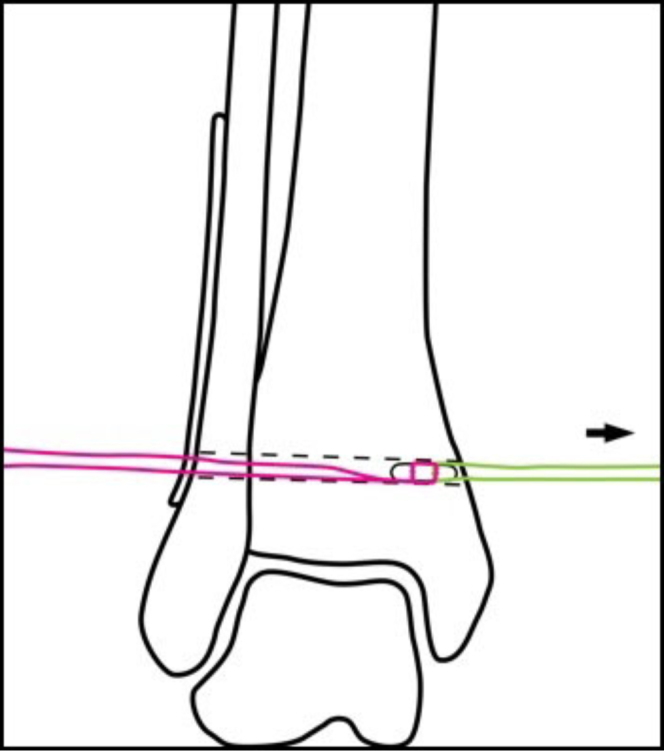
59-year-old woman with right fibular fracture. The oblong button and fiberwire (pink) are passed through the drill hole by the pull-through suture (green).
The suture pulls the oblong button longitudinally across the hole until it can be flipped and attached to the medial tibial cortex. With traction to the ends of the suture, the lateral round button is attached. The suture is tightly tied by hand to stabilize compression (Fig. 7). In cases of Maisonneuve fracture, two Tightropes® may be placed. The procedure requires anatomic fibular alignment, and thus associated fibular fractures usually undergo simultaneous reduction and internal fixation (12).
Figure 7.
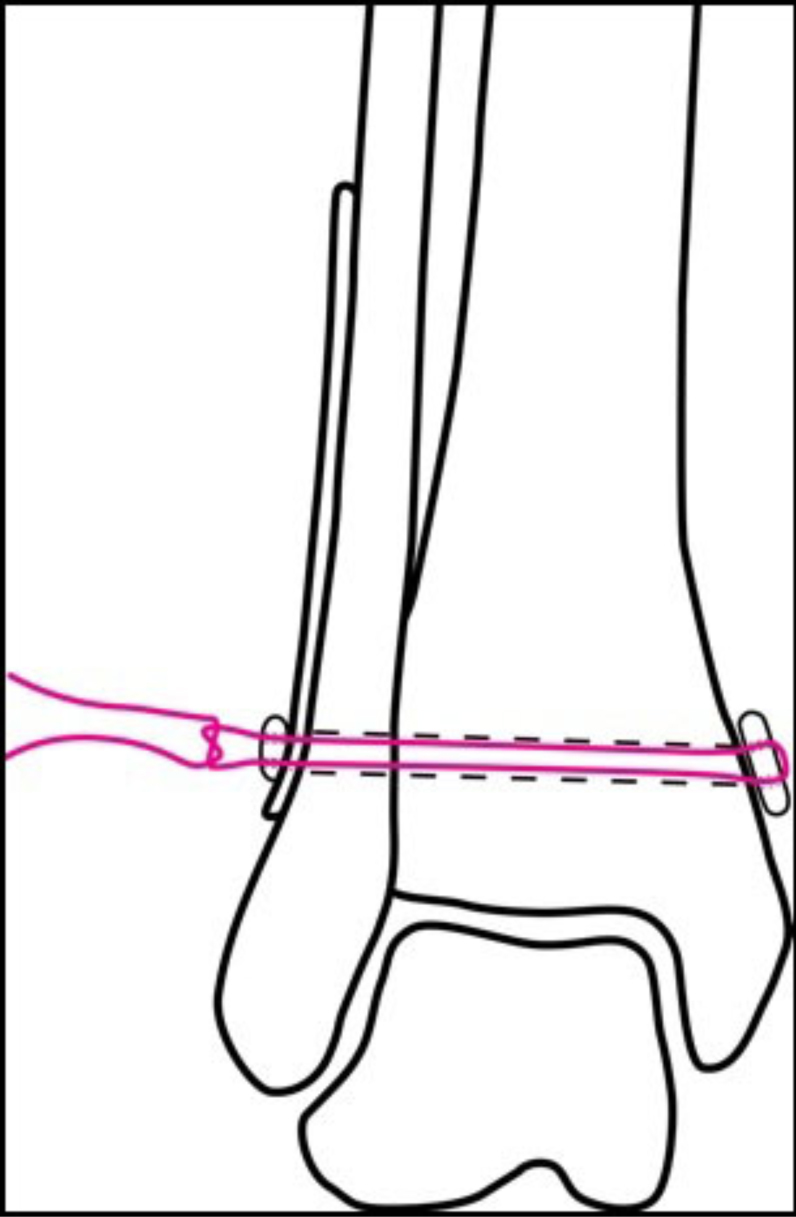
59-year-old woman with right fibular fracture. The oblong button has been flipped perpendicular to the drill hole, and the pull-through suture has been removed. The round lateral button has been threaded over the fiberwire and secured adjacent to the lateral fibular plate with a knot.
