

Abstract
Background: EOS is a 2D/3D muscle skeletal diagnostic imaging system. The device has been developed to produce a high quality 2D, full body radiographs in standing, sitting and squatting positions. Three dimensional images can be reconstructed via sterEOS software. This Health Technology Assessment study aimed to investigate efficacy, effectiveness and cost-effectiveness of new emerged EOS imaging system in comparison with conventional x-ray radiographic techniques.
Methods: All cost and outcome data were assessed from Iran's Ministry of Health Perspective. Data for clinical effectiveness was extracted using a rigorous systematic review. As clinical outcomes the rate of x-ray emission and related quality of life were compared with Computed Radiography (CR) and Digital Radiography (DR). Standard costing method was conducted to find related direct medical costs. In order to examine robustness of the calculated Incremental Cost Effectiveness Ratios (ICERs) we used two-way sensitivity analysis. GDP Per capita of Islamic Republic of Iran (2012) adopted as cost-effectiveness threshold.
Results: Review of related literature highlighted the lack of rigorous evidence for clinical outcomes. Ultra low dose EOS imaging device is known as a safe intervention because of FDA, CE and CSA certificates. The rate of emitted X-ray was 2 to 18 fold lower for EOS compared to the conventional techniques (p<0.001). The Incremental Cost Effectiveness Ratio for EOS relative to CR calculated $50706 in baseline analysis (the first scenario) and $50714, $9446 respectively for the second and third scenarios. Considering the value of neither $42146 as upper limit, nor the first neither the second scenario could pass the cost-effectiveness threshold for Iran.
Conclusion: EOS imaging technique might not be considered as a cost-effective intervention in routine practice of health system, especially within in-patient wards. Scenario analysis shows that, only in an optimum condition such as lower assembling costs and higher utilization rates, the device can be recruited for research and therapeutic purposes in pediatric orthopedic centers.
Keywords: EOS imaging, Radiography, Health Technology Assessment, Cost-effectiveness
Introduction
Advances in new technologies have significantly changed the face of medical devices. In addition, new technologies and modern medicine today are so entwined with each other that without these technologies physicians encounter difficulty in treating and diagnosing the diseases. For diagnostic procedures, part from being cost effective in comparison with treatment in advanced stages of a disease, lack of essential accuracy and sensitivity to select technologies in this area can impose a significant financial burden to health system.
EOS imaging system is a novel technique that contains two parts; EOS that creates the whole body image in a standing position and two-dimensional form using low-dose, and Ster-EOS that converts the data to three-dimensional (3D) in standing position. This system consists of two X-ray tubes and two detectors that move up to down in a vertical chamber and takes patients’ pictures from Frontal and Lateral positions. The imaging can be both, partial or whole of the body and it takes around 15 to 20 seconds to scan the entire body. EOS imaging can be done in standing, sitting and reclining position (1). Because, conventional radiology imaging systems such as the Computed Radiography (CR) and Digital Radiography (DR) has problems such as inability of full body imaging and specifying patients’ Skeletal status which is vital for orthopedic specialists, inability of three-dimensional imaging, and inevitability to take images from different views in distinctive times for accurate diagnosis of bone losses with high-dose. It is essential to have an assistant system to optimize imaging process and diminish current risks and problems. As a result, Ster-EOS software was added to EOS system with the ability of creating 3-Dimensional images and detection of patients’ skeletal status (1). From Iranian policymakers’ perspective it is valuable to find whether the new emerged technology is cost-effective or not. This Health Technology Assessment study has been conducted to evaluate the muscle-skeletal EOS imaging system and compare it with the current diagnostic imaging techniques.
Methods
Through a systematic literature review the clinical effectiveness of EOS imaging system was compared with Computed Radiography (CR) and Digital Radiography (DR) (2). The Study population consisted of patients with any orthopedic condition. Related key terms (2D/3D EOS imaging, Low Dose Musculoskeletal Imaging, ster-EOS) were searched across Medline (via PubMed and Ovid SP), the Cochrane library and All EBM Reviews, up to May 2013. In order to find out randomized clinical trial reports the clinical trial registries (Clinical Trials.gov, Trial register. nl and Trialsjournal.com) were searched.
