

Abstract
Ischiofemoral impingement has been reported in a number of cases as an association between hip pain and quadratus femoris MRI signal abnormality, with concurrent narrowing of the ischiofemoral space. While the literature has included much emphasis on the imaging characteristics useful in the diagnosis of this entity, information on treatment has been scant, with few case reports of surgical resection of the lesser trochanter and incomplete descriptions of steroid injection techniques. We report a case of ultrasound- and CT-guided steroid injection into the ischiofemoral space via the proximal hamstring tendons in a 57-year-old female who had imaging and clinical characteristics of ischiofemoral impingement. The technique is described as a safe alternative to other possible injection techniques.
Case report
A 57-year-old female schoolteacher presented with chronic right hip pain of 1 year's duration. She described the pain as constant and deep, radiating from the lateral right groin region into the buttock, waking her up at night. Her pain was not relieved with nonsteroidal anti-inflammatory drugs, and was worse with athletic activities, particularly hiking. She reported no snapping symptoms. She was clinically diagnosed with greater trochanteric bursitis one year before presentation; however, her symptoms did not improve with trochanteric bursa steroid injection. The patient underwent physiotherapy for one year without improvement. She also underwent sacroiliac joint injection in the past, without improvement. She reported an ankle fracture and medial collateral ligament tear in the ipsilateral leg 7 and 15 years (respectively) before presentation.
The patient was subsequently referred for an MRI direct arthrogram of the right hip for a clinical suspicion of labral tear. The MRI study was performed on a Phillips Achieva 3 Tesla MRI scanner after intra-articular injection of diluted gadolinium. The sequences included the following:
-
•
Coronal T1 and proton-density, fat-suppressed (PD FS) sequences of both hips (40-cm field of view)
-
•
Axial T1, axial PD FS, coronal T1 FS, and sagittal T1 FS sequences of the right hip only (20-cm field of view)
The patient's feet were taped together, resulting in internal rotation of the hips. MRI images showed narrowing of the quadratus femoris and ischiofemoral spaces, which measured 8 mm and 17 mm, respectively (Fig. 1). The ischiofemoral space was defined as the smallest distance between the lateral cortex of the ischial tuberosity and medial cortex of the lesser trochanter. The quadratus femoris space was defined as the smallest space for passage of the quadratus femoris muscle, bordered by the superolateral surface of the hamstrings tendons and the posteromedial surface of the iliopsoas tendon or lesser trochanter. There was also a mild focal edema in the belly of the quadratus femoris muscle (Fig. 2). Although the muscle edema was mild, the patient's clinical history suggested a diagnosis of ischiofemoral impingement.
Figure 1.
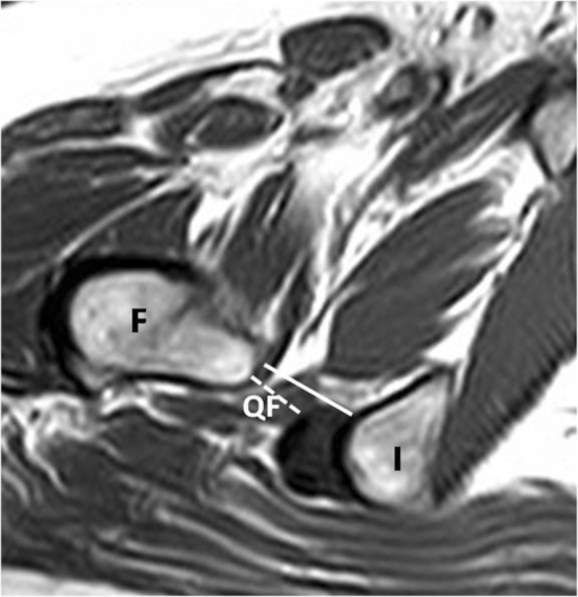
57-year-old female with ischiofemoral impingement. Axial T1-weighted image of the right hip through the lesser trochanter shows narrowing of the ischiofemoral (solid line) and quadratus femoris (dashed line) spaces. I = ischium, F = femur, QF = quadratus femoris
Figure 2.
