

Abstract
Numerous techniques have evolved for acromioclavicular joint fixation over the past decade to help decrease the risk of hardware complications and improve patient satisfaction. One of these techniques involves the TightRope system, which employs two titanium endobuttons to help reduce and secure the coracoclavicular joint. Clinical outcomes have been favorable, as orthopedic surgeons have gained more experience using this nonrigid system. It is important for radiologists to be aware of the radiographic appearance of this device and its associated complications.
Abbreviations: MRI, magnetic resonance imaging; CT, computed tomography
Case report
A 48-year-old motorcycle enthusiast with chronic right acromioclavicular (AC) joint separation and previous right clavicle fracture crashed his motorcycle at high speed at the raceway yet again. He sustained a right AC and coracoclavicular (CC) joint separation with posterior displacement of the proximal clavicle fracture fragment (Rockwood Type IV) (1, 2, 3) (Fig. 1). He underwent an internal repair of the distal clavicle fracture and repair of the AC separation with a “tightrope” fixation device.
Figure 1.
48-year-old male with complex acromioclavicular separation. Rockwood Type IV clavicle fracture with severe comminution of the distal fracture fragment and associated acromioclavicular and coracoclavicular joint separation. There is also a displaced fracture of the 3rd rib.
Intraoperatively, the distal clavicle was found to be quite scarred inferiorly due to his previous fracture, and no CC ligaments were attached to the inferior tubercle. The distal clavicle fracture was reduced and maintained in place by a temporizing Steinmann pin (Fig. 2A). A drill guide was used to place a hole through the central third of the clavicle into the base of the coracoid, a pin was placed through the clavicle and coracoid to check positioning, and this was over-reamed with a cannulated 4mm drill bit (Fig. 2B). Then, reconstruction of the coracoclavicular separation was performed using a “TightRope” fixation kit, and the Steinmann pin was removed. The fracture of the distal third of the clavicle was treated by suture fixation (Fig. 2C).
Figure 2A.
48-year-old male with complex acromioclavicular separation. Intra-operative reduction with temporizing Steinmann pin.
Figure 2B.
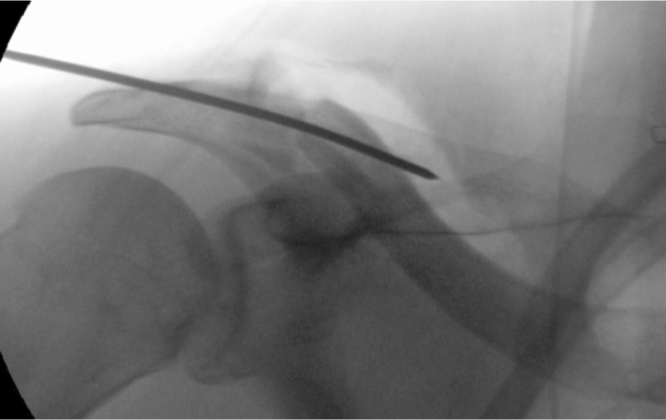
48-year-old male with complex acromioclavicular separation. A tunnel for the TightRope is prepared with a cannulated drill bit passing through the clavicle and the coracoid process
Figure 2C.

48-year-old male with complex acromioclavicular separation. The reduction is maintained by the TightRope following removal of the Steinmann pin.
