

Abstract
Background:
Most studies examining the safety and efficacy of transphyseal anterior cruciate ligament (ACL) reconstruction for skeletally immature patients utilize transtibial drilling. Independent femoral tunnel drilling may impart a different pattern of distal femoral physeal involvement.
Purpose:
To radiographically assess differences in distal femoral physeal disruption between transtibial and independent femoral tunnel drilling. We hypothesized that more oblique tunnels associated with independent drilling involve a significantly larger area of physeal disruption compared with vertically oriented tunnels.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
We analyzed skeletally immature patients aged between 10 and 15 years who underwent transphyseal ACL reconstruction utilizing an independent femoral tunnel drilling technique between January 1, 2008, and March 31, 2011. These patients were matched with a transtibial technique cohort based on age and sex. Radiographic measurements were recorded from preoperative magnetic resonance imaging and postoperative radiographs.
Results:
Ten patients in each group were analyzed. There were significant differences between independent drilling and transtibial drilling cohorts in the estimated area of physeal disruption (1.64 vs 0.74 cm2; P < .001), femoral tunnel angles (32.1° vs 72.8°; P < .001), and medial/lateral location of the femoral tunnel (24.2 vs 36.1 mm from lateral cortex; P = .001), respectively. There was a significant inverse correlation between femoral tunnel angle and estimated area of distal femoral physeal disruption (r = –0.8255, P = .003).
Conclusion:
Femoral tunnels created with an independent tunnel drilling technique disrupt a larger area of the distal femoral physis and create more eccentric tunnels compared with a transtibial technique.
Clinical Relevance:
As most studies noting the safety of transphyseal ACL reconstruction have utilized a central, vertical femoral tunnel, surgeons should be aware that if an independent femoral tunnel technique is utilized during transphyseal ACL reconstruction, more physeal tissue is at risk and tunnels are more eccentrically placed across the physis when drilling at more horizontal angles. Prior studies have shown that greater physeal involvement and eccentric tunnels may increase the risk of growth disturbance.
Keywords: anterior cruciate ligament, knee, physis, pediatric sports medicine, athlete
The past decade has seen a sharp increase in the diagnosis and treatment of pediatric anterior cruciate ligament (ACL) injuries, and there is increasing interest in acute ACL reconstruction in this patient population.5,25,27,39 Many techniques have been described for ACL reconstruction in skeletally immature patients.6,9,28 Transphyseal ACL reconstruction involves drilling bone tunnels across an open physis and fixing a soft tissue graft away from the physis. Although multiple case series have noted transphyseal ACL reconstruction to be safe and effective,3,4,8,12,20,21,33 some animal studies have described limb shortening, deformity, and growth arrest after transphyseal tunnel placement, especially in relatively large tunnels and tunnels placed eccentrically through the physis.7,10,11,26 Clinically, some authors have also noted cases of growth arrest after transphyseal ACL reconstruction.19,22,35
Most published series that note low rates of growth disturbance with transphyseal ACL reconstruction utilize a transtibial drilling technique and have vertically oriented femoral tunnels.3,4,8,12,17,20,21,33 Recent literature has suggested that oblique, anatomically placed femoral tunnels more accurately restore normal knee biomechanics, particularly with simulated Lachman and pivot-shift testing.1,15,28,37,38 Many surgeons are therefore choosing independent femoral tunnel drilling techniques to achieve a more anatomic graft placement and thus are creating more obliquely oriented tunnels. However, in skeletally immature patients, utilizing an independent drilling technique may result in the femoral tunnel being placed more eccentrically across the distal femoral physis, exiting closer to the perichondrial ring, and potentially drilling across a larger area of the physis, thus increasing the potential risk of physeal damage.34
The purpose of this study was to evaluate differences in the radiographic pattern of physeal involvement in a cohort of pediatric patients who underwent transphyseal ACL reconstruction utilizing 2 different femoral tunnel drilling techniques: transtibial or independent. We hypothesized that tunnels created via an independent femoral drilling technique would be more obliquely oriented and more eccentrically placed across the distal femoral physis compared with the transtibial technique. Additionally, we hypothesized that the estimated percentage of the distal femoral physeal area involved would be greater in more obliquely oriented tunnels compared with vertical tunnels.