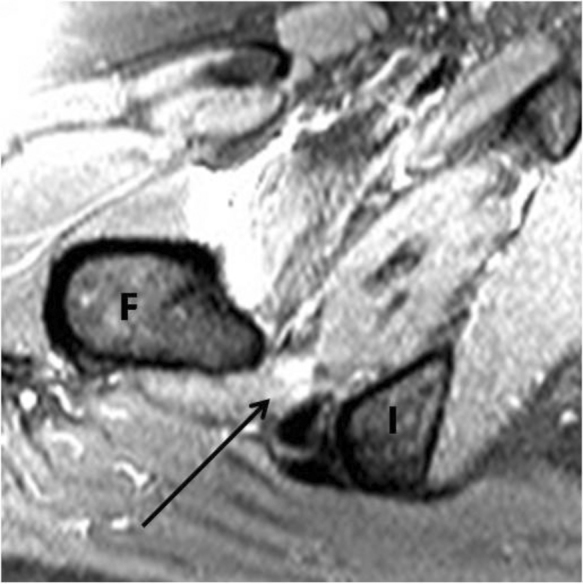
57-year-old female with ischiofemoral impingement. Axial PD FS image shows increased signal in the belly of the quadratus femoris muscle, consistent with edema (arrow). Increased signal around the iliopsoas insertion is thought to be from extravasation of intra-articularly injected gadolinium. I = ischium, F = femur.
The patient received three injections into the ischiofemoral space of combinations of 3 ml of lidocaine and 40 mg Depo-medrol. With each injection, the proximal hamstring tendons were used as a landmark where a 10-cm-long, 22-gauge spinal needle was placed through the tendons, into the ischiofemoral space. The first injection was performed with ultrasound (US) guidance, and immediate relief of symptoms lasting for 9 months was achieved (Fig. 3). The second US-guided injection resulted in 3 weeks of symptom relief. The third injection was performed with computed tomography (CT) guidance, and the patient had continued relief for 9 months (Fig. 4). The patient has reported symptoms of tightness at the proximal hamstring tendons, which has been relieved with stretching activities.
Figure 3.

57-year-old female with ischiofemoral impingement. Grayscale US image through the ischiofemoral space during a steroid injection demonstrates needle placement into the ischiofemoral space (arrows). Due to technical difficulties, the ischiofemoral space is not well delineated on US. Once the needle is placed through the proximal hamstring tendons (not shown), the needle is further advanced by about 2 cm to reach the quadratus femoris.
Figure 4.
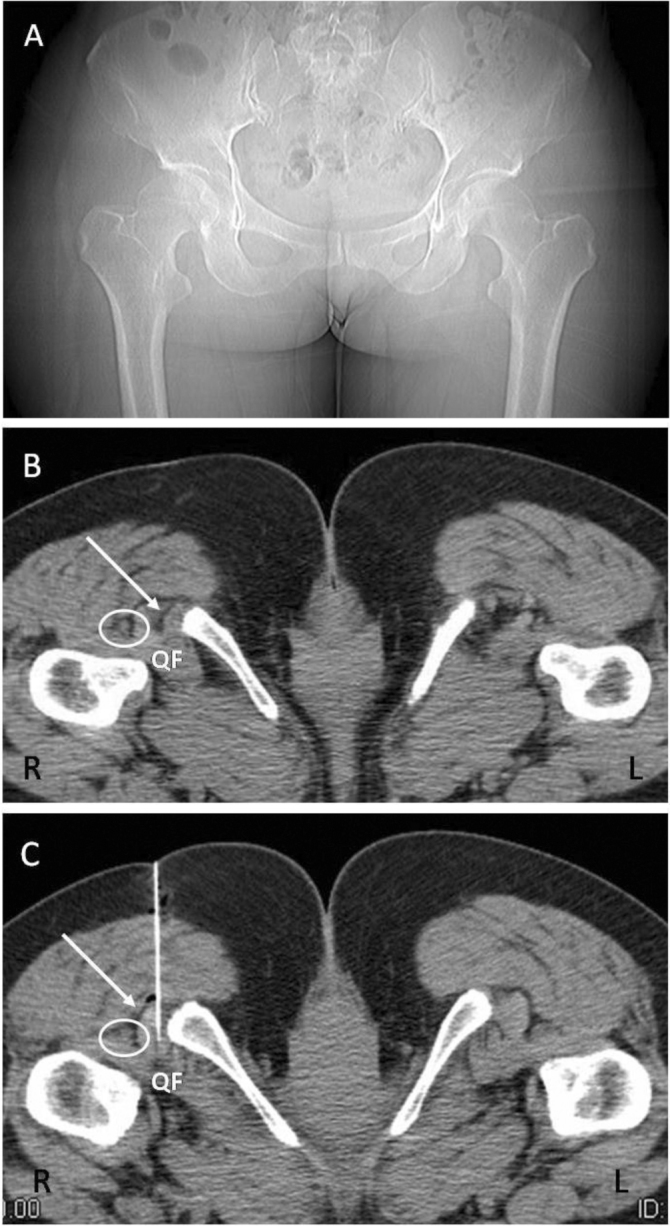
57-year-old female with ischiofemoral impingement. CT scout view (A) and axial CT images through the lesser trochanter during a steroid injection demonstrate asymmetric narrowing of the right ischiofemoral and quadratus femoris spaces (B) and placement of a 10cm-long 22-gauge spinal needle through the proximal hamstring tendons (straight arrow), into the ischiofemoral space (C). In the prone position, both hips were externally rotated, slightly more on the right side. Oval indicates sciatic nerve. QF = quadratus femoris.
