

Abstract
Double aortic arch (DAA) is a congenital vascular anomaly. The diagnosis was difficult till the child was symptomatic, and other causes were ruled out. We present the interesting images of a child of respiratory distress because of tracheal compression from DAA.
Keywords: Airway obstruction, anesthesia management, children, double aortic arch, vascular ring
INTRODUCTION
Double aortic arch (DAA) is the persistence of both left and right aortic arch after birth.[1] The presence of both the arches wraps the trachea and strangulates the trachea in the course of time producing airway obstruction.[1] The early diagnosis of DAA is difficult due to the rare occurrence. The exclusion of other causes of respiratory tract obstruction and the suspicion for DAA can guide the physician to diagnose with computerized tomography (CT) or magnetic resonance imaging.
CASE REPORT
A 7-year-old boy had a history of repeated pneumonia and stridor. He was not relieved of the symptoms by routine treatment. Fiberoptic bronchoscopy examination revealed tracheal narrowing at the lower end of the trachea without any internal pathology. The chest X-ray showed minimal narrowing above the bifurcation. He was planned for CT scan. Computerized tomography scan detected the presence of vascular ring surrounding the trachea [Figure 1]. Reconstruction of CT arteriography showed both right and left aortic arches around the trachea [Figures 2 and 3]. The diagnosis of DAA was confirmed. The right side arch was bigger and dominant. The child was scheduled for surgery. After oxygenation with 100% oxygen, anesthesia was induced with fentanyl 50 μg, midazolam 0.5 mg and ketamine 40 mg. Ease of ventilation was checked with bag and mask. Rocuronium 20 mg was administered to facilitate tracheal intubation. Trachea intubated with 5.5 mm cuffed tube and ventilated mechanically. Correct position of the endotracheal tube (ETT) was confirmed with fiberoptic bronchoscopy. Anesthesia was maintained with fentanyl, vecuronium, isoflurane and oxygen with air. Left thoracotomy was performed. The left side arch was divided and sutured at both ends. The child was ventilated mechanically for 12 h in Intensive Care Unit and trachea was extubated after slow weaning by continuous positive airway pressure mode with a full awake child. The child was relieved of symptoms without any stridor. He was kept under observation with adequate pain relief and humidification of inspired oxygen and discharged on 8th postoperative day.
Figure 1.
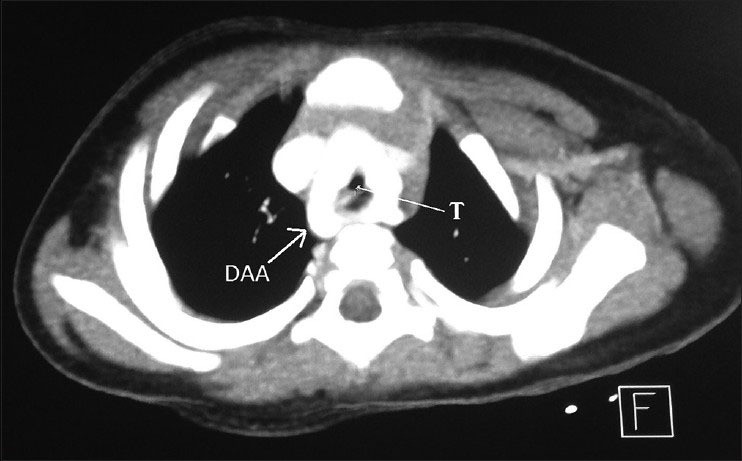
Contrast enhanced computerized tomography axial section image showing the double aortic arch (DAA, marked by white arrow) encircling the trachea (T, marked by white arrow)
Figure 2.
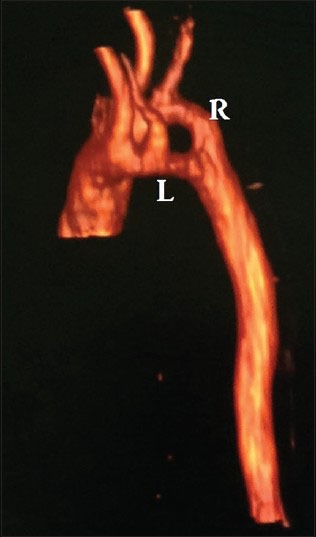
Computerized tomography reconstruction arteriography anterior view showing the right (R) and left (L) aortic arch making a vascular ring
Figure 3.
