

Abstract
The purpose of this study was to determine whether the excursion of the scaphoid tuberosity and therefore scaphoid motion are minimized during a dart-throwing motion. Scaphoid tuberosity excursion was studied as an indicator of scaphoid motion in 29 cadaver wrists as they were moved through wrist flexion-extension, radioulnar deviation and a dart-throwing motion. Study results demonstrate that excursion was significantly less during the dart-throwing motion than during either wrist flexion-extension or radioulnar deviation. If the goal of early wrist motion after carpal ligament or distal radius injury and reconstruction is to minimize loading of the healing structures, a wrist motion in which scaphoid motion is minimal should reduce length changes in associated ligamentous structures. Therefore, during rehabilitation, if a patient uses a dart-throwing motion that minimizes their scaphoid tuberosity excursion, there should be minimal changes in ligament loading while still allowing wrist motion.
Study Design
Bench research – biomechanics – cross-sectional
Level of evidence
N/A since this was a lab based study
Keywords: Dart-throwing motion, scaphoid tuberosity
Introduction
Optimal post-surgical treatment of scapholunate interosseous ligament (SLIL) tears and distal radius fractures should stabilize a tear or fracture site while still allowing for early wrist motion. Most published studies discuss methods to detect, grade or repair injuries1, 2 and do not emphasize rehabilitation methods. A rehabilitation method suggested by Moritomo et al,3 advocates that patients utilize a dart-throwing pattern of motion following surgery.
Previous studies4-6 have shown that scaphoid motion is minimized during a dart-throwing motion as compared to wrist flexion-extension or radioulnar deviation. This would suggest that a dart-throwing type of motion might reduce the ligament forces on a repair or fracture while still allowing wrist motion. However, the patient-specific dart-throwing orientation that minimizes carpal motion varies between subjects.6 The purpose of this study is to assess a method that might eventually help determine a patient-specific dart-throwing motion that minimizes scaphoid tuberosity excursion. A second purpose was to determine if there is an association between scaphoid tuberosity excursion and scapholunate interosseous ligament length changes during wrist motion.
The first hypothesis of this study is that excursion of the scaphoid tuberosity is minimized during a dart-throwing motion compared to a wrist flexion-extension or radioulnar deviation motion. The second hypothesis is that a specific orientation of a dart-throwing motion will reduce scaphoid tuberosity motion more than other orientations. In this study it is assumed that a wrist motion with less tuberosity movement will have less scaphoid motion, with less associated dorsal and volar SLIL elongation, which, in turn, will reduce loading on a scaphoid or distal radius fracture. If excursion of the tuberosity is clinically measured by direct palpation, one could determine the dart-throwing motion orientation during which the tuberosity excursion is minimal. If a patient can be trained or guided to use this wrist motion, scaphoid motion would be reduced and thus presumably allow for early range of motion exercise of the wrist when minimal carpal motion and SLIL length change is desired.
Purpose of study
The purpose of this study was to determine whether the excursion of the scaphoid tuberosity is minimized during a dart-throwing motion.
Methods
Cadaver Wrist Motion
Analyses involved scaphoid and lunate kinematic data from 29 (average 67.8 years, range 29 to 98; 14 female, 15 male) cadaver wrists. Each wrist had been previously cyclically moved through flexion-extension, radioulnar deviation and dart-throwing motions using a wrist joint motion simulator7 while intact6 and after various ligament sectioning sequences.8-11 In this study, analyses included only the data from scaphoid and lunate motions while all ligaments were intact were analyzed.
During the wrist flexion-extension motion the wrist moved from 50 degrees of flexion to 30 degrees of extension and back to 50 degrees of flexion repetitively for six cycles. During the radioulnar deviation motion the wrist moved from 20 degrees of ulnar deviation to 10 degrees of radial deviation and back to 20 degrees of ulnar deviation repetitively for six cycles. During the dart-throwing motion the wrist moved from 30 degrees of extension and 10 degrees of radial deviation to 30 degrees of flexion and 10 degrees of ulnar deviation and back to extension and radial deviation repetitively six times. The limits of 50 degrees flexion, 20 degrees of ulnar deviation and 10 degrees of radial deviation were selected based on previous testing that identified some wrist motion limitations at the end ranges of motion. Study requirements necessitated that all wrists achieve the same endpoints of motion. The limit of 30 degrees of extension was selected to prevent the lunate sensor post (described later) from hitting the dorsal rim of the radius.
