

Abstract
Pulmonary scintigraphy has a well-established role in the diagnosis of pulmonary embolism (PE). The diagnostic specificity is increased if the perfusion study is combined with assessment of regional ventilation. VQ scans interpreted as either normal, near-normal, or high probability are reasonably diagnostic. Misinterpretation of the VQ scan can result in failure of this simple and noninvasive modality to diagnose a PE. Dose infiltration of the perfusion tracer is one of the rare causes of the misinterpretation of the VQ scan study. We present the VQ scan images of two patients and discuss the findings when Tc99m macroaggregated serum albumin (MAA) dose infiltration was recognized and the perfusion study was repeated for optimal interpretation.
Abbreviations: MRI, magnetic resonance imaging; CT, computed tomography; V/Q scan, ventilation-perfusion scan
Case report
Case 1 was of a 59-year-old female with a history of asthma who presented with cough and fever. Chest x-ray showed cardiomegaly and mild prominence of the pulmonary vasculature, consistent with minimal congestive heart failure. The VQ scan was performed to rule out PE. On the first day, the ventilation images and perfusion images looked similar, and there was some soft-tissue and renal activity in the perfusion images (Fig. 1). These observations were thought to be suspicious for Tc99m MAA dose infiltration. To further confirm this, count rates were checked during ventilation and perfusion scanning. The count ratio was only 2.5, with the count rate of 2.04 Kcounts/second in the ventilation study and 5.15 Kcounts/second in the perfusion study. The perfusion study was repeated the next day after the IV administration of 192.4 MBq (5.2 mCi) of Tc99m MAA (Fig. 2), and a higher count rate was achieved (7.6 Kcounts/second). Matched defects were reported in bilateral lower lung zones (more pronounced on ventilation), without any definite evidence of segmental mismatched perfusion defects, consistent with a “low” probability for PE, according to the PIOPED criteria.
Figure 1.
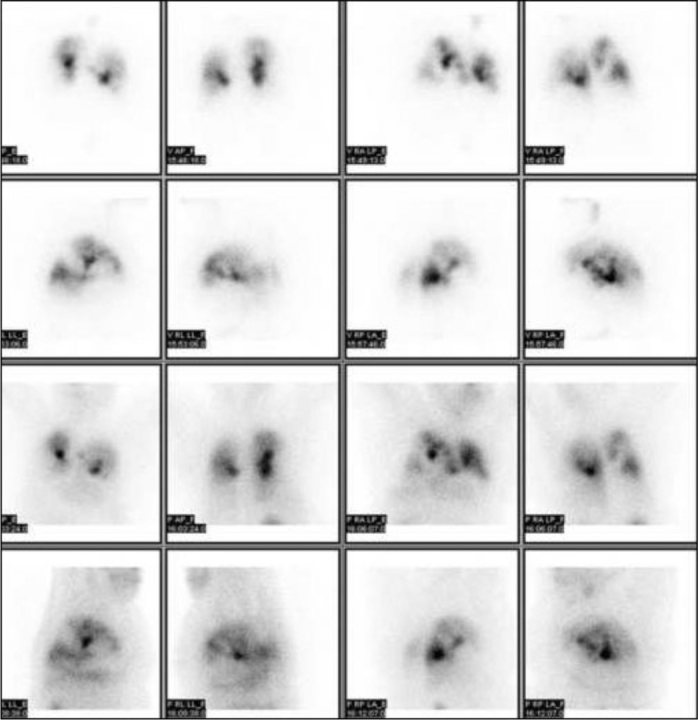
59-year-old female with suspected pulmonary embolism. The V/Q scan on day one. Ventilation and perfusion images are mirror copies of each other due to significant dose infiltration during perfusion. V-ventilation, P-perfusion.
Figure 2.
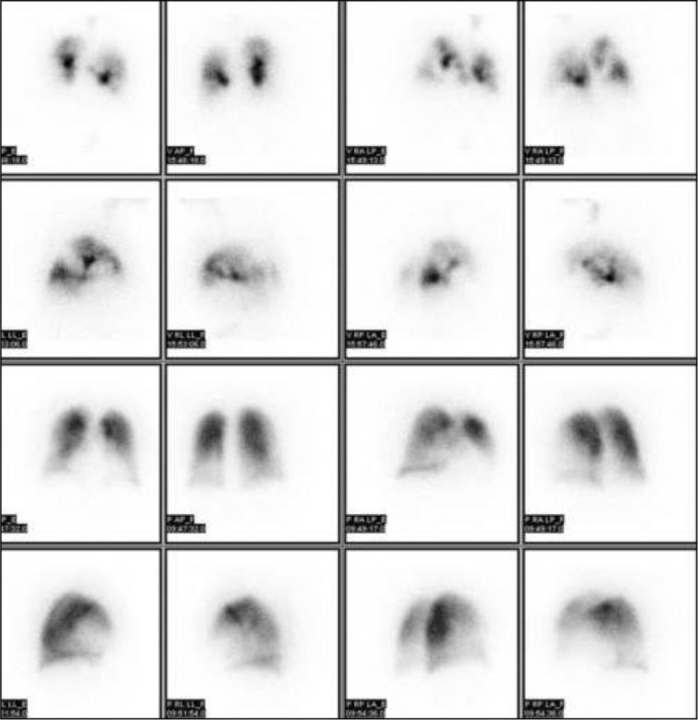
59-year-old female with suspected pulmonary embolism. Repeated perfusion images of the patient in case 1 on the following day (bottom two rows).