Discussion
Abnormal contact between the acetabulum and femur or between the ischium and femur are the two main sources for impingement in the hip (1). While femoro-acetabular impingement is a well-known potential cause of hip pain, ischiofemoral impingement has been rarely described in the medical literature. Impingement between the ischium and femur was first suggested in three patients with prior hip surgery who obtained pain relief after lesser trochanter excision (2). Patti et al. described MRI findings of ischiofemoral space narrowing and impingement in a patient with hip pain and no history of surgery (3). This case demonstrated abnormal MR signal intensity of the quadratus femoris muscle, and narrowing of the space between the ischial tuberosity and lesser trochanter. Consequently, Torriani et al. described the entity of the ischiofemoral impingement syndrome in their study of nine patients with hip pain and abnormal MR intensity of the quadratus femoris muscle (1). In this study, all subjects with abnormal MR signal intensity of the quadratus femoris muscle were women, had significantly narrowed ischiofemoral spaces in comparison with control subjects, and demonstrated significantly narrowed quadratus femoris space. Abnormalities of the quadratus femoris muscle included edema (100%), partial tear (33%), and fatty infiltration (8%). The hamstring tendons of affected subjects showed evidence of edema (50%) and partial tears (25%). Stafford et al. further described the entity of the ischiofemoral impingement syndrome and its treatment (4).
The quadratus femoris muscle arises from the anterior portion of the ischial tuberosity, anterior to the origin of the hamstring tendons. It inserts along the posterior medial aspect of the proximal femur, into the minor tubercle of the trochanteric crest of the femur, and is a strong lateral rotator of the thigh (5, 6). It is bordered anteriorly by the obturator externus; posteriorly by fat, the sciatic nerve, and the hamstring tendons; superiorly by fat and the inferior gemellus; and inferiorly by the adductor magnus (5). It occupies the space between the lesser trochanter and the ischium, and may be compressed between these two bone structures (4). The normal distance between the lesser trochanter and the ischial tuberosity was thought to be approximately 20 mm (2). Torriani et al. (1), however, determined in their study that this space is reduced to 13 +/− 5 mm in patients with ischiofemoral impingement. This space was found to measure 23 +/− 8 mm in the asymptomatic control group in the same study. Narrowing of this space puts the quadratus femoris muscle at risk of damage due to repetitive abrasion (7).
Patients with ischiofemoral impingement present with chronic pain in the groin and/or buttock without a precipitating injury, and the pain may radiate distally (4). The differential diagnosis includes snapping psoas tendon, sciatica, chronic hamstring injury, quadratus femoris tear, and tendonitis (4). Imaging is important in the diagnosis of this condition. Though plain radiographs may be normal, they may demonstrate sclerosis and cystic changes in the lesser trochanter and ischium in patients with chronic impingement (4). MRI remains the best diagnostic modality for this entity, where edema within the muscle belly of quadratus femoris muscle is seen on T2-weighted images. The presence of edema in the muscle belly rather than the myotendinous junction, and absence of fiber disruption, help to distinguish ischiofemoral impingement from quadratus femoris muscle tear (5, 8). Quadratus femoris atrophy is also associated with this disorder, and is best visualized on T1-weighted MRI images as hyperintense fatty replacement and volume loss of the muscle (6). Tear of the quadratus femoris muscle is a different entity that has been described in the literature (9). It can occur with trauma and, although not reported, it can occur as a result of chronic ischiofemoral impingement, conceivably using the same mechanism as subacromial impingement (causing rotator-cuff tendon tears). It is therefore occasionally difficult to differentiate ischiofemoral impingement from trauma or other entities. Careful analysis of the muscle belly, myotendinous junction, and the ischiofemoral and quadratus spaces; of the ancillary findings of sclerosis of the lesser trochanter and lateral ischium; and of the clinical history may lead to the correct diagnosis (3, 5).