Six of these wrists had also been moved using a wrist simulator through 9 different orientations of a dart-throwing motion while all ligaments were intact.6 Data collection involved recording scaphoid motion during each of the 9 movements: a pure flexion-extension motion from 30 degrees of flexion to 30 degrees of extension and a pure radioulnar deviation motion from 20 degrees of ulnar deviation to 10 degrees of radial deviation and 7 addition motions (figure 1) reflecting variations of a dart-throwing motion from extension and radial deviation to flexion and ulnar deviation. These selected motions were chosen to address most possible variations of a dart-throwing motion.
Figure 1.

Nine dart-throwing wrist motions studied as viewed in the transverse plane. Motion A is a pure extension to flexion motion. Motion I is a pure radial deviation to ulnar deviation. The other 7 motions were as the wrist moved from extension and radial deviation to flexion and ulnar deviation. The length of each line corresponds to the excursion of the motion. (Reprinted with permission from Werner et al. Scaphoid and Lunate Motion During a Wrist Dart Throw Motion, J Hand Surg 29A;2004;419).
Wrist Simulator Testing
All of these arms were tested in a wrist simulator (figure 2) in which the dynamic cyclic wrist motions were caused by physiological forces being applied under computer control to five wrist flexor and extensor tendons.6 Each tendon was connected in series with a load cell which was connected to its own hydraulic actuator. Motion of the third metacarpal, assumed to be the same as wrist motion, was measured by an electromagnetic motion sensor (Polhemus, Colchester, VT) and was used as feedback to the algorithm controlling the simulator to actively control the tendon loading and thus actively cause the wrist motion. During a planar motion such as wrist flexion-extension, the out of plane motion (e.g. radioulnar deviation during wrist flexion-extension) was less than 1 degree. The motions of the scaphoid, lunate, and distal radius were similarly measured by using electromagnetic motion sensors mounted onto plastic platforms which were glued onto composite posts that were cemented into the scaphoid and the lunate or connected directly to the radius. The radial sensor became the local coordinate system and was aligned with the anatomical directions (proximal-distal; radial-ulnar and dorsal-volar). The translations and the angular motions of the scaphoid and lunate were thus transformed to the distal radius. The accuracy of these sensors was previously reported to be 0.2 degrees and 0.2 mm.12
Figure 2.

Wrist joint motion simulator used to test each wrist. Motion of the third metacarpal and therefore the wrist was measured by an electromagnetic sensor mounted on the third metacarpal. Motion of the scaphoid (and lunate) were measured by sensors attached to posts cemented into each bone. These motions were referenced to the sensor mounted on the distal radius. Wrist motion was caused by actuators connected in series with clamps attached to the wrist flexors and extensors.
Wrist Imaging
At the end of each experiment, a CT scan was taken of the carpal bones, distal radius and ulna and the scaphoid and lunate motion sensors, to obtain 1.0 mm axial slices (voxel size of 0.33-0.54 mm2 by 1 mm). Using the methodology of Green et al13 the data from the CT scans were used to create 3D models of each bone. As described by Green et al, SliceOmatic Imaging Software (Tomovision, Montreal, Canada) was used to create surface shells of each bone or object from the CT slices and 3DStudio Max animation software (Autodesk, Inc., San Rafael, CA) was used to animate each bone or object. The models were animated by combining the recorded kinematic data of the sensor with the surface model of each bone to move the scaphoid and lunate through each of the wrist motions. The overall error of this method was reported by Green et al to be 0.2 mm when computing minimum distances between the scaphoid and lunate during similar wrist motions. Since the motion of the carpal bones were computed relative to the radius, CT scan based models made of each radius and ulna had no motion and could be included in the figures.