Methods
Inclusion Criteria
This study was approved by the institutional review board at our institution. All patients aged between 10 and 15 years who underwent ACL reconstruction at a large, urban, tertiary-care children’s hospital from May 2009 to June 2011 were identified. There were a total of 108 ACL reconstructions performed in this age group, with 102 reconstructions performed utilizing a transphyseal technique. During this period, the preferred surgical technique for transphyseal ACL reconstruction at our institution evolved from transtibial to independent femoral tunnel drilling. Patients were included if they (1) underwent transphyseal ACL reconstruction utilizing an outside-in, independent femoral tunnel drilling technique; (2) had preoperative magnetic resonance imaging (MRI) and 3-month postoperative plain radiographs (per our normal postoperative protocol); and (3) had not undergone prior ACL reconstruction. Ten patients met the inclusion criteria and were subsequently matched by age (chronologic) and sex with a cohort of patients who underwent transtibial femoral tunnel drilling during the same time period. Graft fixation differed between the 2 cohorts. Crosspin fixation was used for the transtibial tunnel cohort and suspensory fixation was used for the independent tunnel cohort.
Data Collection
Demographic characteristics, including age and sex, were collected. Information regarding patient surgery was recorded with particular attention paid to surgical reconstruction technique, method of femoral tunnel creation, and femoral drill/reamer diameters.
All radiographic measurements were analyzed utilizing iSite Enterprise PACS software (Philips) and were measured by 1 blinded study investigator (N.L.; although true blinding was difficult because of different fixation methods used between the 2 cohorts). Preoperative baseline MRI was utilized to determine the estimated total cross-sectional area of the femoral physis for each patient. This was accomplished by tracing a custom region of interest (ROI) along the physeal border of axial images. Postoperative plain radiographs were then used to measure the width (anteroposterior [AP] films) and length (lateral films) of the portion of physis that was removed via the formation of the femoral tunnel. The estimated area of physis removed was calculated utilizing the geometric equation for area of an ellipse (π·a·b, where a is the length of the semi–major axis and b is the length of the semi–minor axis). The percentage of the total physeal area removed was subsequently calculated. Additional data including the angle of the femoral tunnel (relative to the femoral condyles) and location of the center of the femoral tunnel (to estimate tunnel eccentricity) were collected (Figure 1).
Figure 1.
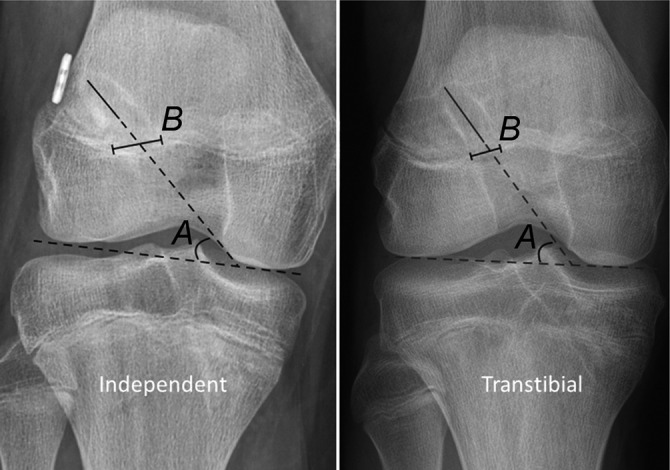
Anteroposterior knee radiographs depicting the angle of the femoral tunnel in relation to the femoral condyles, A, and the femoral tunnel width at the level of the physis, B.
Statistical Analysis
Percentage of total estimated physeal area removed, femoral tunnel angles, and medial/lateral location of the femoral tunnel at the level of the physis were compared between the transtibial and independent tunnel groups using independent-samples Student’s t tests. After ensuring data normality, the Pearson correlation coefficient was used to characterize the relationship between femoral tunnel angle and estimated percentage area of femoral physeal involvement. All statistical analyses were performed using SPSS Statistics 22 (IBM Corp). All comparative analyses were 2-tailed, and statistical significance was set at P < .05. Because this study used all available patients, an a priori power analysis was not appropriate and therefore not performed.
Results
Ten patients who underwent independent femoral tunnel drilling were age- and sex-matched with a cohort of 10 patients who underwent transtibial drilling. The mean age of the patients at the time of surgery was similar in both groups (14.65 ± 0.75 years for the transtibial group, 14.72 ± 0.77 years for the independent group; P = .92). There were 5 males and 5 females in each group. The mean knee size was also roughly the same, with a mean physeal area of 34.04 ± 3.60 cm2 in the transtibial group and 33.4 ± 3.62 cm2 in the independent group (P = .38). The mean size of the femoral reamer used to create the tunnel measured 9.1 ± 0.81 mm in the transtibial group and 9.2 ± 0.85 mm in the independent cohort (P = .92).