The diagnosis of ischiofemoral impingement in our patient was suggested based on narrowing of the spaces, a focal edema signal in the quadratus femoris muscle, and the clinical history. Even though the edema was focal and mild, we were confident about the diagnosis, as we have encountered similar cases. Our MRI hip-imaging protocol required taping of the feet, with the hip joints in internal rotation, which is similar to the technique reported by Torriani et al. Our MRI imaging protocol did not include large field-of-view axial sequences that would include both hips. We provide a CT image from the injection (Fig. 4) to show asymmetry of the ischiofemoral and quadratus femoris spaces between the right and left hips, to support the diagnosis of space narrowing and impingement on the right side. Although there is a slight asymmetric external rotation of the hips, we do not believe this accounted significantly for the ischiofemoral space narrowing on the right side.
In our injection technique, the proximal hamstring tendons were used as a landmark. The hamstring tendons were readily identifiable on both US and CT and provided a good landmark for both injection techniques. The quadratus femoris muscle is bordered posteriorly by the sciatic nerve and, as noted from the CT images (Fig. 4), the available spaces around sciatic nerve are inadequate for a lateral approach adjacent to the nerve. Placement of the injection needle through the hamstring tendons minimizes damage to the nerve. Also, for a CT-guided injection, placement of the needle through the hamstring tendons provides a vertically oriented path on a prone patient that is less challenging than obliquely oriented angles from the more lateral approaches.
It is of note that during the first US-guided injection, the patient felt immediate relief of her pain, but this was not achieved during the second US-guided injection. On US, the ischium and femur can be identified, but the muscles are difficult to define. This is due to various layers of tissues and the depth of the muscles from the imaging plane. US has been reported normal in a patient found to have impingement changes on MRI (10). Once the needle is placed through the hamstring tendons, we advanced the needle by approximately 2 cm to reach the quadratus femoris, as this is the average distance from the proximal hamstring tendon to the quadratus femoris muscle. It is thought that the needle placement was not directly in the quadratus muscle during the second US-guided injection. During the first US-guided injection, the patient immediately recognized her pain symptom when the needle was advanced into the quadratus femoris. She did not recognize this immediate pain relief during the second injection. We opted for CT guidance during the third injection, with successful results. On CT, the quadratus femoris muscle is readily identifiable. Immediate relief of symptoms is a good indicator of a successful injection.
Although there can be complications, including scarring and tearing associated with puncture of the hamstring tendons with a spinal needle, our patient experienced only tightness at the hamstring tendons, and this was relieved with stretching activities. We recommend keeping needle passages through the hamstring tendons to a minimum. There can also be complications with chronic steroid injections, including fat atrophy of the injected muscle and rare periarticular calcifications (11). Take care to avoid inadvertent injection of steroid into the hamstring tendons, as this could result in tendon rupture. The quadratus femoris tendon is thus not directly injected, and this potential complication can be minimized.
No definite treatment has been recommended other than excision of the lesser trochanter (2, 7). Some authors speculate that the ischiofemoral space would be amenable to arthroscopic access and endoscopic technique, which is currently used for treatment of other causes of hip pain (4). Radiologically guided infiltration of the ischiofemoral space with a combination of local anesthetics and steroids has been reported to be useful. One patient received immediate relief of inner-thigh pain from injection of betamethasone and lidocaine into the region of the lesser trochanter, although the pain in the hip persisted (2). Another patient with suspected quadratus femoris tendinitis received two injections of Depo-medrol under US guidance at the insertion of the quadratus femoris tendon, and demonstrated gradual but complete resolution of groin pain (12). One subject in the study by Torriani et al. received CT-guided steroid injection of the quadratus femoris muscle with relief of symptoms for 1 week (1). In our case, the patient has been receiving significant palliative relief with steroid injections.
It remains unclear if steroid injections provide only short-term symptom relief. With successful injections, our patient has had relief as long as 9 months for each injection, which is in the range of intermediate symptom relief. Most studies of steroid injections evaluate injections of tendinopathy, which is a noninflammatory condition. The pathology of the quadratus femoris muscle in ischiofemoral impingement is unknown. The impinged quadratus femoris muscle is bound to have repeated injuries as long as the impingement is not corrected. It is thus reasonable to assume that steroid injections provide palliative relief but not definitive treatment. Besides the reported surgical treatment with lesser trochanter resection (2, 7), physiotherapy would likely play an important role in the management of ischiofemoral impingement. There have been no publications addressing the rationale for each treatment.