For each of the 29 wrists, the scaphoid tuberosity was identified in the animation. The 3D movement of the scaphoid tuberosity (figure 3) relative to a neutral wrist flexion-extension starting position was then computed at each of the 273 frames of one cycle of each animation. The 273 frames of motion were based on each cycle of motion taking 10 seconds and the motion of the scaphoid and lunate sensors being recorded at 27.3 Hz. The movement of the scaphoid tuberosity was computed by first locating its 3D location relative to the scaphoid sensor and then applying to it the kinematic transformation defining the scaphoid sensor location at each increment of wrist motion relative to the radial sensor. This allowed us to determine the overall 3D excursion (movement) of the scaphoid tuberosity and thus determine the peak excursion during each wrist motion as well as its distal-proximal, dorsal-volar and radioulnar displacements components. Since the methods used were similar to those used by Green et al to compute the minimum distance between the scaphoid and lunate, a comparable error of 0.2 mm would be expected here. In the animation of the scaphoid and lunate in 28 of the wrists, single points, representing the insertions and attachments of the dorsal and volar components (figure 4) of the scapholunate interosseous ligament (SLIL) were identified and tracked during each wrist motion using the same methods (with the same potential error) developed to track the excursion of the scaphoid tuberosity. The length of the dorsal and volar components of the SLIL was then computed as the distance between these points throughout each wrist motion and for each arm.
Figure 3.

Excursion of the scaphoid tuberosity movement during a flexion-extension motion is shown by a series of red spheres during the wrist motion. Scaphoid (blue) and lunate (green) are located with wrist in extension.
Figure 4.

Dorsal and volar scaphoid lunate interosseous ligament (SLIL) components for a right wrist in extension.
Data Analysis
Differences in scaphoid excursion and ligament length were statistically analyzed using repeated measures ANOVAs using P<0.05 as our level of significance. Post-hoc tests were performed using a Bonferroni correction for multiple comparisons. Using a linear model assumption, a linear regression was performed to determine associations between tuberosity excursion and SLIL length.
Results
Examination of the data from the 28 wrists, identified that the 3D excursion of the scaphoid tuberosity (table 1, figure 5) was significantly less during the dart-throwing motion than during either the flexion-extension motion (p<0.001) or the radioulnar deviation motion (p<0.001). The distal-proximal component of the overall excursion of the scaphoid tuberosity was significantly greater than either the radioulnar (p<0.001) or dorsal-volar (p<0.001) excursions (table 2).
Table 1.
Average SLIL length at the endpoint of motion relative to the neutral wrist position and average scaphoid tuberosity excursion (standard deviation). The scaphoid tuberosity excursions are the average of the maximum excursions during a cycle of motion for the 28 arms. The largest displacement may not occur at the same angle in each arm.
| Wrist Position | Scaphoid Tuberosity Excursion (mm) | Dorsal SLIL Length (mm) | Volar SLIL Length (mm) |
|---|---|---|---|
| Flexion-Extension at Maximum Flexion | 6.9 (2.5) | 6.9 (2.6) | 8.6 (2.6) |
| Radioulnar Deviation at Maximum Ulnar Deviation | 8.1 (2.7) | 6.1 (2.0) | 8.2 (2.6) |
| Dart Throw Motion at Maximum Ulnar Flexion | 3.8 (1.6) | 6.6 (4.0) | 8.2 (2.1) |
Figure 5.

Absolute Magnitude of 3D Scaphoid Tuberosity Excursion During One Cycle of Flexion-Extension, Radioulnar Motion and Dart-Throwing Motions. The peak values, here in figure 5, are not the same as the peak values given in table 1, since these values are the average for all 28 arms, averaged at each degree of wrist motion. The table 1 values are the average of the largest values during each cycle for the 28 arms.
Table 2. Total tuberosity excursion in 3 orthogonal directions based on 28 arms.
| Wrist Motion | Radioulnar Component (mm, std dev) | Dorsal-Volar Component (mm, std dev) | Distal-Proximal Component (mm, std dev) |
|---|---|---|---|
| Flexion-extension | 2.8 (1.3) | 4.0 (2.0) | 9.3 (3.8) |
| Radioulnar Deviation | 3.5 (2.0) | 3.4 (2.1) | 9.4 (3.2) |
| Dart Throwing Motion | 2.3 (1.1) | 2.4 (1.3) | 4.2 (2.6) |
There was a strong association (r2 = 0.73 for the volar SLIL component, r2 = 0.62 for the dorsal SLIL) between increasing scaphoid tuberosity excursion and increasing SLIL length (figure 6) during the flexion-extension motion. During the radioulnar deviation motion there was an association (r2 = 0.65 for the volar SLIL component, r2 = 0.66 for the dorsal SLIL) between increasing scaphoid tuberosity excursion and increasing SLIL length (figure 7). During the dart-throwing motion there was an association (r2 = 0.68 for the volar SLIL component, r2 = 0.64 for the dorsal SLIL) between increasing scaphoid tuberosity excursion and increasing SLIL length (figure 8).
