

Abstract
We present a case of pelvic osteosarcoma in an 18-year-old woman with a tumor thrombus in the left iliac vein, extending to the inferior vena cava. Tumor thrombus has been rarely described with osteosarcoma, with only 14 cases in the literature.
Case report
An 18-year-old Hispanic woman presented to her primary care physician with left hip, posterior buttock, and low back pain that continued to increase over several months. She then developed numbness along the lateral aspect of her left leg and foot. Subsequently, she presented to the emergency room because of difficulty ambulating secondary to severe left hip pain. CT of the abdomen and pelvis with contrast revealed a large, aggressive mass centered in the left iliac bone, along with lobulated, soft-tissue components, extensive areas of osseous matrix, and a sunburst periosteal reaction (Fig. 1). The imaging appearance was most consistent with osteosarcoma.
Figure 1.
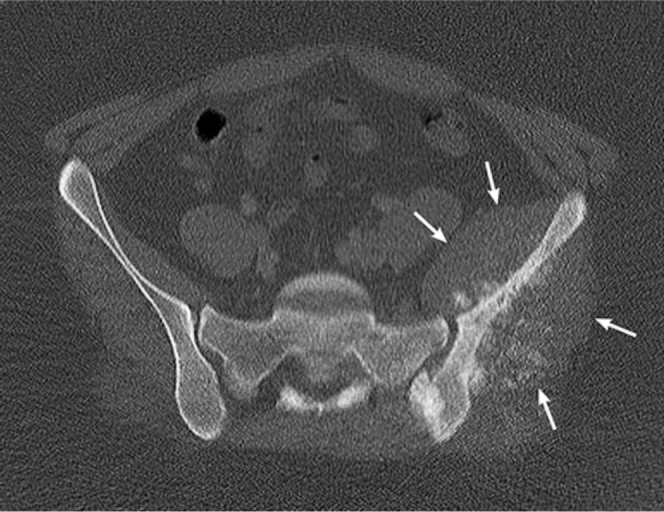
18-year-old woman with venous tumor thrombus. Axial CT through the upper pelvis showing the aggressive tumor (arrows) of the left iliac wing with osseous matrix and extensive soft-tissue components.
The left common iliac vein was noted to be enlarged and nonopacified, suspicious for a thrombus (Fig. 2). CT of the chest with contrast revealed a 2.3 × 1.5-cm noncalcified pulmonary nodule located posteriorly within the right lower lung. The patient was referred to our medical center for further evaluation and management.
Figure 2.

18-year-old woman with venous tumor thrombus. Coronal reformatted image of the initial CT shows a thrombus (arrow) extending from the left common iliac vein to the inferior vena cava.
Physical examination revealed tenderness to palpation over the left iliac bone region and left sacroiliac joint. Additionally, sensation was decreased on the lateral border of the left foot.
Contrast-enhanced MRI of the pelvis was performed to further evaluate the thrombus. This confirmed the large mass in the left iliac bone with soft-tissue components. Intraluminal, enhancing soft tissue was seen in a small venous tributary arising from the tumor. The tumor thrombus extended to the left common iliac vein and inferior aspect of the inferior vena cava (Figure 3, Figure 4). Additionally, there was extension into the left L5 and S1 neural foramina, and into the epidural space at S1. The tumor also extended into the greater sciatic notch, with enhancement around the sciatic nerve.
Figure 3.
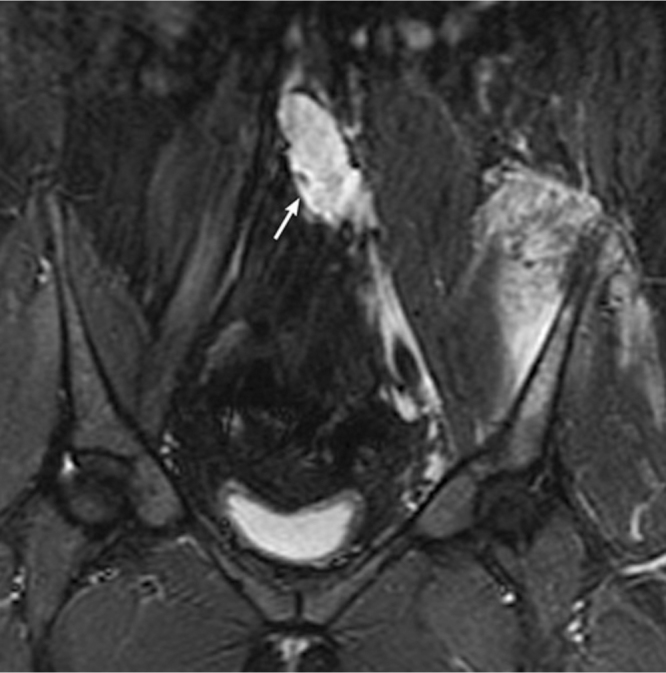
18-year-old woman with venous tumor thrombus. Coronal inversion recovery MR image of the pelvis shows the hyperintense thrombus (arrow) in the left common iliac vein extending to the inferior vena cava.