On radiographs and CT, a radiolucent tunnel will be seen extending across the distal tibiofibular syndesmosis, parallel to the plafond. An oblong button and round button will be seen against the medial and lateral cortices, respectively. Radiographic findings indicative of a failed procedure include a button that is not in contact with the cortex (suggestive of loosening or inadequate tension), widening of the lateral ankle mortise, and soft-tissue masses adjacent to either button. Such soft-tissue masses represent postoperative formation of granulomatous fibrous tissue, likely due to an inflammatory reaction to the buttons (10, 16), and may require surgical revision.
Tightrope® fixation is a promising technique for surgical repair of ankle syndesmosis injuries, and may eventually replace traditional screw fixation. Musculoskeletal radiologists should be aware of the expected postoperative appearance in these patients, as well as findings suggestive of potential complications.
Footnotes
Published: February 10, 2010
References
- 1.Lindsjo U. Operative treatment of ankle fractures. Acta Orthop Scand. 1981;189(Suppl. 189):1–131. doi: 10.3109/ort.1981.52.suppl-189.01. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Court-Brown CM, McBirnie J, Wilson G. Adult ankle fractures: an increasing problem? Acta Orthop Scand. 1998;69:43–47. doi: 10.3109/17453679809002355. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Clanton TO, Paul P. Syndesmosis injuries in athletes. Foot Ankle Clin. 2002;7(3):529–549. doi: 10.1016/s1083-7515(02)00045-1. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Heim D., Schmidlin V., Ziviello O. Do type B malleolar fractures need a positioning screw? Int. J. Care Injured. 2002;33:729–734. doi: 10.1016/s0020-1383(01)00199-1. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Stark E, Tornetta III, P, Creevy WR. Syndesmotic instability in Weber B ankle fractures: A clinical evaluation. J. Orthop Trauma. 2007;21:63–646. doi: 10.1097/BOT.0b013e318157a63a. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Jensen SL, Andresen BK, Mencke S, Nielsen PT. Epidemiology of ankle fractures: A prospective population-based study of 212 cases in Aalborg, Denmark. Acta Orthop Scand. 1998;69:48–50. doi: 10.3109/17453679809002356. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Michelson J, Solocoff D, Waldman B, Kendell K, Ahn U. Ankle fractures: The Lauge-Hansen classification revisited. Clin Orthop. 1997;345:198–205. [PubMed] [PubMed] [Google Scholar]
- 8.Gardner MJ, Demetrakopoulos D, Briggs SM. Malreduction of the tibiofibular syndesmosis in ankle fractures. Foot Ankle Int. 2006;27:788–792. doi: 10.1177/107110070602701005. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.De Souza LJ, Gustilo RB, Meyer TJ. Results of operative treatment of displaced external rotation and abduction fractures of the ankle. J Bone Joint Surg Am. 1985;67:1066–1074. [PubMed] [PubMed] [Google Scholar]
- 10.Willmott HJS. Injury. 2009 Nov;40(11):1204–1206. doi: 10.1016/j.injury.2009.05.008. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Close JR. Some applications of the functional anatomy of the ankle joint. J. Bone Joint Surg Am. 1956 Jul;38-A(4):761–781. [PubMed] [PubMed] [Google Scholar]
- 12.Thornes B, McCartan D. Ankle syndesmosis injuries treated with the TightRope Suture-Button Kit. Techniques in Foot and Ankle Surgery. 2006;5(1):45–53. [Google Scholar]
- 13.Coetzee JC, Ebeling P. Treatment of syndesmosis disruptions with tightrope fixation. Techniques in Foot and Ankle Surgery. 2008;7(3):196–202. [Google Scholar]
- 14.Thornes B, Shannon F, Guiney A. Suture-button syndesmosis fixation: accelerated rehabilitation and improved outcomes. Clin Orthop. 2005;431:207–212. [PubMed] [PubMed] [Google Scholar]
- 15.Ankle TightRope® Syndesmosis Fixation [Internet]. Naples (FL): Arthrex; 2010 [cited 2010 Feb 7] Available from http://www.ankletightrope.com/
- 16.McMurray D, Hornung B, Venkateswaran Z. Walking on a tightrope: our experience in the treatment of traumatic ankle syndesmosis rupture. Injury Extra. 2008;39:182. [Google Scholar]