Figure 6.
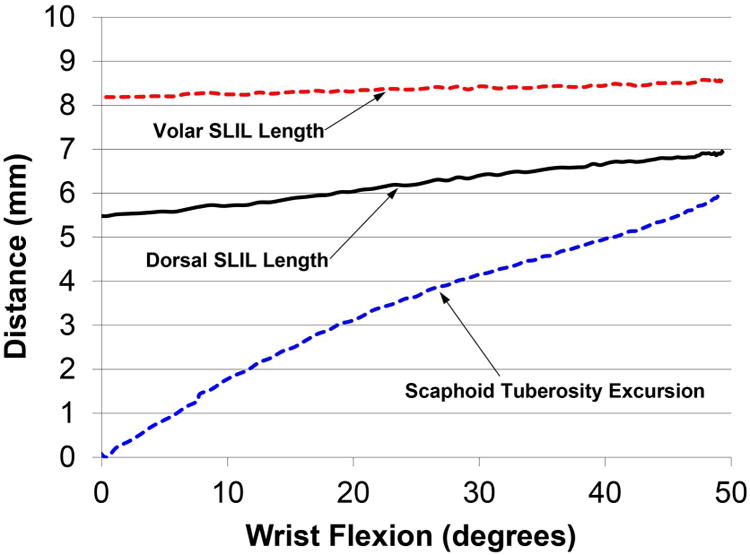
Scaphoid Tuberosity Excursion from the Neutral Reference Position and Length of Dorsal and Volar Components of the SLIL as a Function of Wrist Flexion Angle (Average of 28 Arms during Flexion-Extension Motion)
Figure 7.

Scaphoid Tuberosity Excursion from the Neutral Reference Position and Length of Dorsal and Volar Components of the SLIL as a Function of Wrist Ulnar Deviation Angle (Average of 28 Arms during Radioulnar Deviation Motion)
Figure 8.

Scaphoid Tuberosity Excursion from the Neutral Reference Position and Length of Dorsal and Volar Components of the SLIL as a Function of Wrist Flexion Angle (Average of 28 Arms during Dart-Throwing Motion)
In the part of the study with six arms examining 9 different dart-throwing motions, there was a strong association (r2 = 0.96; figure 9) between the relative motion of the scaphoid to the 3rd metacarpal and scaphoid tuberosity excursion. The total scaphoid tuberosity excursion was the smallest in those motions during which the scaphoid moved least relative to the 3rd metacarpal (motions E, F and G; table 3).
Figure 9.
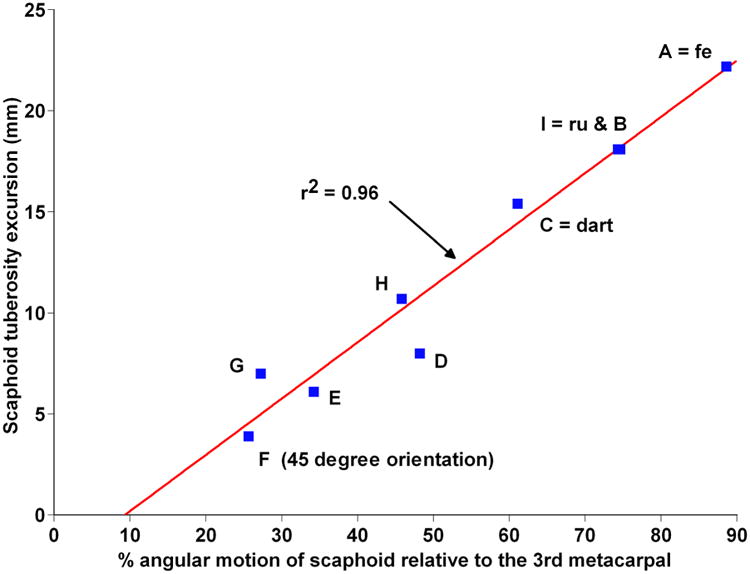
Relative Excursion of Scaphoid Tuberosity for the 6 arms undergoing 9 different dart-throwing motions compared to the amount of Scaphoid motion. Here scaphoid motion is expressed as a percentage of the third metacarpal motion which by definition is the same as wrist motion. (Tuberosity excursion is amplified due here to using an ulnar coordinate based system instead of the radial coordinate system). “fe” is the planar flexion-extension motion. “ru” is the planar radioulnar deviation motion. “dart” is the same dart throw motion used in the base data set of 28 arms. The letters A, B, etc. refer to the different dart-throwing motions shown in figure 1.