Complementary search was performed in Google scholar, relevant orthopedic journals and the manufacturer’s home pages. Reference list of eligible studies were manually searched for relevant articles. Searches were not limited by date, language or study design. Two reviewers (AM and AV) independently reviewed all titles and abstracts. Any case of disagreement resolved by negotiations.
The Emitted Surface Dose (ESD) level and Dose Area Product (DAP) were employed as measures of radiation dose. Quality adjusted life years (QALYs) were considered as health related outcome. Furthermore, the image quality and workflow of device were compared as a criterion for efficacy.
We assessed the quality of eligible studies using different quality assessment tools. The quality assessment tool for diagnostic accuracy studies (QUADAS) (3) for original studies, CASP (4) and INAHTA (5) checklist for systematic review and HTA reports respectively. All steps were performed by one reviewer and checked by another.
Economic evaluation was done from the perspective of Iran's Ministry of Health. Standard Costing analysis was used to calculate the unit-cost for each imaging service. To calculate the cost of capital goods, straight line depreciation method was used. We used no discount or annuitization for technology costs. But the model presented by McKenna’s study has employed 3% discount rate for modeling of side effect costs. This rate can be relevant for Iranian context (6). Two-way sensitivity analysis was accomplished to examine Incremental Cost Effectiveness Ratio in uncertain conditions. Final conclusion about cost-effectiveness of new technology was driven based on threshold analysis.
Results
Clinical effectiveness of EOS versus CR and DR
We recognized 1497 records from electronic search and 4 extra records through hand search (Fig. 1). Of the 1501 titles, 40 full text articles were selected for screening. A total of 35 full-texts were excluded. After a double checked full text review, 4 papers and 1 HTA report realized as eligible for quality assessment.
Fig. 1 .
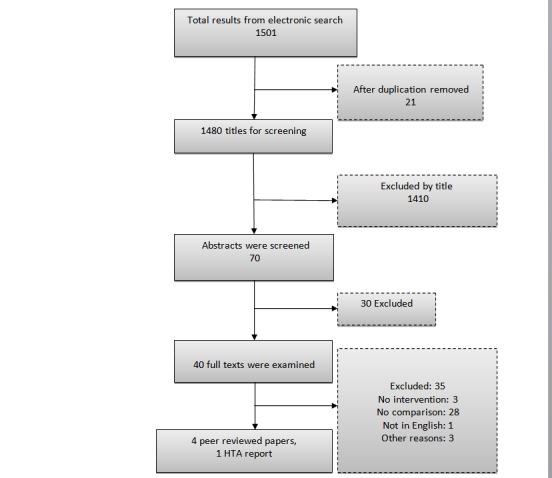
Flow chart of the selection process records
Systematic review revealed the lack of well-designed studies on clinical effectiveness. Quality assessment of included studies depicted several limitations in study designs, population and selected outcome measures. The risk of bias was probable for all studies. Almost studies reported immediate outcomes such as radiation rate, image quality; work flow and patient comfort as the criteria for effectiveness. It is clear that none of these surrogate outcomes could not be translated to patient health or quality of life. Only McKenna’s study had used QALYs as outcome measure which was recognized as one and only patient's health related outcome in this regard (7). Health related quality of life and QALYs were measured based on the effect of X-ray exposure on four most probable cancers (8-10).
The average rate of emitted dose in current imaging techniques relative to EOS has been reported in the range of 2.15 (1) to 18.8 (11). However, the highest rate belongs to Kalifa’s study which has used earlier version of the device (11). It means that the new technology decreases x-ray emission to patient's body from 2.15 to 18.8 fold lesser than conventional techniques.
Result of literature review showed that although the time of imaging process is lower for EOS system, but patients declared they feel discomfort inside the cabin then they estimated imaging time longer than digital radiography (1). Based on the study findings, other outcomes related to patient ease or comfort did not show significant preference to any of the technologies (1).
For Iranian context the only work which attempted to estimate life time costs of cancer was Haghighat’s study (12). In this PhD thesis researchers calculated relevant treatment costs of breast cancer from diagnosis to death. The Discount rate for costs and outcomes was 5 and 10 percent. Because of the absence of data for other three most frequent cancers which could cause by x-ray exposure, the life time cost estimated relative to the breast cancer. The relative value for calculation acquired from McKenna’s study (7). Estimated Cost of breast, lung, colorectal and prostate cancer was 500988500 (US$15656), 759069430 (US$23720), 470407810 (US$14700), 414059140 (US$12939) Rials.