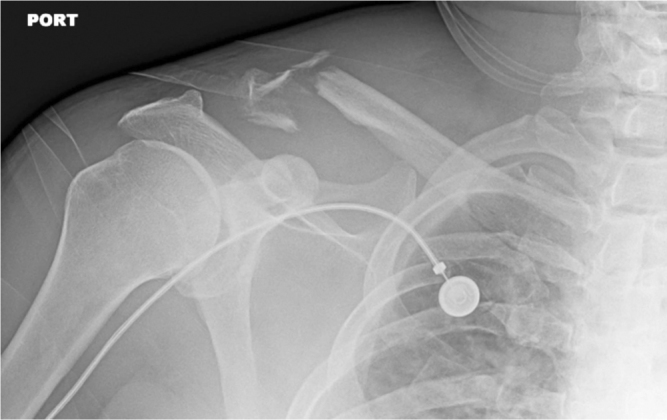
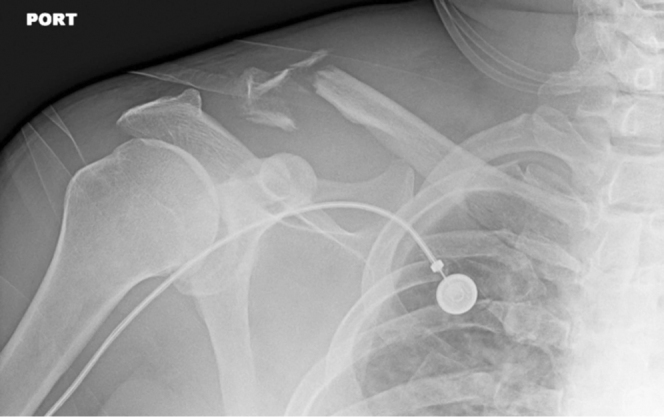
Followup images six weeks later showed continued improved anatomic alignment of the clavicle post tightrope fixation with persistent widening of the AC joint (Fig. 3). The patient continues to do well, with increasing strength, a full range of motion, and no complications.
Figure 3.

48-year-old male with complex acromioclavicular separation. At 6 weeks, the CC joint remains reduced with the TightRope in place. The clavicle fractures are healing.
Discussion
Acromioclavicular joint separations are one of the most common shoulder injuries. The are usually due to direct force applied at the superior-lateral aspect of the shoulder, with the arm in adducted position.
Over the past few decades, dozens of surgical techniques have been used to stabilize the AC joint, including primary joint fixation with screws, plates, suture wires, suture-based anchors, and pins; isolated ligament and/or tendon transfers; distal clavicle resection (with or without ligament reconstruction); and double-endobutton techniques. The most effective operative technique remains controversial, and there has yet to emerge a gold standard (1, 2, 4, 5, 6).
The use of rigid fixation with pins and screws is associated with complications such as hardware migration and fracture and/or loosening, which is compounded by the loss of normal joint movement. In addition, a second operation may be needed to remove hardware (1, 5, 6, 7, 9, 10). The advantages of the more recent techniques include the preservation of normal joint function, minimal scarring, faster recovery time, and a reduction in risk of coracoid fracture (1, 8).
One of the most recent techniques is the TightRope system, which was originally designed for ankle syndesmosis fixation but has since been expanded to include acromioclavicular joint injuries. This device consists of a multistranded polyethylene core (fiberwire) suture with a polyester braided jacket that is looped twice through two titanium buttons—one oblong and the other round—and tightened to hold the clavicle in position relative to the coracoid under tension (Fig. 4) (11).
Figure 4.
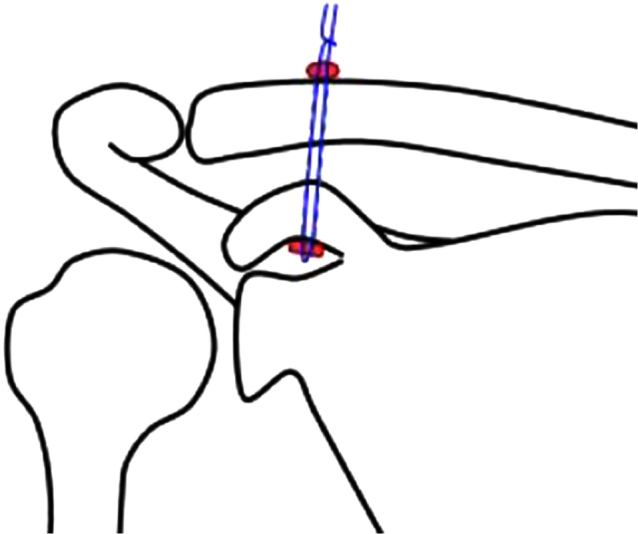
48-year-old male with complex acromioclavicular separation. Pictorial image of the endobuttons (red) with the fiberwire suture (blue) being tied down to reduce the coracoclavicular joint separation.
