

Abstract
This rare case report presents the 2 nostrils 4 hands expanded endoscopic excision of the suprasellar dermoid through planum sphenoidale approach. This minimally invasive technique through the natural passage offers panaromic view of vital structures, complete excision of the lesion with reconstruction of the skull base defect at the same procedure.
Keywords: Endoscopic, Suprasellar, Ruptured dermoid, Surgery
Introduction
Intracranial dermoid cysts are rare benign lesions comprising 0.04–0.7 % of intracranial tumours. They are derived from ectopic epithelial cells that are part of the neural tube which explains their typical midline positions [1]. Rupture of intracranial dermoid cyst is a rare phenomenon 5 out of 2707 cases or 0.11 % of all new tumours operated [2]. We report a case of ruptured suprasellar dermoid cyst surgical excision through expanded endoscopic two nostrils—four hand technique without the aid of microscope.
Case Report
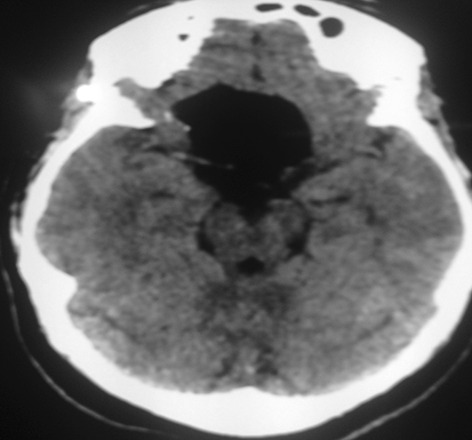
A 34 years female with history of headache for 10 days. She had a head injury before 6 months but did not have any complaints. ENT examination was normal. In the Neuro-opthalmology examination revealed bilateral florid papillodema. Patient is a known hypertensive on treatment and recently detected diabetic. The MRI scan of brain showed a 40 mm × 28 mm × 25 mm lesion well defined T1 and T2 heterogenous predominantely hyperintense extra axial mass lesion in suprasellar region encasing pituitary stalk and optic chiasma reported as ruptured dermoid cyst (Fig. 1). We approached the lesion by using the expanded endoscopic—two nostrils—four hands technique with closure of the skullbase defect in the same procedure without microscope. The main surgeon holding the endoscope and dissecting while the assistant surgeon removing the tumour with micro-forcep and clearing field of blood.
Fig. 1.

Pre operative MRI
The surgical steps details are given in box (1) and preoperative picture (Fig. 1).
Opening the sphenoid.
Drilling and opening Planum Sphenoid to expose the dura.
Aspiration of cyst contents.
Incising Dura.
Letting out cyst contents.
Widening the opening.
Removing cyst pearly white keratin with hair material (Fig. 2).
Clearing cyst from anterior cranial fossa, below optic chiasma.
Complete removal of remnants by flushing with saline.
Dural reconstruction with Fascia Lata.
Applying tissue seal and surgical for haemostasis.
Nasal packing.
Fig. 2.