Figure 4.
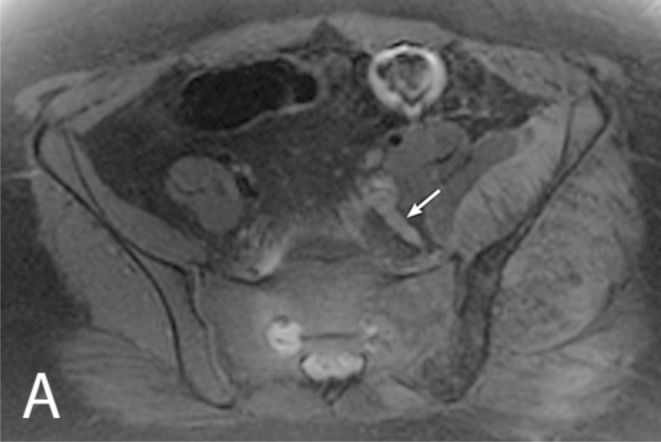
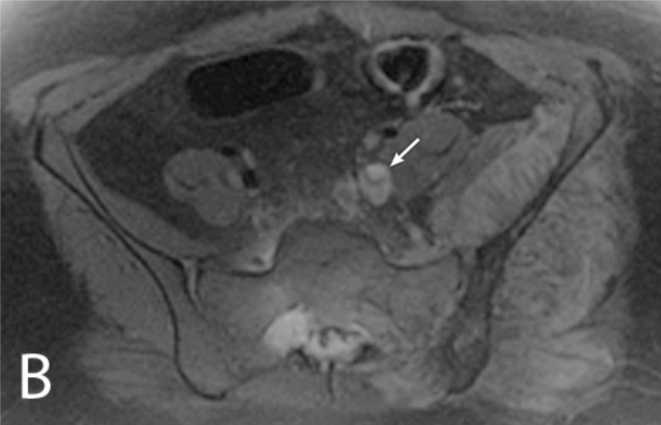
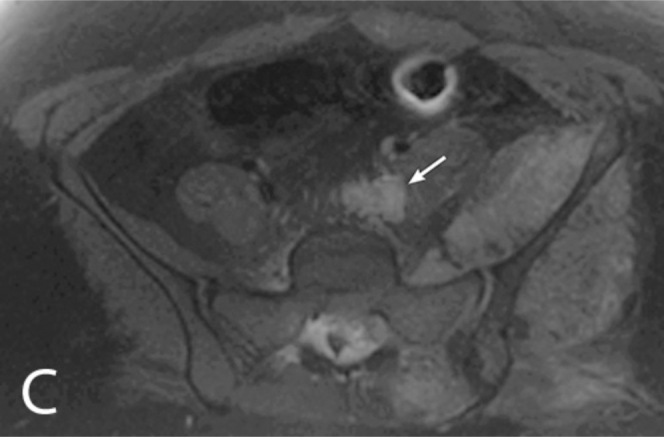
18-year-old woman with venous tumor thrombus. Axial T1W fat-saturated, postcontrast MR image of the pelvis.
Incisional biopsy of the left pelvic mass confirmed the suspected diagnosis of high-grade osteosarcoma. The patient is currently being treated with neoadjuvant chemotherapy agents, according to the high-risk arm of the Children’s Oncology Group Protocol AOST 0331, prior to surgical resection.
Discussion
Osteosarcoma is the most common bone sarcoma in adolescents and children, and approximately 1,000 new cases are diagnosed each year (1). The peak age of incidence is between 15 and 19 years of age (2). Approximately 12% of patients present with radiologic evidence of metastases, most commonly to the lung (3).
The pelvis is an uncommon site for osteosarcoma, accounting for 5% of all patients (4). Using the same treatment protocols, survival of patients with osteosarcoma of the pelvis is worse than the survival of patients with osteosarcoma not located in the pelvis (5). Isakoff et al. also found that the percentage of patients with pelvic osteosarcoma who had metastatic disease at presentation was significantly greater than for patients with primary tumors of any other site: 35% versus 16%, respectively (5). Janeway et al. reported poorer prognosis in osteosarcoma patients with metastatic disease at diagnosis, and those with a pelvic tumor site (6). Additionally, the event-free survival in patients greater than or equal to 18 years old was poorer because of an increased rate of relapse (6).