Table 3. Amount of Scaphoid Tuberosity Excursion for Different Dart-Throwing Motions.
| Amount of wrist flexion-extension and radioulnar deviation during each Dart-Throwing Motion | Corresponding letter of motion in figure 1 | Scaphoid Tuberosity Excursion (Percent of pure flexion-extension motion; motion A) | |
|---|---|---|---|
| Total amount of Flexion-extension (degrees) | Total amount of Radioulnar Deviation (degrees) | ||
| 60 | 0 | A (pure flexion-extension) | 100 |
| 60 | 10 | B | 82 |
| 60 | 20 | C | 69 |
| 40 | 20 | D | 36 |
| 40 | 30 | E | 27 |
| 30 | 30 | F | 18 |
| 20 | 30 | G | 32 |
| 10 | 30 | H | 48 |
| 0 | 30 | I (pure radioulnar deviation) | 82 |
Discussion
The primary purpose of this study was to evaluate scaphoid tuberosity excursion during different wrist motions and determine which dart-throwing orientation results in the least amount of excursion. Our assumption is that a wrist motion with less tuberosity movement will have less scaphoid motion, with associated less dorsal and volar SLIL elongation, which in turn will reduce loading on a scaphoid or distal radius fracture. These results demonstrate that scaphoid tuberosity excursion is minimized during a dart-throwing motion when compared to wrist flexion-extension or radioulnar deviation. Although studies4-6 have previously demonstrated that a dart-throwing motion minimizes scaphoid motion, these results could serve as a basis to clinically assess scaphoid tuberosity excursion and could help determine which type of a dart-throwing motion is optimal during rehabilitation. These results support the work by Braidotti et al14 who developed an orthosis based on patient specific anatomical landmarks (radio-palmar aspect of the scaphoid tuberosity and the ulno-dorsal aspect of the hamate) to guide the patient through a dart-throwing motion. The current study supports the use of their selection of the scaphoid tuberosity.
Upal et al,15 in an in vivo study observed that the elongation of the palmar and dorsal SLIL was minimal during a wrist dart-throwing motion as compared to other motions. In their study, they also showed that a different dart-throwing orientation minimized the palmar SLIL elongation as compared to the dorsal SLIL. Palmar SLIL elongation was minimized during a dart-throwing motion that included more radioulnar deviation than the orientation when the dorsal SLIL elongation was minimized. The results of this study supports their findings and provides additional evidence in associating scaphoid tuberosity excursion with scaphoid motion. The patient-specific dart-throwing motion orientation that minimizes scaphoid excursion and motion may vary slightly among patients. The results from this study support the second hypothesis that one dart-throwing motion orientation (specifically a motion approximately 45 degrees from the sagittal plane) requires less scaphoid tuberosity motion than other dart-throwing orientations. Determination of the patient-specific orientation which minimizes scaphoid tuberosity motion should also result in minimal scaphoid motion.
This study is limited in that these motions were measured in cadaver specimens. However by moving each cadaver wrist with this simulator, its motion could be carefully and repeatedly controlled, which allowed us to make clear distinctions between slightly different dart-throwing motion orientations. For example, on average, a dart-throwing motion oriented 45 degrees from the flexion-extension plane (motion F in figure 1) had the smallest scaphoid tuberosity excursion (figure 9, table 3) followed closely by dart-throwing motions (motions E and G) oriented slightly away from the motion oriented 45 degrees from the flexion-extension plane. During motion F, when the dart-throwing motion was 45 degrees from the flexion-extension plane, the scaphoid tuberosity excursion was only 18% of that during the pure flexion-extension motion. Another limitation is that the elongations of the dorsal and palmar SLIL were based on single point insertion sites on the scaphoid and lunate while in fact they attach over a broad surface of each bone. While this study, based on three dimensional modeling, shows that a specific dart-throwing motion may minimize scaphoid motion, it did not evaluate the reliability of clinically finding the optimal motion. Clinical determination of that motion may be achieved by palpating the scaphoid tuberosity during wrist motion. In an uninjured wrist, one can locate the tuberosity in a neutral wrist position (figure 10A, 10B) and with radial deviation (figure 10C) confirm its location as it moves palmarly and with ulnar deviation (figure 10D) notice how it moves dorsally. Variations of a dart-throwing motion from radial extension (figure 10E) to ulnar flexion (figure 10F) can be adjusted until the tuberosity position is in nearly the same position as in the neutral wrist position. Although not addressed by this study, once that motion is found a patient might be educated to use this best dart-throwing motion. Possibly a brace similar to that developed by Braidotti et al14 could be used initially to train a patient and continued to be used until healing has occurred. Lastly, this study does not address how to determine this ideal dart-throwing motion in a patient with injured or healing structures. These structures would be at increased risk during any motions used to determine this ideal motion but the possibility of identifying this motion using the contralateral uninjured wrist may warrant further study.
