

Abstract
We present a case of failure of acromioclavicular joint (ACJ) reduction that was performed with low-profile, double-metallic button technique (Tightrope; Arthrex Inc). The patient presented with coracoid fracture and loss of reduction within eight weeks of surgery.
Abbreviations: MRI, magnetic resonance imaging; CT, computed tomography; ACJ, acromioclavicular joint
Case report
A 32-year-old male electrician underwent arthroscopically assisted ACJ reduction with a low-profile, double-metallic button technique (Tightrope; Arthrex Inc), with allograft after a relatively acute type III ACJ separation sustained in an ATV accident (Fig. 1).
Figure 1.

32-year-old male with type III ACJ dislocation. AP radiograph shows superior dislocation of distal clavicle from ACJ, with increased coracoclavicular interval, indicating disruption of coracoclavicular ligaments of the lesion.
Within eight weeks of surgery, while doing weightlifting exercises, he experienced an acute sense of “popping” in the shoulder with acute pain. Radiographs revealed a coracoid fracture with pull-through of the Tightrope device and recurrent ACJ separation (Fig. 2). At this point, it was decided to follow the patient with nonoperative management. His symptoms are subsiding, and it is felt that with continued work on strengthening and range of motion, his activity level will increase with time.
Figure 2.
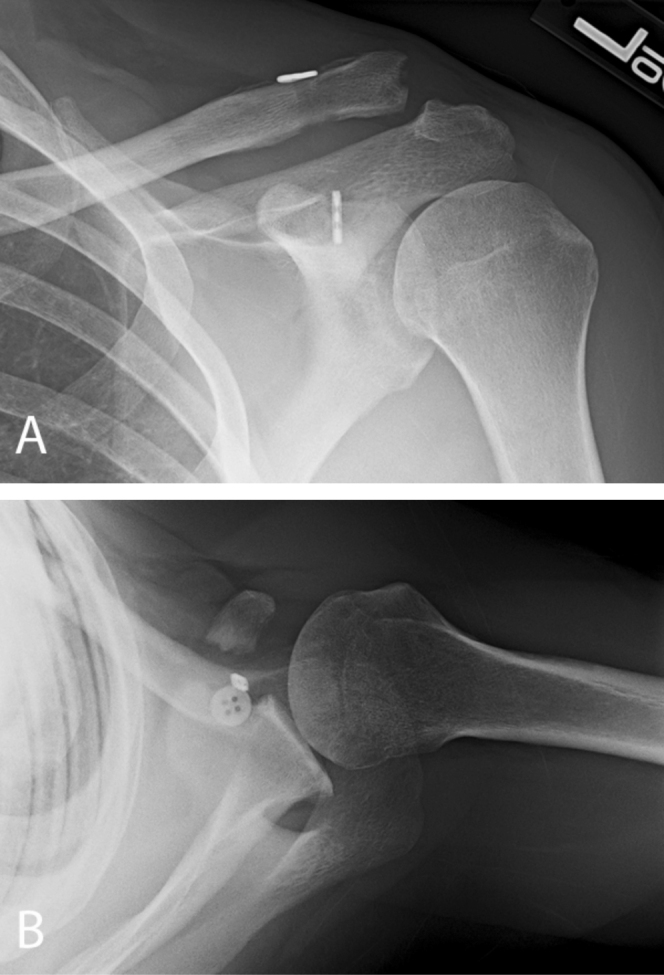
32-year-old male with failed Tightrope reconstruction of ACJ within eight weeks of surgery. Views of left shoulder. A. AP view shows malpositioned coracoid endobutton with some superior subluxation of distal clavicle. B. Axillary view shows coracoid fracture and confirms pulled through coracoid endobutton.
Discussion
ACJ dislocation is a common injury that often affects young adults. Its sequelae range from an asymptomatic shoulder to one that is painful, with significant loss of strength in the affected upper limb. The management of ACJ dislocation is dictated by the type of injury. In general, type I and II injuries are treated nonoperatively. On the other end of the spectrum, type IV, V, and VI injuries nearly always require operative intervention. The initial treatment of an acute type III separation of the ACJ, however, remains controversial. Although many studies have demonstrated successful outcome with nonoperative treatment, several other studies have noted variable outcomes. Many of these patients have undergone subsequent surgical treatment for ongoing symptoms of both pain and/or weakness. This has led to a commonly accepted recommendation of surgical treatment in high-level athletes or high-demand manual laborers (1).