Tumor thrombi have been more frequently described with other tumors, primarily renal and liver malignancies. The main feature of tumor thrombus is the presence of an enhancing intraluminal mass. Additional findings include continuity of tumor with intravascular thrombus, vessel expansion by thrombus, and thrombus signal intensity characteristics similar to those of the adjacent tumor (7).
Tumor thrombus arising from osteosarcoma is rare, with only 14 previous reports (8). Of these 14 cases, tumor thrombus was detected by MRI in only one case, in addition to other imaging modalities (9). Tumor thrombus may be discovered incidentally during staging of the disease. Alternatively, patients may present with clinical findings corresponding to their intravascular site of growth.
In the past two decades, CT, MRI, and ultrasound have all been used to detect tumor thrombi. Most recently, simultaneous 18F-FDG-PET/CT aided in the accurate detection of tumor thrombus and the loclization of the vessel involved (10). Accurate detection of tumor thrombus versus bland venous thromboembolism is crucial in overall management, and to avoid unnecessary long-term anticoagulation.
Current potential curative treatment for metastatic osteosarcoma includes polychemotherapy and complete removal of all metastases, including surgical resection of the intravascular tumor thrombus (2, 8). Novel therapeutic approaches currently under investigation include agents that target tumor signal-transduction pathways, agents that inhibit tumor microtubules and other cell-cycle proteins, and immunomodulatory agents (11).
Footnotes
Published: September 20, 2013
References
- 1.Amankwah EK, Conley AP, Reed DR. Epidemiology and therapies for metastatic sarcoma. Clin Epidemiol. 2013;5:147–162. doi: 10.2147/CLEP.S28390. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ritter J, Bielack SS. Osteosarcoma. Ann Oncol. 2010;21(Suppl 7):vii320–vii325. doi: 10.1093/annonc/mdq276. [PubMed] [DOI] [PubMed] [Google Scholar]
- 3.Bielack SS, Kempf-Bielack B, Delling G, Exner GU, Flege S, Helmke K, Kotz R, Salzer-Kuntschik M, Werner M, Winkelmann W, Zoubek A, Jurgens H, Winkler K. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol. 2002;20(3):776–790. doi: 10.1200/JCO.2002.20.3.776. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Ries L, Eisner M, Kosary C, Hankey B, Miller B, Clegg L, Mariotto A, Feuer E, Edwards B. SEER Cancer Statistics Review, 1975–2001. National Cancer Institute; Bethesda, MD: 2004. Available at: http://seer.cancer.gov/csr/1975_2001/ Accessed July 17, 2013. [Google Scholar]
- 5.Isakoff MS, Barkauskas DA, Ebb D, Morris C, Letson GD. Poor survival for osteosarcoma of the pelvis: a report from the Children's Oncology Group. Clin Orthop Relat Res. 2012;470(7):2007–2013. doi: 10.1007/s11999-012-2284-9. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Janeway KA, Barkauskas DA, Krailo MD, Meyers PA, Schwartz CL, Ebb DH, Seibel NL, Grier HE, Gorlick R, Marina N. Outcome for adolescent and young adult patients with osteosarcoma: a report from the Children's Oncology Group. Cancer. 2012;118(18):4597–4605. doi: 10.1002/cncr.27414. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akin O, Dixit D, Schwartz L. Bland and tumor thrombi in abdominal malignancies: magnetic resonance imaging assessment in a large oncologic patient population. Abdom Imaging. 2011;36(1):62–68. doi: 10.1007/s00261-010-9608-6. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Navalkele P, Jones SM, Jones JK, Salazar JD, Toy PC, Iyer RV, Herrington B. Osteosarcoma tumor thrombus: a case report with a review of the literature. Tex Heart Inst J. 2013;40(1):75–78. [PubMed] [PMC free article] [PubMed] [Google Scholar]
- 9.Hines N, Lantos G, Hochzstein J, Gitig A, DeAnda A. Osteosarcoma of the lumbosacral spine invading the central venous pathways, right-sided cardiac chambers, and pulmonary artery. Skeletal Radiol. 2007;36(11):1091–1096. doi: 10.1007/s00256-007-0338-y. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Lai P, Bomanji JB, Mahmood S, Nagabhushan N, Syed R, Gacinovic S, Lee SM, Ell PJ. Detection of tumour thrombus by 18F-FDG-PET/CT imaging. Eur J Cancer Prev. 2007;16(1):90–94. doi: 10.1097/01.cej.0000220641.46470.77. [PubMed] [DOI] [PubMed] [Google Scholar]
- 11.O'Day K, Gorlick R. Novel therapeutic agents for osteosarcoma. Expert Rev Anticancer Ther. 2009;9(4):511–523. doi: 10.1586/era.09.7. [PubMed] [DOI] [PubMed] [Google Scholar]