Since there was no real deference between overhead costs of intervention and comparison group, only the direct costs of technology were considered. Market prices and user charges were considered in resource valuation (Table 1).
Table 1 . Direct average cost of new and current imaging techniques .
| EOS | CR | DR | |
| Purchasing, installing, set up and training costs | 550000 | 95000 | 167500 |
| Annual maintenance (Tube and Software costs) | 38438 | 12813 | 25625 |
| Useful lifetime of medical equipment (year) | 10 | ||
| The number of delivered services per year (graph) | 4159 | ||
| The maximum deliverable services per year (graph) | 13824 | 8640 |
The systematic review recognized no significant difference between Computed and Digital Radiography. Therefore, CR dominates DR because of Low average cost of this technique. The rest of analysis was run with comparison of CR and EOS.
Cost effectiveness results
In first scenario we calculated the average cost of one radiography in both groups.
According to data gathered from diagnostic imaging centers, Average cost of each radiograph was calculated based on mean annual production. The ratio of emitted radiation dose for EOS relative to the comparators (18.83, Kalifa's (11)). Euro value in terms of Rials (41000) which is important in valuation of purchasing price of technologies. In the second scenario maximum service provision (throughput) was assumed in which the maximum capacity of each device considered according to manufacturer information. In the third scenario the ratio for radiation dose were changed from least emission rate (11) to most (1). Cost-effectiveness analysis result is showed in Table 2.
Table 2 . Cost-effectiveness Analysis results in pre-defined scenarios (US Dollar) .
| Pre-defined scenarios | EOS | CR |
∆cost US $ |
∆QALY | ICER | ||
| Cost | QALY | Cost | QALY | ||||
| Emitted radiation dose (18.8), Euro value (41000Rialss), Annual throughput (4159) | 27 | 20.85 | 3 | 20.82 | 24 | 0.00049 | 47538 |
| Emitted radiation dose (18.8), Euro value (41000 Rials), Annual throughput (4159) | 27 | 20.85 | 3 | 20.82 | 24 | 0.00049 | 47538 |
| Emitted radiation dose (2.15), Euro value (4100 Rials), Maximum Annual throughput | 8 | 20.82057 | 4 | 20.82008 | 4 | 0.00049 | 8856 |
Discussion
Despite the complications linked to X-ray imaging, application of new technology still remains of great importance and increases in developing countries (13). The results of literature review proved the absence of well-designed RCTs and serious limitation in both quantity and quality of studies. Furthermore, none of relevant trials included health related outcomes, such as Health Related Quality of Life or Quality Adjusted Life Years (QALYs). Then the real impact of X-ray filming on patient’s health remains questionable.
Our study did not find any significant difference in clinical effectiveness of Computed Radiography (CR) and Digital Radiography (DR), thus according to the Cost-Minimization Analysis CR is dominates DR, and considered as comparator to EOS. Unfortunately, with an opposite trend to this evidence, DR is increasingly imported into Iran's medical device market and is executed in the majority of diagnostic centers.
In this health technology assessment study, we considered per capita Gross Domestic Product (GDP) of year 2012 as the threshold for decision making about cost-effectiveness. According to the Iran’s National Accounts, the GDP per capita (2012) was 6815 US dollars. The cost-effectiveness threshold ranges from 6815 as lower limit, to 20445 as upper limit of decision rule. The ICER obtained from the first scenario showed that, cost per each additional QALY is larger than upper threshold of cost-effectiveness. Therefore, in this scenario, new technology is not cost-effective.
The calculated ICER in the first and second scenario (47538 USD) exceeded the threshold of cost-effectiveness and it illustrates, even with assumption of optimum efficacy level which reported in Kalifa's study (11), EOS cannot pass cost-effectiveness threshold and still remains as cost-ineffective intervention. It implies, the claim of manufacturers about dose lowering aspect of new technology might not be proven in real condition.
Sensitivity analysis of uncertainty in national currency indicated, even the value of Euro reduced by half (20000 Rials), the calculated ICER from first and second scenario cannot pass the upper limit of cost-effectiveness to prove EOS as a cost - effective intervention. We can conclude that even without international sanctions and strengthening the national currency which results in low acquisition cost of new technology EOS cannot be taken in to consideration.