Case 2 is of a 51-year-old female who presented with chest pain. A VQ scan was performed to rule out PE. The images (Fig. 3) showed heterogeneous activity in both lungs. The ventilation and perfusion images looked similar, with some soft-tissue and renal activity in the perfusion images. Again, this was thought to be suspicious for Tc99m MAA dose infiltration, which was confirmed by noting the count rate on the ventilation study (4.5 Kcounts/second) and the count rate on perfusion study (9.8 Kcounts/second), with the ratio of counts being only 2.1. The perfusion study was repeated the next day (Fig. 4), after the IV administration of 196.1 MBq (5.3 mCi) of Tc99m MAA, and the count rate was higher (12.5 Kcounts/second). Bilateral, scattered, matched defects were reported in the lungs (more pronounced on ventilation), without any definite evidence of segmental, mismatched, perfusion defects, consistent with a “low” probability for PE.
Figure 3.
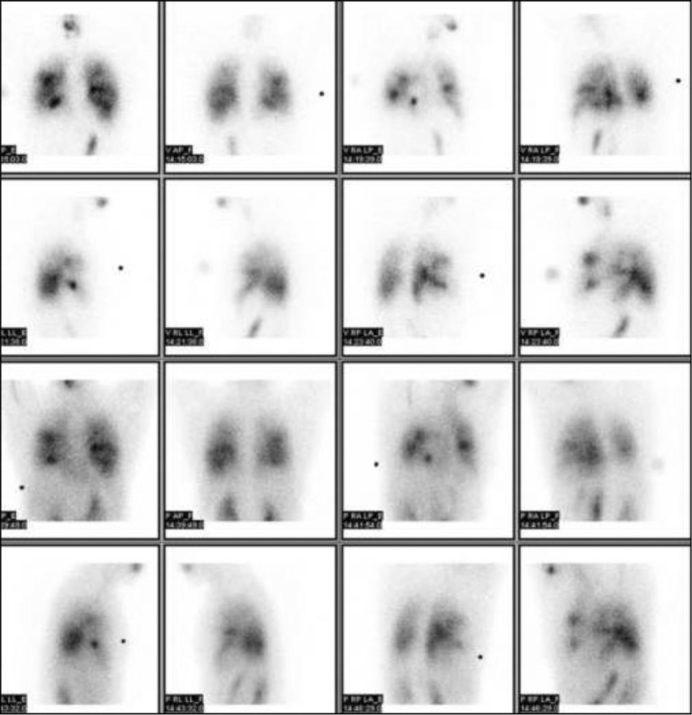
51-year-old female with suspected pulmonary embolism. The V/Q scan of patient in case 2 on day one, again showing absence of tracer signal in perfusion images due to dose infiltration.
Figure 4.
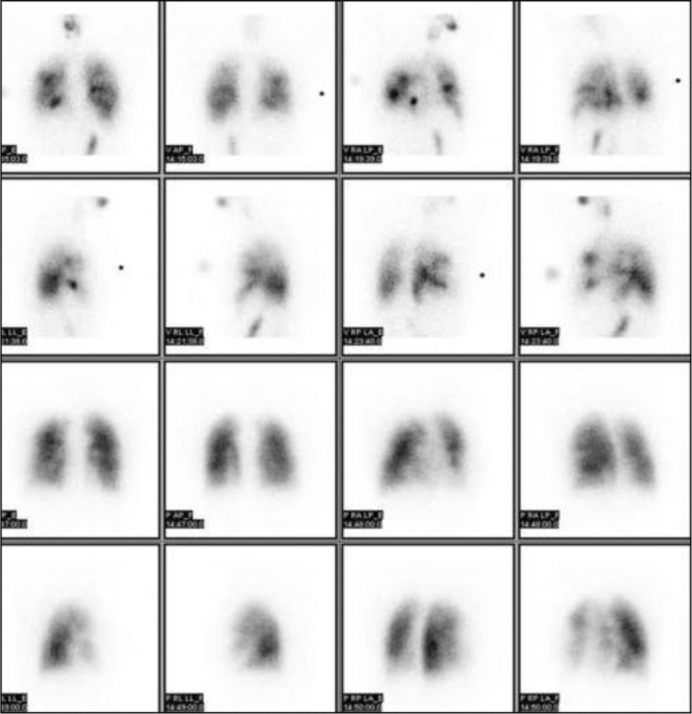
51-year-old female with suspected pulmonary embolism. Repeated perfusion scan of the patient in case 2 on the following day (bottom two rows).