Per operative picture
The specimen sent for HPE reported as attenuated squamous epithelial lining of cyst with eosionophilic keratin material and hair materials features consistent with dermoid cyst (Fig. 4). The post operative MRI shows the complete excision of the tumour (Fig. 3). The post operative period was uneventful with papillodema reverting to normal pressure.
Fig. 4.
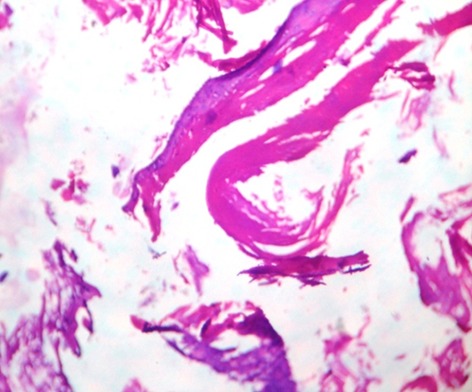
Attenuated Squamous epithelial lining of cyst with eosinophilic Keratinous material
Fig. 3.
Post operative picture
Discussion
Dermoid cysts are thick walled cysts lined by keratinized Squamous epithelium and supported by a well formed dermis containing skin appendages, usually hair and hair follicles, sebaceous and sweat gland, teeth or nails. All the ectodermal contents may or may not be present in a single patient. Intracranial Dermoid cysts are most commonly seen below the tentorium, either in the cavity of fourth ventricle or in the vermis, often associated with dermal sinus. Supra tentorial dermoid are less common and are located on the skullbase near the midline. Suprasellar and pineal gland are rare sites. Supratentorial dermoid appears in the 20–30 years age group, although the age presentation is variable. Following complete excision of dermoid the recurrence is rare contrary to epidermoid that are known to recur [3].
The four hand technique is an evolution described by May. Castelnuovo and Locatelli in 1997 started the treatment of sellar disease applying four hand technique, using access through both nostrils allowing two surgeons to work simultaneously to explore the central skullbase [4]. The endoscopic transnasal skull base approach is an excellent alternative to a traditional frontal craniotomy, to achieve removal of intra cranial dermoid cyst. The endoscope has been a useful tool for removing epidermoid tumors from the cavernous sinus and enhances visualisation of areas that would otherwise be difficult with microscopes alone. Endoscopes also help to minimise the retraction of neuro vascular structures. Fries and Perneczky described the advantages of the endoscopes as an adjunct tool in micro surgery including reduced surgical trauma, especially in a vascular lesions such as epidermoid tumor [5]. Expanded endonasal transsphenoidal approach has advantages of no incisions, faster recovery, early devascularisation of tumour, no brain retraction, minimal manipulation of optic apparatus, avoids craniotomy, less post operative discomfort and no loss of olfaction. The disadvantages are risk of CSF leak which can be sealed in the same surgery, meningitis and difficult to dissect tumour’s adherent/encased around small vessels [6]. Endoscope offers better intraoperative visualization due to the angled view. Finally it is a team work of Otorhino-laryngologist and Neuro-surgeons.
Conclusion
Transnasal endoscopic skull base surgery is a field that has experienced explosion of development over the past several years. The range of anatomic regions and pathology that can be addressed by endoscopic approaches is already impressive. When considering the approach to use, generally the approach that traverses the fewest neuro vascular structures to access the lesion will be the best approach. For the vast majority of midline skull base lesions the endoscopic two nostrils—four hands technique from below offers the best approach. The training of surgeon will enable them to perform extended approaches in anterior skull base, sella and suprasellar regions. It is noteworthy that this technique has fostered true interdiscipilinary improvement in the treatment of patients.
References
- 1.Kucera JN, Roy P, Murtagh R. Ruptured intracranial dermoid cyst manifesting as new onset seizure: a case report. J Radiol Case Rep. 2011;5(4):10–18. doi: 10.3941/jrcr.v5i4.592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Liu JK, Gottfried ON, Salzman KL, Schmidt RH, Couldwell WT. Ruptured intracranial dermoid cysts: clinical, radiographic, and surgical features. Neurosurgery. 2008;62(2):377–384. doi: 10.1227/01.neu.0000316004.88517.29. [DOI] [PubMed] [Google Scholar]
- 3.Venkatesh SK, Phadke RV, Trivedi P, Bannerji D. Asymptomatic spontaneous rupture of suprasellar dermoid cyst: a case report. Neurol India. 2002;50:480–483. [PubMed] [Google Scholar]
- 4.Castelnuovo P, Pistochini A, Locatelli D. Different surgical approaches to the sellar region: focusing on the “Two Nostrils Four Technique. Rhinology. 2006;44:2–7. [PubMed] [Google Scholar]
- 5.Chung JC, Kim SM, Sade B, Kim HK, Park MS, Chung SY, Park KS. Endoscope-assisted microsurgical removal of an epidermoid tumor within the cavernous sinus. Yonsei Med J. 2012;53(6):1216–1219. doi: 10.3349/ymj.2012.53.6.1216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hayhurst C, Teo C. Tuberculum sella meningioma. Otolaryngol Clin N Am. 2011;44:953–963. doi: 10.1016/j.otc.2011.06.012. [DOI] [PubMed] [Google Scholar]