Cost per QALY in third scenario reveals a high sensitivity of the cost-effectiveness of EOS technology on service throughput. On the other hand, if the device worked with maximum delivering capacity, and the market demand still is enough, cost per each additional QALY may decrease three times. This finding confirms Tobias’s (1) and McKenna’s conclusions (7). Since there are numerous imaging centers in Iran which can meet the large portion of market demand, as well as the inefficacy of EOS at in-patient settings, the maximum throughput assumption sounds unrealistic condition. Therefore introduction of new technology would provoke over supplying of diagnostic imaging services.
Conclusion
EOS imaging technique cannot be con-sidered as a cost-effective intervention in routine practice of mentioned indications. However because of main benefits associ-ated with the technology (dose reduction) in pediatric and pregnant patients, a limited number of the device for further investigations sounds to be justifiable. This conclusion is in line with NICE’s (The National Institute for Health and Care Excellence) report.
Recommendations for future research
Due to the lack of evidence on clinical effectiveness of EOS imaging, it is recommended that studies to be conducted with proper design to ensure about additional benefits of this technology. Adequate information about health related outcomes especially for cancers within the country is the fundamental of all cost-effectiveness studies. These necessitate the attention of researchers in this area.
Limitations
The Lack of the appropriate information about prices and maintenance costs, lack of appropriate information about the costs of various cancers and quality of life associated with them, as well as the lack of appropriate databases on the incidence and prevalence of abnormalities of the spine, and some problems in accessing to complete articles were some important limitations of this study.
Acknowledgments
We appreciate the Ministry of Health and Education as the founder of the study. Maryam Asadi for her technical notes on technology characteristics. Imagin Center of Sina, Loghman hospitals for their consults on radiography process.
Conflict of interests
The authors declare they have no competing interest.
Cite this article as: Mahboub-Ahari A, Hajebrahimi S, Yusefi M, Velayati A. EOS imaging versus current radiography: A health technology assessment study. Med J Islam Repub Iran 2016 (17 February). Vol. 30:331.
References
- 1.Dietrich TJ, Pfirrmann CW, Schwab A, Pankalla K, Buck FM. Comparison of radiation dose, workflow, patient comfort and financial break-even of standard digital radiography and a novel biplanar low-dose X-ray system for upright full-length lower limb and whole spine radiography. Skeletal Radiol. 2013 Jul;42(7):959–67. doi: 10.1007/s00256-013-1600-0. [DOI] [PubMed] [Google Scholar]
- 2. Velayati A, Mahboub-AhariA, Hajebrahimi S. Comparison of Clinical Effectiveness of EOS Imaging Technology with the Current Methods of Medical Imaging: A Systematic Review. Proceedings of the 7th IHMC, Tehran, Iran 16-17 August 2015.
- 3.Whiting P, Rutjes AW, Reitsma JB, Bossuyt PM, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol. 2003 Nov 10;3:25. doi: 10.1186/1471-2288-3-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Critical Appraisal Skills Programme (CASP), 2014, http://www.systematicreviewsjournal.com/content/supplementary/139-3-4053-2046-s8.pdf. Ox ford.
- 5.Hailey D. Toward Transparency in Health Technology Assessment; A Checklist for HTA Reports. Int J Technol Assess Health Care. 2003 Winter;19(1):1–7. doi: 10.1017/s0266462303000011. [DOI] [PubMed] [Google Scholar]
- 6.Mahboub-Ahari A, Pourreza A, Akbari Sari A, Rahimi Foroushani A, Heydari H. Stated Time Preferences for Health: A Systematic Review and Meta-Analysis of Private and Social Discount Rates. J Res Health Sci. 2014;14(3):181–6. [PubMed] [Google Scholar]
- 7.McKenna C, Wade R, Faria R, Yang H, Stirk L, Gummerson N. et al. EOS 2D/3D X-ray imaging system: a systematic review and economic evaluation. Health Technol Assess. 2012;16(14):1–188. doi: 10.3310/hta16140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation, Board on Radiation Effects Research, Division on Earth and Life Studies, National Research Council of the National Academies. Health risks from exposure to low levels of ionizing radiation: BEIR VII Phase 2. Washington, DC: The National Academies Press; 2006. URL: www.nap.edu/catalog.php?record_id= 11340 (accessed 27 October 2010).