Figure 10.
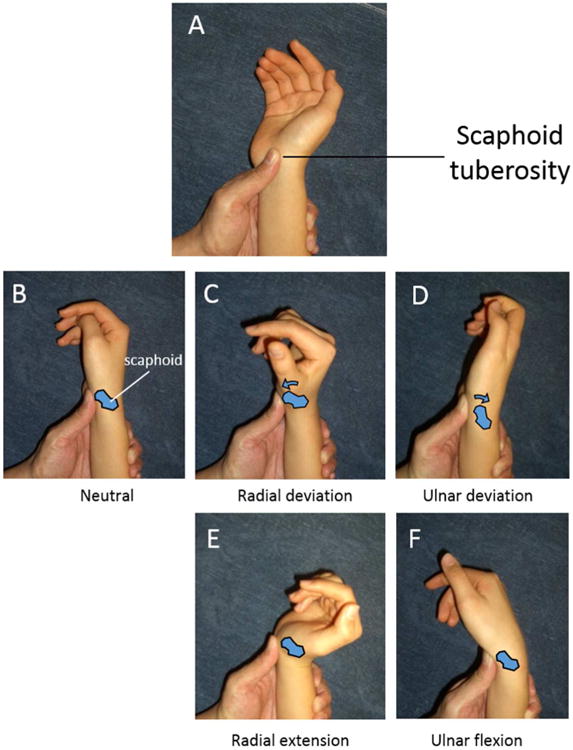
Suggested method on how to clinically palpate the scaphoid tuberosity in an uninjured wrist. The scaphoid tuberosity of a patient be can located with the wrist in a neutral position (A, B). When the patient's wrist is moved into radial deviation (C), the tuberosity will protrude palmarly and push against the thumb of the examiner. When the wrist is moved into ulnar deviation (D), the tuberosity will move dorsally. If the wrist is moved into the radial extended position (E), or into the ulnar flexed position (F), the tuberosity will be in nearly the same position as the neutral wrist. The positions of radial extension and ulnar flexion may need to be slightly varied until the tuberosity motion is minimized.
Conclusion
This study demonstrates that excursion of the scaphoid tuberosity is associated with scaphoid motion. It further shows that both parameters can be minimized during a patient-specific dart-throwing orientation. These results support the benefit of clinically palpating a patient's scaphoid tuberosity during a patient's wrist motion to determine which dart-throwing motion minimizes the tuberosity excursion and thus minimizes scaphoid motion. Determination of the optimal dart-throwing orientation should minimize loading of a SLIL repair or a distal radius fracture. These findings may influence rehabilitation practice guidelines after these injuries.
Optimal wrist motion with least ligament loading is desired during rehabilitation.
Dart throw motion with minimal scaphoid tuberosity motion minimizes ligament loading.
Determine optimal dart throw motion by minimizing scaphoid tuberosity motion.
Acknowledgments
Funded in part by NIH AR5009. NIH had no role in the design, collection, analysis or interpretation of the data, in the writing of the manuscript, or in the decision to submit this manuscript for publication.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Work performed at: SUNY Upstate Medical University
Contributor Information
Levi G. Sutton, Email: levigsutton@gmail.com.
Walter H. Short, Email: wshort@twcny.rr.com.
Hisao Moritomo, Email: moritomo@tcct.zaq.ne.jp.
Hugo St-Amand, Email: hugo.stamand@gmail.com.
