

Abstract
Uterine didelphys with obstructed hemivagina and ipsilateral renal agenesis is a rare congenital anomaly of the Müllerian duct system referred to as Herlyn-Werner-Wunderlich syndrome. Because of its rare occurrence, a high level of suspicion is often required for diagnosis. Clinically, these patients usually present after menarche with pelvic pain, dysmenorrhea, and a palpable pelvic mass. We present a case of a 31-year-old female patient with infertility. Imaging findings were consistent with Herlyn-Werner-Wunderlich syndrome, with a congenital defect in the longitudinal vaginal septum resulting in partial spontaneous decompression of right-sided hematocolpos.
Case report
A 31-year-old female presented with 18 months of primary infertility. Her menstrual cycles were regular. She had no history of dysmenorrhea, pelvic mass, or pelvic pain. A bimanual pelvic examination yielded a normal-size uterus that was mobile and nontender, without palpable pelvic masses. A speculum examination demonstrated a nulliparous cervix without lesions.
The patient reported that a prior evaluation elsewhere had indicated a septate uterus or uterine didelphys. Magnetic resonance imaging (MRI) of the pelvis (to evaluate the possible Mullerian anomaly) was performed on a 1.5-Tesla MR scanner (Achieva, Philips Medical Systems). An intravenous contrast agent was not considered necessary. Images were acquired on multiple planes with oblique axial T1 (TR 608 ms; TE 10 ms), oblique coronal T2 (TR 3733 ms; TE 120 ms), oblique axial T2 (TR 3172 ms; TE 120 ms), sagittal T2 (TR 8276 ms; TE 120 ms), and coronal T2 SPAIR (TR 761 ms; TE 120 ms) sequences.
MR images showed two uterine horns that were completely separate and widely splayed. They appeared fully developed and almost normal in size, with preserved endometrial, myometrial, and junctional zones. Two individual cervices were in continuity with the uterine horns (Fig. 1). A longitudinal vaginal septum divided the upper vagina into two cavities, with one cervix entering each hemivagina. A defect in the proximal end of the vaginal septum allowed direct communication between the two hemivaginas (Fig. 2). The right hemivagina was moderately distended and contained blood products that were T2-hyperintense and mildly T1-hyperintense, consistent with hematocolpos. The right hemivagina terminated blindly approximately 4 cm cranial to the introitus. The left hemivagina was decompressed (Fig. 2). A single lower vaginal cavity likely communicated with the left hemivagina, the left cervix, and the left uterine horn. Coronal images through the midabdomen demonstrated an empty right renal fossa and a normal left kidney (Fig. 3). These imaging features were diagnostic of HWW syndrome with a congenital defect in the longitudinal vaginal septum, resulting in partial spontaneous decompression of the right hemivagina.
Figures 1.
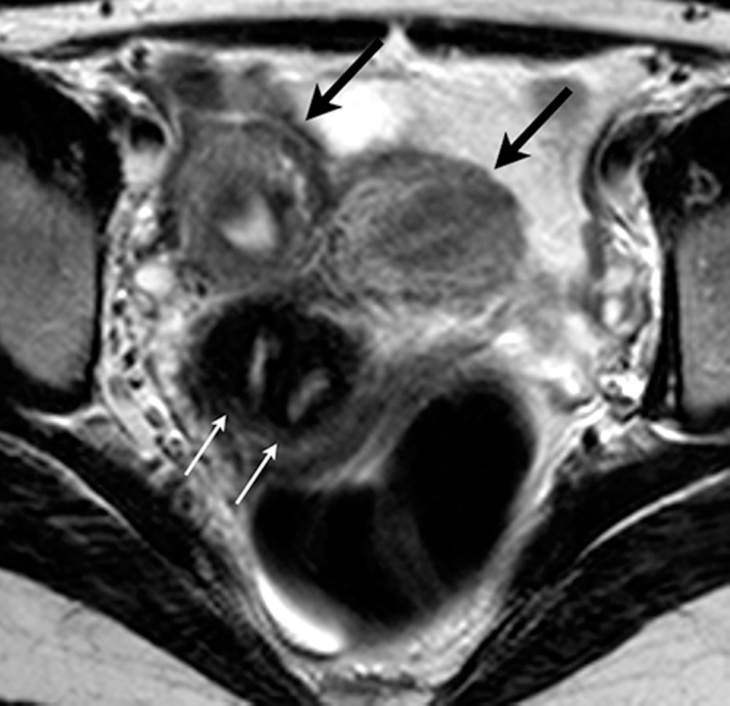
31-year-old female with Herlyn-Werner-Wunderlich syndrome. T2-weighted axial MR image through the pelvis demonstrated two uterine horns (black arrows) and two individual cervices (white arrows). The uterine horns were almost of normal size, completely separate, and widely splayed.