- 9. United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). Sources and effects of ionizing radiation. UNSCEAR 2008 – report to the General Assembly with scientific annexes. Volume I. New York, NY: United Nations; 2010. URL: www.unscear.org/unscear/en/ publications/2008_1.html (accessed 27 October 2010).
- 10. International Commission on Radiological Protection (ICRP). . The 2007 recommendations of the International Commission on Radiological Protection ICRP publication 103. Ann ICRP. 2007;37:1–332. doi: 10.1016/j.icrp.2007.10.003. [DOI] [PubMed] [Google Scholar]
- 11.Kalifa G, Kalifa G, Charpak Y, Maccia C, Fery-Lemonnier E, Bloch J, Boussard JM. et al. Evaluation of a new low-dose digital x-ray device: first dosimetric and clinical results in children. Pediatr Radiol. 1998 Jul;28(7):557–61. doi: 10.1007/s002470050413. [DOI] [PubMed] [Google Scholar]
- 12. Haghighat Sh. The study of Cost-effectiveness of Breast Cancer Screening in Iranian Women, 2014, [PhD thesis].
- 13.Ajayi IR, Akinwumiju A. Measurement of Entrance Skin Doses to Patients in Four Common Diagnostic Examinations by Thermoluminescence Dosimetry in Nigeria. Radiat Prot Dosimetry. 2000;87(3):217–220. [Google Scholar]
- 14.Benameur S, Mignotte M, Labelle H, De Guise JA. A hierarchical statistical modeling approach for the unsupervised 3-d biplanar reconstruction of the scoliotic spine. IEEE Trans Biomed Eng. 2005 Dec;52(12):2041–57. doi: 10.1109/TBME.2005.857665. [DOI] [PubMed] [Google Scholar]
- 15.Kadoury S, Cheriet F, Laporte C, Labelle H. A versatile 3D reconstruction system of the spine and pelvis for clinical assessment of spinal deformities. Med Biol Eng Comput. 2007 Jun;45(6):591–602. doi: 10.1007/s11517-007-0182-1. [DOI] [PubMed] [Google Scholar]
- 16.Murphey MD, Quale JL, Martin NL, Bramble JM, Cook LT, Dwyer SJ 3rd. Computed radiography in musculoskeletal imaging: state of the art. AJR Am J Roentgenol. 1992 Jan;158(1):19–27. doi: 10.2214/ajr.158.1.1727344. [DOI] [PubMed] [Google Scholar]
- 17.Somoskeoy S, Tunyogi-Csapo M, Bogyo C. Accuracy and reliability of coronal and sagittal spinal curvature data based on patient-specific three-dimensional models created by the EOS 2D/3D imaging system. SPINE. 2012;12:1052–1059. doi: 10.1016/j.spinee.2012.10.002. [DOI] [PubMed] [Google Scholar]
- 18.Ilharreborde B, Steffen JS, Nectoux E, Vital JM, Mazda K, Skalli W. et al. Angle measurement reproducibility using EOS three-dimensional reconstructions in adolescent idiopathic scoliosis treated by posterior instrumentation. Spine (Phila Pa 1976) . 2011 Sep 15;36(20):E1306–13. doi: 10.1097/BRS.0b013e3182293548. [DOI] [PubMed] [Google Scholar]
- 19.Illés T, Tunyogi-Csapó M, Somoskeöy S. Breakthrough in three-dimensional scoliosis diagnosis: significance of horizontal plane view and vertebra vectors. Eur Spine J. 2011 Jan;20(1):135–43. doi: 10.1007/s00586-010-1566-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Glaser DA, Doan J, Newton PO. Comparison of 3-Dimensional Spinal Reconstruction Accuracy. SPINE. 2012;37:1391–1397. doi: 10.1097/BRS.0b013e3182518a15. [DOI] [PubMed] [Google Scholar]
- 21.Janssen MM, Drevelle X, Humbert L, Skalli W, Castelein RM. Differences in Male and Female Spino-Pelvic Alignment in Asymptomatic Young Adults A Three-Dimensional Analysis Using Upright Low-Dose Digital Biplanar X-rays. SPINE. 2009;34:E826–E832. doi: 10.1097/BRS.0b013e3181a9fd85. [DOI] [PubMed] [Google Scholar]