References
- 1.Kuo CE, Wolfe SW. Scapholunate instability: current concepts in diagnosis and management. J Hand Surg - Am. 2008;33:998–1013. doi: 10.1016/j.jhsa.2008.04.027. [DOI] [PubMed] [Google Scholar]
- 2.Werner FW, Wang H, Short WH, Sutton LG, Rosenbaum PF. Identifying scapholunate ligamentous injury. J Orthop Res. 2009;27:394–399. doi: 10.1002/jor.20749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Moritomo H, Apergis EP, Herzberg G, Werner FW, Wolfe SW, Garcia-Elias M. 2007 IFSSH committee report of wrist biomechanics committee: biomechanics of the so-called dart-throwing motion of the wrist. J Hand Surg - Am. 2007;32:1447–1453. doi: 10.1016/j.jhsa.2007.08.014. [DOI] [PubMed] [Google Scholar]
- 4.Crisco JJ, Coburn JC, Moore DC, Akelman E, Weiss AP, Wolfe SW. In vivo radiocarpal kinematics and the dart thrower's motion. J Bone Joint Surg - Am. 2005;87:2729–2740. doi: 10.2106/JBJS.D.03058. [DOI] [PubMed] [Google Scholar]
- 5.Ishikawa J, Cooney WP, 3rd, Niebur G, An KN, Minami A, Kaneda K. The effects of wrist distraction on carpal kinematics. J Hand Surg - Am. 1999;24:113–120. doi: 10.1016/S0266-7681(99)90057-8. [DOI] [PubMed] [Google Scholar]
- 6.Werner FW, Green JK, Short WH, Masaoka S. Scaphoid and lunate motion during a wrist dart throw motion. J Hand Surg - Am. 2004;29:418–422. doi: 10.1016/j.jhsa.2004.01.018. [DOI] [PubMed] [Google Scholar]
- 7.Werner FW, Palmer AK, Somerset JH, et al. Wrist joint motion simulator. J Orthop Res. 1996;14:639–646. doi: 10.1002/jor.1100140420. [DOI] [PubMed] [Google Scholar]
- 8.Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J Hand Surg - Am. 2005;30:24–34. doi: 10.1016/j.jhsa.2004.09.015. [DOI] [PubMed] [Google Scholar]
- 9.Short WH, Werner FW, Green JK, Sutton LG, Brutus JP. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part III. J Hand Surg - Am. 2007;32:297–309. doi: 10.1016/j.jhsa.2006.10.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Short WH, Werner FW, Sutton LG. Treatment of scapholunate dissociation with a bioresorbable polymer plate: a biomechanical study. J Hand Surg - Am. 2008;33:643–649. doi: 10.1016/j.jhsa.2008.01.016. [DOI] [PubMed] [Google Scholar]
- 11.Short WH, Werner FW, Sutton LG. Dynamic biomechanical evaluation of the dorsal intercarpal ligament repair for scapholunate instability. J Hand Surg - Am. 2009;34:652–659. doi: 10.1016/j.jhsa.2008.12.009. [DOI] [PubMed] [Google Scholar]
- 12.Short WH, Werner FW, Green JK, Weiner MM, Masaoka S. The Effect of Sectioning the Dorsal Radiocarpal Ligament and Insertion of a Pressure Sensor into the Radiocarpal Joint on Scaphoid and Lunate Kinematics. J Hand Surg - Am. 2002;27:68–76. doi: 10.1053/jhsu.2002.30074. [DOI] [PubMed] [Google Scholar]
- 13.Green JK, Werner FW, Wang H, Weiner MM, Sacks JM, Short WH. Three-dimensional modeling and animation of two carpal bones: a technique. J Biomechanics. 2004;37:757–762. doi: 10.1016/j.jbiomech.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 14.Braidotti F, Atzei A, Fairplay T. Dart-Splint: An innovative orthosis that can be integrated into a scapho-lunate and palmar midcarpal instability re-education protocol. J Hand Therapy. 2015;28:329–335. doi: 10.1016/j.jht.2015.01.007. [DOI] [PubMed] [Google Scholar]
- 15.Upal MA, Crisco JJ, Moore DC, Sonenblum SE, Wolfe SW. In vivo elongation of the palmar and dorsal scapholunate interosseous ligament. J Hand Surg - Am. 2006;31:1326–1332. doi: 10.1016/j.jhsa.2006.06.005. [DOI] [PubMed] [Google Scholar]