One advantage of the TightRope system is that it is a permanent device and thus does not need a separate operation to remove fixation hardware. Another advantage is that it maintains reduction yet allows for normal physiologic movement at the joint. Complications include loss of reduction (which could in part be due to the suture abrasion from other fixation hardware against sharp bony fragments), subsidence and displacement of the endobuttons (thought to be due to the use of a larger drill bit to create the portal), and posterior displacement of the clavicle with respect to the anterior edge of the acromion, which is best evaluated on axillary views (5, 8, 9). The relationship of the two endobuttons to each other is fixed by the suture that holds them together, and it is important to pay attention to the space between the endobuttons on subsequent followup films. If this space increases, it suggests that the suture has broken or become undone.
A number of radiographically similar but different techniques are used for AC joint separation, such as a double-endobutton technique. In this technique, an oblong button instead of a circular button is used on both ends as well as the two TightRope fixation devices, one to replicate each of the coracoclavicular ligaments (6, 9). A biomechanical study with reconstructions of both the conoid and trapezoid ligaments using two TightRope fixation devices showed that this device provides stabilization and can withstand similar or even higher vertical and anterior forces than the native ligaments (7). It is important to recognize these differences on radiographs to help predict complications due to differences in surgical technique.
The use of the TightRope fixation system and its variants is becoming more common in the reduction of acromioclavicular joint injuries. One might expect to see similar devices used for other injuries where reduction can be maintained by tension alone. It is important for radiologists to be aware of the postoperative radiographic appearance of this device and to be able to predict and recognize potential complications.
Footnotes
Published: July 17, 2011
References
- 1.Rios CG, Mazzocca AD. Acromioclavicular joint problems in athletes and new methods of management. Clin Sports Med. 2008 Oct;27(4):763–788. doi: 10.1016/j.csm.2008.06.006. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Melenevsky Y, Yablon CM, Ramappa A, Hochman MG. Clavicle and acromioclavicular joint injuries: a review of imaging, treatment, and complications. Skeletal Radiol. 2010 Jun 6 doi: 10.1007/s00256-010-0968-3. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.DeBerardino TM, Pensak MJ, Ferreira J, Mazzocca AD. Arthroscopic stabilization of acromioclavicular joint dislocation using the AC graftrope system. J Shoulder Elbow Surg. 2010 Mar;19(2 Suppl):47–52. doi: 10.1016/j.jse.2009.12.014. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Bahk MS, Kuhn JE, Galatz LM, Connor PM, Williams GR., Jr. Acromioclavicular and sternoclavicular injuries and clavicular, glenoid, and scapular fractures. J Bone Joint Surg Am. 2009 Oct;91(10):2492–2510. [PubMed] [PubMed] [Google Scholar]
- 5.Lim YW, Sood A, van Riet RP, Bain GI. Acromioclavicular joint reduction, repair and reconstruction using metallic buttons—early results and complications. Tech Shoulder Elbow Surg. 2007;8(4):213–221. [Google Scholar]
- 6.Struhl Steven. Double endobutton technique for repair of complete acromioclavicular joint dislocations. Tech Shoulder Elbow Surg. 2007;8(4):175–179. [Google Scholar]
- 7.Walz L, Salzmann GM, Fabbro T, Eichhorn S, Imhoff AB. The anatomic reconstruction of acromioclavicular joint dislocations using 2 TightRope devices: a biomechanical study. Am J Sports Med. 2008 Dec;36(12):2398–2406. doi: 10.1177/0363546508322524. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Richards A, Tennent TD. Arthroscopic stabilization of acute acromioclavicular joint dislocation using the tightrope system. Tech Shoulder Elbow Surg. 2008;9(2):51–54. [Google Scholar]
- 9.Salzmann GM, Walz L, Buchmann S, Glabgly P, Venjakob A, Imhoff AB. Arthroscopically assisted 2-bundle anatomical reduction of acute acromioclavicular joint separations. Am J Sports Med. 2010 Jun;38(6):1179–1187. doi: 10.1177/0363546509355645. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Nuber GW, Bowen MK. Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg. 1997 Jan;5(1):11–18. doi: 10.5435/00124635-199701000-00002. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.AC Joint TightRope Fixation [Internet]. Naples (FL): Arthrex; 2010 [cited 2010 Aug 1] Available from http://www.ankletightrope.com/easyedit/files/ac%20joint%20tightrope%20brochure.pdf