In conclusion, although ischiofemoral impingement is an uncommon cause of hip pain that occurs predominantly in females, physicians should be aware of this entity. Imaging findings seen with this entity include the following:
-
•
Narrowing of the ischiofemoral and quadratus femoris spaces
-
•
Edema of the quadratus femoris muscle belly
-
•
Atrophy of the quadratus femoris
-
•
Sclerosis of the lesser trochanter and lateral ischium
We report a safe US- and CT-guided injection technique using the proximal hamstring tendons as a landmark for injection into the ischiofemoral space.
Acknowledgements
The authors wish to thank Dr. Shaun Fowler at Dr. Jones & Partners Medical Imaging in Adelaide, Australia for his contribution to the US-guided injection technique.
Footnotes
Published: March 10, 2013
References
- 1.Torriani M, Souto SC, Thomas BJ, Ouellette H, Bredella MA. Ischiofemoral impingement syndrome: an entity with hip pain and abnormalities of the quadratus femoris muscle. AJR Am J Roentgenol. 2009;193:186–190. doi: 10.2214/AJR.08.2090. [PubMed] [DOI] [PubMed] [Google Scholar]
- 2.Johnson KA. Impingement of the lesser trochanter on the ischial ramus after total hip arthroplasty. Report of three cases. J Bone Joint Surg Am. 1977;59:268–269. [PubMed] [PubMed] [Google Scholar]
- 3.Patti JW, Ouellette H, Bredella MA, Torriani M. Impingement of lesser trochanter on ischium as a potential cause for hip pain. Skeletal Radiol. 2008;37:939–941. doi: 10.1007/s00256-008-0551-3. [PubMed] [DOI] [PubMed] [Google Scholar]
- 4.Stafford GH, Villar RN. Ischiofemoral impingement. J Bone Joint Surg Br. 2011;93:1300–1302. doi: 10.1302/0301-620X.93B10.26714. [PubMed] [DOI] [PubMed] [Google Scholar]
- 5.Kassarjian A, Tomas X, Cerezal L, Canga A, Llopis E. MRI of the quadratus femoris muscle: anatomic considerations and pathologic lesions. AJR Am J Roentgenol. 2011;197:170–174. doi: 10.2214/AJR.10.5898. [PubMed] [DOI] [PubMed] [Google Scholar]
- 6.Tosun O, Algin O, Yalcin N, Cay N, Ocakoglu G, Karaoglanoglu M. Ischiofemoral impingement: evaluation with new MRI parameters and assessment of their reliability. Skeletal Radiol. 2012;41:575–587. doi: 10.1007/s00256-011-1257-5. [PubMed] [DOI] [PubMed] [Google Scholar]
- 7.Ali AM, Whitwell D, Ostlere SJ. Case report: imaging and surgical treatment of a snapping hip due to ischiofemoral impingement. Skeletal Radiol. 2011;40:653–656. doi: 10.1007/s00256-010-1085-z. [PubMed] [DOI] [PubMed] [Google Scholar]
- 8.Kassarjian A. Signal abnormalities in the quadratus femoris muscle: tear or impingement? AJR Am J Roentgenol. 2008;190:W379. doi: 10.2214/AJR.07.3540. [PubMed] [DOI] [PubMed] [Google Scholar]
- 9.O'Brien SD, Bui-Mansfield LT. MRI of quadratus femoris muscle tear: another cause of hip pain. AJR Am J Roentgenol. 2007;189:1185–1189. doi: 10.2214/AJR.07.2408. [PubMed] [DOI] [PubMed] [Google Scholar]
- 10.Peltola K, Heinonen OJ, Orava S, Mattila K. Quadratus femoris muscle tear: an uncommon cause for radiating gluteal pain. Clin J Sport Med. 1999;9:228–230. [PubMed] [PubMed] [Google Scholar]
- 11.Sparling M, Malleson P, Wood B, Petty R. Radiographic followup of joints injected with triamcinolone hexacetonide for the management of childhood arthritis. Arthritis Rheum. 1990;33:821–826. doi: 10.1002/art.1780330608. [PubMed] [DOI] [PubMed] [Google Scholar]
- 12.Klinkert P, Jr., Porte RJ, de Rooij TP, de Vries AC. Quadratus femoris tendinitis as a cause of groin pain. Br J Sports Med. 1997;31:348–349. doi: 10.1136/bjsm.31.4.348. [PubMed] [DOI] [PMC free article] [PubMed] [Google Scholar]