- 22.Azmy C, Guérard S, Bonnet X, Gabrielli F, Skalli W. EOS orthopaedic imaging system to study patellofemoral kinematics: Assessment of uncertainty. Orthopaedics & Traumatology: Surgery & Research. 2010;96:28–36. doi: 10.1016/j.rcot.2009.12.003. [DOI] [PubMed] [Google Scholar]
- 23.Journé A, Sadaka J, Bélicourt C, Sautet A. New method for measuring acetabular component positioning with EOS imaging: feasibility study on dry bone. International Orthopaedics (SICOT) 2012;36:2205–2209. doi: 10.1007/s00264-012-1650-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brosses ESS, Jolivet E, Travert C. Prediction of the Vertebral Strength Using a Finite Element Model Derived From Low-Dose Biplanar Imaging. SPINE. 2012;37:E156–E162. doi: 10.1097/BRS.0b013e3182293628. [DOI] [PubMed] [Google Scholar]
- 25.Rousseau MA, Laporte S, Chavary-Bernier E, Lazennec JY, Skalli W. Reproducibility of Measuring the Shape and Three-Dimensional Position of Cervical Vertebrae in Upright Position Using the EOS Stereoradiography System. SPINE. 2007;32:2569–2572. doi: 10.1097/BRS.0b013e318158cba2. [DOI] [PubMed] [Google Scholar]
- 26.Schlatterer B, Suedhoff I, Bonnet X, Catonne Y, Maestro M, Skalli W. Skeletal landmarks for TKR implantations: Evaluation of their accuracy using EOS imaging acquisition system. Orthopaedics & Traumatology Surgery & Research. 2009;95:2–11. doi: 10.1016/j.otsr.2008.05.001. [DOI] [PubMed] [Google Scholar]
- 27.Douglas TS, Vaughan CL, Wynne SM. Three-dimensional point Iocalisation in low-dose X-ray images using stereo-photogrammetry. Medical & Biological Engineering & Computing. 2004;42:37–43. doi: 10.1007/BF02351009. [DOI] [PubMed] [Google Scholar]
- 28.Gheno R, Nectoux E, Herbaux B, Baldisserotto M, Glock L, Cotten A. et al. Three-dimensional measurements of the lower extremity in children and adolescents using a low-dose biplanar X-ray device. EurRadiol. 2012:765–771. doi: 10.1007/s00330-011-2308-y. [DOI] [PubMed] [Google Scholar]
- 29.Sabourin M, Jolivet E, Miladi L, Wicart P, Rampal V, Skalli W. Three-dimensional stereoradiographic modeling of rib cage before and after spinal growing rod procedures in early-onset scoliosis. Clinical Biomechanics. 2010;25:284–291. doi: 10.1016/j.clinbiomech.2010.01.007. [DOI] [PubMed] [Google Scholar]
- 30.Dumas R, Aissaoui R. Personalized Body Segment Parameters From Biplanar Low-Dose Radiography. IEEE Transactions on Biomedical Engineering. 2005:52. doi: 10.1109/TBME.2005.855711. [DOI] [PubMed] [Google Scholar]
- 31.Dubousset J, Charpak G, Dorion I, Skalli W, Lavaste F, Deguise J. et al. A new 2D and 3D imaging approach to musculoskeletal physiology and pathology with low-dose radiation and the standing position: the EOS system. BullAcadNatl Med. 2005;189:287–300. [PubMed] [Google Scholar]
- 32.Illes T, Somoskeoy S. Principles of the EOS X-ray machine and its use in daily orthopedic practice] Orv Hetil. 2012 Feb 26;153(8):289–95. doi: 10.1556/OH.2012.29312. [DOI] [PubMed] [Google Scholar]
- 33.Illés T, Somoskeöy S. The EOS™ imaging system and its uses in daily orthopaedic practice. International Orthopaedics (SICOT) 2012;36:1325–1331. doi: 10.1007/s00264-012-1512-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Jerbi T, Burdin V, Leboucher J, Stindel E, Roux C. 2-D-3-D frequency registration using a low-dose radiographic system for knee motion estimation. IEEE Trans Biomed Eng. 2013 Mar;60(3):813–20. doi: 10.1109/TBME.2012.2188526. [DOI] [PubMed] [Google Scholar]