Discussion
The VQ scan remains an important modality for the diagnosis of PE (1, 2, 3, 4, 5, 6). It helps to identify the patients at risk for future embolic events if they do not undergo anticoagulation. When combined with objective studies of the venous system, the VQ scan provides a guide to management for the great majority of patients. Several publications have shown that some emboli found on angiography are clinically benign and, in the absence of persistent thrombosis of the lower extremities, do not require anticoagulation (1).
In the United States, Tc99m DTPA and Tc99m MAA are the most frequently used agents for ventilation and perfusion imaging, respectively (7). Tc99m DTPA is a low-molecular-weight molecule that crosses the respiratory epithelium, enters the bloodstream, and is excreted by the kidneys (7). After the tracer has been inhaled through the nebulizer, images of the lungs are acquired in eight standard projections. Perfusion imaging is performed later when, after the IV administration of Tc99m MAA, images of the lungs are acquired (7). If there is accidental infiltration of the Tc99m MAA dose, the remains of tracer from ventilation activity (Tc99m DTPA) contribute to findings on the perfusion images. Dose infiltration of MAA at the injection site can cause uneven distribution of the radioactivity in the vascular bed and can significantly lower the amount of radioactivity reaching the lungs. Dose infiltration can be diagnosed by visual inspection of the images, imaging the site of injection, confirming the counts on the ventilation and perfusion images, and quantitative analyses. The count rate of the perfusion study should be at least three to four times higher than that of the ventilation study for adequate imaging.
In the first case, the count rate of the perfusion study on the first day was only 2.5 times that of the ventilation study. In the second case, the count rate of the perfusion study on the first day was only 2.1 times that of ventilation study. In both cases, the perfusion images looked similar to the ventilation images, and there was some soft-tissue and renal activity, likely from the metabolism of Tc99m DTPA. The perfusion study was repeated the next day.
Our reports recognize the dose infiltration as an important pitfall causing inaccurate, nonrepresentative perfusion images in a VQ scan with the potential for misinterpretation—in particular, for decreased sensitivity in diagnosing PE. Once recognized on the images, Tc99m MAA infiltration can be confirmed by evaluating ventilation and perfusion scan count rates, and if significant infiltration of the perfusion dose has occurred, the perfusion study should be repeated.
Footnotes
Published: December 29, 2011
References
- 1.Juni JE, Alavi A. Lung scanning in the diagnosis of pulmonary embolism: The emperor redressed. Seminars in Nuclear Medicine. 1991;XXI(4):281–296. doi: 10.1016/s0001-2998(05)80132-1. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Buxton-Thomas MS, Wraight EP. The use of 99Tcm-DTPA aerosol ventilation scintigraphy in the diagnosis of pulmonary embolism. Nucl Med Commun. 1984 Jun;5(6):387–391. doi: 10.1097/00006231-198406000-00005. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Worsley DF, Alavi A, Palevsky H. Role of radionuclide imaging in patients with suspected pulmonary embolism. Radiologic Clinics of North America. 1993;31:849–858. [PubMed] [PubMed] [Google Scholar]
- 4.Bergus GR, Barloon TS, Kahn D. An approach to diagnostic imaging of suspected pulmonary embolism. Am Fam Physician. 1996;53(4):1259–1266. [PubMed] [PubMed] [Google Scholar]
- 5.Biello DR. Radiological (scintigraphic) evaluation of patients with suspected pulmonary thromboembolism. JAMA. 1987; Jun 19;257(23):3257–3259. [PubMed] [PubMed] [Google Scholar]
- 6.Gotway MB, Edinburgh KJ, Feldstein VA, Lehman J, Reddy GP, Webb WR. Imaging evaluation of suspected pulmonary embolism. Curr Probl Diagn Radiol. 1999;28(5):129–184. doi: 10.1016/s0363-0188(99)90018-x. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Stein PD, Gottschalk A. Critical review of ventilation/perfusion lung scans in acute pulmonary embolism. Progress in cardiovascular diseases. 1994;XXXVII(1):13–24. doi: 10.1016/s0033-0620(05)80048-9. [PubMed] [DOI] [PubMed] [Google Scholar]