Figure 2.
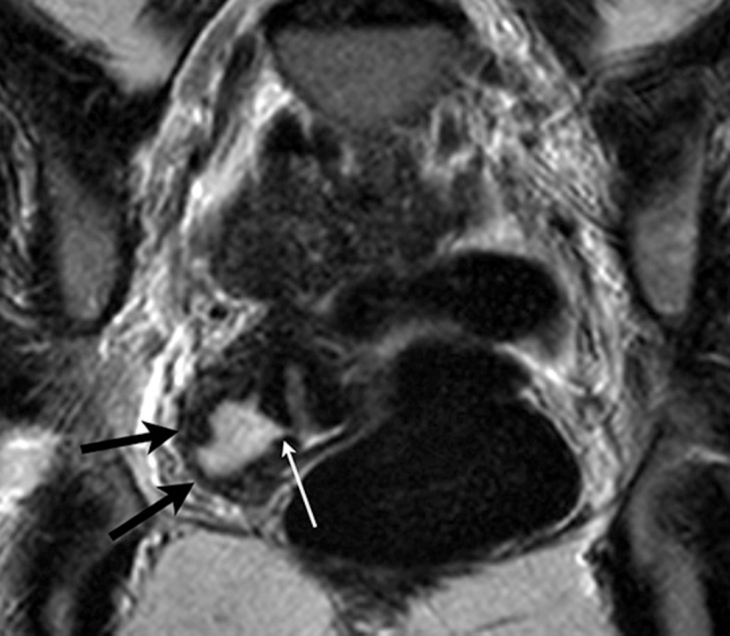
31-year-old female with Herlyn-Werner-Wunderlich syndrome. T2-weighted coronal oblique MR image through the pelvis demonstrated a moderately distended right hemivagina (black arrows) and a defect in the proximal end of the vaginal septum (white arrow) that allowed direct communication between the two hemivaginas.
Figure 3.

31-year-old female with Herlyn-Werner-Wunderlich syndrome. T2-weighted coronal MR image through the mid-abdomen demonstrated an empty right renal fossa (thin white arrow) and a normal left kidney (thick white arrow).
Discussion
Herlyn-Werner-Wunderlich (HWW) syndrome is a congenital anomaly of the Müllerian and Wolffian ducts (1) characterized by a triad of uterus didelphys, obstructed hemivagina, and ipsilateral renal agenesis (2, 3, 4, 5). The diagnosis is usually made soon after menarche due to symptoms related to the obstructed hemivagina, such as pelvic pain, dysmenorrhea, and palpable mass from associated hematocolpos or hematometra.
An obstructed hemivagina with a didelphic uterus is the most common type of obstructing malformation of the uterus and vagina (6). The longitudinal vaginal septum is due to incomplete disappearance of the partition between the fused Müllerian ducts (7). As an obstructing vaginal malformation, this condition precludes the outflow of menstruation, resulting in hematocolpos, possible hematometra, and hematosalpinx. The diagnosis is therefore usually made soon after menarche due to symptoms related to the obstructed hemivagina, such as pelvic pain, dysmenorrhea, and a palpable pelvic mass. Long-term complications of HWW syndrome include endometriosis from retrograde menstruation, and obstetric complications such as recurrent pregnancy loss, preterm labor, abnormal fetal presentation, and prematurity due to uterine anomalies (8, 9, 10).