- 35.Wybier M, Bossard P. Musculoskeletal imaging in progress: The EOS imaging system. Joint Bone Spine. 2013 May;80(3):238–43. doi: 10.1016/j.jbspin.2012.09.018. [DOI] [PubMed] [Google Scholar]
- 36.Bourghli A, Guérin P, Vital JM, Aurouer N, Luc S, Gille O. et al. Posterior Spinal Fusion From T2 to the Sacrum for the Management of Major Deformities in Patients With Parkinson Disease. J Spinal Disord Tech. 2012 May;25(3):E53–60. doi: 10.1097/BSD.0b013e3182496670. [DOI] [PubMed] [Google Scholar]
- 37.Ohl X, Stanchina C, Billuart F, Skalli W. Shoulder bony landmarks location using the EOS low-dose stereoradiography system: a reproducibility study. SurgRadiol Anat. 2010 Feb;32(2):153–8. doi: 10.1007/s00276-009-0566-z. [DOI] [PubMed] [Google Scholar]
- 38.Morvan G, Mathieu P, Vuillemin V, Guerini H, Bossard P, Zeitoun F. et al. Standardized way for imaging of the sagittal spinal balance. Eur Spine J. 2011 Sep;20Suppl 5:602–8. doi: 10.1007/s00586-011-1927-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Lazennec JY, Rangel A. The eos imaging system for understanding a paellofemoral disorder following THR. Orthopaedics & Traumatology: OrthopTraumatolSurg Res. 2011 Feb;97(1):98–101. doi: 10.1016/j.otsr.2010.07.010. [DOI] [PubMed] [Google Scholar]
- 40.Guenoun B, Zadegan F. Reliability of a new method for lower- extremity measurements based on stereoradiographic three-dimensional reconstruction. OrthopTraumatolSurg Res. 2012 Sep;98(5):506–13. doi: 10.1016/j.otsr.2012.03.014. [DOI] [PubMed] [Google Scholar]
- 41.Douglas TS, Sanders V, Pitcher R. Early Detection of Fractures with Low-Dose Digital X-Ray Images in a Pediatric Trauma Unit. J Trauma. 2008 Jul;65(1):E4–7. doi: 10.1097/01.ta.0000198534.47134.bc. [DOI] [PubMed] [Google Scholar]
- 42.Illes T, Somoskeoy S. Comparison of scoliosis measurements based on three-dimensional vertebra vectors and conventional two-dimensional measurements: advantages in evaluation of prognosis and surgical results. Eur Spine J. 2013 Jun;22(6):1255–63. doi: 10.1007/s00586-012-2651-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. NHS, Diagnostics Assessment Programme EOS 2D/3D X-ray Imaging System.
- 44. NHS, the EOS 2D/3D imaging system.
- 45.Grignon B, Mainard L, Delion M, Hodez C, Oldrini G. Recent advances in medical imaging: anatomical and clinical applications. SurgRadiolAnat, SurgRadiol Anat. 2012 Oct;34(8):675–86. doi: 10.1007/s00276-012-0985-0. [DOI] [PubMed] [Google Scholar]
- 46.Bittersohl B, Freitas J, Zaps D, Schmitz MR, Bomar JD, Muhamad AR. et al. EOS Imaging of the Human Pelvis: Reliability, Validity, and Controlled Comparison with Radiography. J Bone Joint Surg Am. 2013 May 1;95(9):e581–9. doi: 10.2106/JBJS.K.01591. [DOI] [PubMed] [Google Scholar]
- 47.Lazennec JY, Rangel A, Baudoin A, Skalli W, Catonne Y, Rousseau MA. The eos imaging system for understanding a paellofemoral disorder following THR Orthopaedics & Traumatology: Surgery & Research. Orthop Traumatol Surg Res. 2011 Feb;97(1):98–101. doi: 10.1016/j.otsr.2010.07.010. [DOI] [PubMed] [Google Scholar]
- 48.lles T. Comparison of classical 2D measurement of scoliosis and 3D measurement using vertebral vectors: advantages for prognosis and treatment evaluation. Bull AcadNatl Med. 2011 Mar;195(3):629–42. discussion 642-3. [PubMed] [Google Scholar]