However, many of the surgical techniques have been associated with significant implant-related complications (2). The traditional Weaver-Dunn procedure (and its modifications) avoids the use of metallic implants and continues to be a popular procedure. The original Weaver-Dunn procedure described in 1972 combines resection arthroplasty of the ACJ with fixation of the clavicle in an anatomical position by suture of the acromial end of the shortened coraco-acromial ligaments into the medullary canal of the clavicle (3). Although many of the modifications of this procedure have shown excellent success, implant -elated complications (including infection, soft tissue reactivity, and fractures) have been identified. Also, this ligament reconstruct has been shown to be weaker and much more compliant than the native ligament (4).
A relatively new technique for ACJ reconstruction uses a low-profile, double-metallic button technique (Tightrope; Arthrex Inc, Naples, Fla) for reduction of the coracoclavicular interval. The fixation device consists of a no. 5 Fiberwire suture that is tensioned and secured at both ends by metallic buttons against the cortices of the clavicle and the coracoid (5, 6). The proposed advantages include a nonrigid fixation of the ACJ that maintains reduction yet allows for normal movement (7).
Immediate anatomical reduction of an acute ACJ separation with flip-button devices provides satisfactory clinical results at intermediate-term followup (8). Walz et al reported favorable in-vitro results of this reconstruction technique with equal or even higher forces than native ligaments (9).
The implant can be used either as a standalone device or in conjunction with other biologic implants to improve long-term stability. In our case, the implant (along with the allograft) failed within eight weeks of the surgical repair. The patient’s early exercise could very well have contributed to the coracoid fracture with loss of reduction. However, further clinical experience will better define the success rate of this new technique.
Footnotes
Published: December 06, 2011
References
- 1.Struhl Steven. Double endobutton technique for repair of complete acromioclavicular joint dislocations. Tech Shoulder Elbow Surg. 2007;8(4):175–179. [Google Scholar]
- 2.Tsou PM. Percutaneous cannulated screw coracoclavicular fixation for acute acromioclavicular dislocations. Clin Orthop Relat Res. 1989 Jun;243:112–121. [PubMed] [PubMed] [Google Scholar]
- 3.Weaver JK, Dunn HK. Treatment of acromioclavicular injuries, especially complete acromioclavicular separation. J Bone Joint Surg Am. 1972 Sep;54(6):1187–1194. [PubMed] [PubMed] [Google Scholar]
- 4.Luis GE, Yong CK, Singh DA, Sengupta S, Choon DS. Acromioclavicular joint dislocation: a comparative biomechanical study of the Palmaris-longus tendon graft reconstruction with other augmentative methods in cadaveric models. J Orthop Surg Res. 2007 Nov 27;2:22. doi: 10.1186/1749-799X-2-22. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Petscavage J, Perez F, Khorashadi L, Richardson ML. Tightrope walking: A new technique in ankle syndesmosis fixation. Radiology Case Reports. [Online] 2010;5:354. doi: 10.2484/rcr.v5i1.354. (http://radiology.casereports.net/index.php/rcr/article/view/354/707) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lam DL, Chew FS. Tightrope fixation of complex acromioclavicular separation: A high-wire act. Radiology Case Reports. (Online) 2011;6:509. doi: 10.2484/rcr.v6i3.509. (http://radiology.casereports.net/index.php/rcr/article/view/509/836) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lim YW, Sood A, van Riet RP, Bain GI. Acromioclavicular joint reduction, repair and reconstruction using metallic buttons—early results and complications. Tech Shoulder Elbow Surg. 2007;8(4):213–221. [Google Scholar]
- 8.Salzmann GM, Walz L, Buchmann S, Glabgly P, Venjakob A, Imhoff AB. Arthroscopically assisted 2-bundle anatomical reduction of acute acromioclavicular joint separations. Am J Sports Med. 2010 Jun;38(6):1179–1187. doi: 10.1177/0363546509355645. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.Walz L, Salzmann GM, Fabbro T, Eichhorn S, Imhoff AB. The anatomic reconstruction of acromioclavicular joint dislocations using 2 Tightrope devices: a biomechanical study. Am J Sports Med. 2008 Dec;36(12):2398–2406. doi: 10.1177/0363546508322524. [PubMed] [DOI] [PubMed] [Google Scholar]