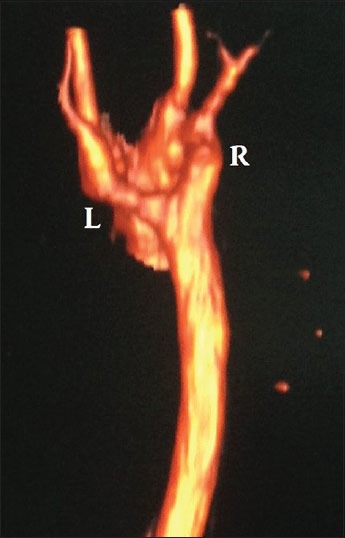
Computerized tomography reconstruction arteriography posterior view showing the bigger right (R) and smaller left (L) aortic arch
DISCUSSION
Double aortic arch is a rare congenital vascular malformation. DAA may be right dominant (70% case), left dominant (25%) and balanced type (5%).[1] The ring of the DAA gradually increases in size and produces compression over trachea and esophagus.[1] DAA may be associated with cardiac diseases or noncardiac diseases.[2,3] In our patient, the child had tracheal compression due to the DAA leading to stridor and repeated respiratory infection. Fiberoptic bronchoscope (FB) detected the problem and subsequent confirmation was established with CT scan. Resection of the left aortic arch relieved the tracheal compression. Surgical resection of one arch is the only curative treatment to relieve the compressive features. Airway management in the perioperative period and weaning from the ventilator are challenges for anesthesiologists.[4,5] Ventilation after intubation in these patients may be difficult if the tip of ETT is placed or migrated to lower level in trachea and obstructed by the narrowed portion of trachea at the level of vascular ring.[5] Hence, FB confirmation of ETT tip position is helpful, and ETT should be secured firmly by adhesive plaster or thread.
The case emphasizes the suspicion for vascular ring due to DAA in children with repeated pneumonia, stridor, dysphagia and aspiration when other common etiologies were excluded. Strategic planning for airway management, selection of anesthetics, ventilation during thoracotomy, weaning from the ventilator for tracheal extubation are key concerns for administering anesthesia in DAA patients.
ACKNOWLEDGMENT
Department of Cardiac Radiology, AIIMS for helping to develop the images.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Fraser CD, Jr, Carberry KE. Townsend CM, Jr, Beauchamp RD, Evers BM, Mattox KL. Sabiston Textbook of Surgery. 19th ed. Ch. 59. Philadelphia, PA: Saunders; 2012. Congenital heart disease. [Google Scholar]
- 2.Pandit BN, Kurien S, Gupta MD, Palleda GM, Tyagi S. Balanced double aortic arch with tetralogy of Fallot. Egypt Heart J. 2014;66:287–8. [Google Scholar]
- 3.Takazawa S, Uchida H, Kawashima H, Tanaka Y, Sato K, Jimbo T, et al. Massive hemorrhage after Kasai portoenterostomy in a patient with a congenital extrahepatic portosystemic shunt, malrotation and a double aortic arch: Report of a case. Surg Today. 2014;44:1561–4. doi: 10.1007/s00595-013-0605-6. [DOI] [PubMed] [Google Scholar]
- 4.Becit N, Erkut B, Karaca Y. Vascular ring: Tracheoesophageal compression associated with symmetrical double aortic arch. Tex Heart Inst J. 2008;35:209–10. [PMC free article] [PubMed] [Google Scholar]
- 5.Umegaki T, Sumi C, Nishi K, Ikeda S, Shingu K. Airway management in an infant with double aortic arch. J Anesth. 2010;24:117–20. doi: 10.1007/s00540-009-0850-4. [DOI] [PubMed] [Google Scholar]