Our patient presented with primary infertility and had a congenital defect in the longitudinal vaginal septum, resulting in partial spontaneous decompression of right-sided hematocolpos. As illustrated by this case report, patients with HWW syndrome may have a defect in the longitudinal vaginal septum that allows spontaneous decompression of the obstructed hemivagina into the nonobstructed hemivagina. Such patients are likely to present with fewer obstructive symptoms than in those with an intact longitudinal vaginal septum and complete obstruction of the hemivagina. Although some amount of hematocolpos and/or hematometra may be present at diagnosis, we assume that the volume may not be sufficient to cause obstructive symptoms. This would explain the delay in presentation as in the case presented. We also postulate that patients with a defect in the longitudinal vaginal septum may be protected from retrograde menstruation and subsequent development of pelvic endometriosis, since the hemivagina is partially decompressed via the defect.
To our knowledge, this is the only reported case where a defect in the septum has resulted in decompression of the obstructed vagina. MRI has been shown to be the gold standard in imaging of Müllerian anomalies (11), and we consider it the imaging modality of choice for illustration of defects in the longitudinal vaginal septum.
Footnotes
Published: December 21, 2012
References
- 1.Candiani GB, Fedele L, Candiani M. Double uterus, blind hemivagina, and ipsilateral renal agenesis: 36 cases and long-term follow-up. Obstet Gynecol. 1997;90:26–32. doi: 10.1016/S0029-7844(97)83836-7. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Gholoum S, Puligandla PS, Hui T, Su W, Quiros E, Laberge JM. Management and outcome of patients with combined vaginal septum, bifid uterus, and ipsilateral renal agenesis (Herlyn-Werner-Wunderlich syndrome) J Pediatr Surg. 2006;41:987–992. doi: 10.1016/j.jpedsurg.2006.01.021. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Sarac A, Demir MK. Herlyn-Werner-Wunderlich syndrome: a rare cause of infertility (2009: 2b) Eur Radiol. 2009;19:1306–1308. doi: 10.1007/s00330-008-1085-8. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Orazi C, Luchetti MC, Schingo PM, Marchetti P, Ferro F. Herlyn-Werner-Wunderlich syndrome: uterus didelphys, blind hemivagina and ipsilateral renal agenesis. Sonographic and MR findings in 11 cases. Pediatr Radiol. 2007;37:657–665. doi: 10.1007/s00247-007-0497-y. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Rana R, Pasrija S, Puri M. Herlyn-Werner-Wunderlich syndrome with pregnancy: a rare presentation. Congenit Anom (Kyoto) 2008;48:142–143. doi: 10.1111/j.1741-4520.2008.00195.x. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Pinsonneault O, Goldstein DP. Obstructing malformations of the uterus and vagina. Fertil Steril. 1985;44:241–247. [PubMed] [PubMed] [Google Scholar]
- 7.Crosby WM, Hill EC. Embryology of the Mullerian duct syytem. Review of present-day theory. Obstet Gynecol. 1962;20:507–515. [PubMed] [PubMed] [Google Scholar]
- 8.Rock JA, Jones HW., Jr. The double uterus associated with an obstructed hemivagina and ipsilateral renal agenesis. Am J Obstet Gynecol. 1980;138:339–342. doi: 10.1016/0002-9378(80)90260-4. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.Heinonen PK. Clinical implications of the didelphic uterus: long-term follow-up of 49 cases. Eur J Obstet Gynecol Reprod Biol. 2000;91:183–190. doi: 10.1016/s0301-2115(99)00259-6. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Rock JA, Schlaff WD. The obstetric consequences of uterovaginal anomalies. Fertil Steril. 1985;43:681–692. doi: 10.1016/s0015-0282(16)48548-1. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.Burgis J. Obstructive Mullerian anomalies: case report, diagnosis, and management. Am J Obstet Gynecol. 2001;185:338–344. doi: 10.1067/mob.2001.116738. [PubMed] [DOI] [PubMed] [Google Scholar]