Femoral tunnels drilled with a transtibial technique were more vertical than tunnels drilled with an independent technique; the angle relative to the transcondylar axis was 72.8° versus 32.1°, respectively (P < .001). The measured width of the tunnel at the level of the physis on the AP radiograph was significantly smaller in the transtibial tunnel group compared with those drilled using an independent technique (1.08 vs 1.91 cm; P < .001). The measured length of the tunnel across the physis on the lateral radiograph was not significantly different in the transtibial group compared with the independent tunnel group (0.85 vs 1.07 cm; P = .139). The estimated area of physeal involvement was calculated and compared with the area of the physis from the preoperative MRI to estimate the percentage of physeal disruption. The mean estimated total area of physeal disruption was significantly smaller in the transtibial group compared with the independent tunnel group (0.74 vs 1.64 cm2, respectively; P < .001). The estimated mean percentage area of physeal disruption was also significantly smaller in the transtibial group compared with the independent group (2.11% vs 4.93%, respectively; P < .001). Table 1 summarizes the anatomic measurements.
TABLE 1.
Anatomic Measurements
| Transtibial Group (n = 10) | Independent Group (n = 10) | P Valuea | |
|---|---|---|---|
| Initial physeal area, cm2 | 34.04 | 33.4 | .72 |
| Femoral tunnel angle, deg | 72.8 | 32.1 | <.001 |
| Plain radiograph measurements, cm | |||
| Width of femoral tunnel | 1.08 | 1.91 | <.001 |
| Length of femoral tunnel | 0.85 | 1.07 | .139 |
| Physeal disruption | |||
| Area of physis removed, cm2 | 0.74 | 1.64 | <.001 |
| % of physis removed | 2.11 | 4.93 | <.001 |
| Medial/lateral location of the femoral tunnel (distance from lateral cortex), mm | 36.1 | 24.2 | .001 |
aIndependent-samples Student’s t test.
To assess the eccentricity in the location of the femoral tunnel at the level of the physis, the medial/lateral location of the femoral tunnel was calculated. The transtibial tunnels were more centrally located than the independently drilled tunnels (36.1 vs 24.2 mm from lateral cortex; P = .001).
More horizontal tunnels were associated with greater estimated percentage area of physeal disruption. There was a significant inverse correlation between femoral tunnel drill angle and estimated area of femoral physeal involvement (r = –0.8255, Pearson correlation coefficient; P = .003) (Figure 2).
Figure 2.

Scatterplot depicting the relationship between the drill angle of the femoral tunnel (x-axis) and estimated percentage of physeal area that was removed (y-axis). There was a significant inverse correlation between femoral tunnel drill angle and estimated area of femoral physeal involvement (r = –0.8255, P = .003).
Discussion
The optimal technique for surgically treating ACL tears in the skeletally immature population continues to be controversial, and the potential for physeal damage, which may result in growth arrest and/or subsequent deformity, remains a concern.10,23 Alternative reconstruction techniques, such as all-epiphyseal ACL reconstruction, in which the physes are theoretically not compromised by drilling, have been developed to address some of these concerns.2,24 However, ACL reconstruction utilizing transphyseal tunnels with a soft tissue graft remains a commonly used approach. Most studies demonstrating the safety and efficacy of transphyseal ACL reconstruction have utilized femoral tunnels drilled across the distal femoral physis via a transtibial drilling technique.3,4,8,12,17,18,20,21,33 Recent literature has suggested that independent femoral tunnel drilling may allow for more anatomic placement of the graft within the native ACL footprint and thus more accurately restore normal knee biomechanics compared with transtibial drilling techniques. Because of this, many surgeons have adopted independent femoral tunnel drilling. The main finding in this study is that transphyseal ACL reconstruction performed with an independent drilling technique was associated with significantly greater estimated damage to the physis and more eccentrically placed tunnels compared with transtibial techniques.
Prior studies examining transtibial versus independent femoral tunnel drilling in adults have also noted differences in the morphology of the femoral tunnel. Osti et al31 examined 100 patients undergoing single-bundle ACL reconstruction utilizing transtibial (TT), anteromedial (AM), or outside-in (OI) femoral tunnel drilling. The authors found that OI drilling produced more oblique femoral tunnel orientations compared with the TT technique. Tasdemir et al40 retrospectively reviewed 44 adult patients who had undergone ACL reconstruction using either an AM or a TT femoral tunnel drilling technique. While the authors used a slightly different method of estimating the femoral tunnel angle compared with the current investigation, they also showed significant differences in tunnel obliquity between independent and transtibial tunnel drilling. Using adult cadavers, Tompkins et al41 showed that femoral tunnels drilled with an independent anteromedial portal technique were more “horizontal” in the coronal plane (relative to the tibial plateau) than tunnels drilled via a transtibial technique (42.1° vs 60.9°, respectively; P < .001).
Prior studies have estimated the potential for physeal injury during ACL reconstruction in skeletally immature patients utilizing computer-modeling techniques. Shea et al34 examined 3-dimensional (3D) MRI scans of 10 pediatric knees and estimated the volume of physeal injury after simulated drilling of various diameter tunnels. The authors showed that the mean estimated percentage of distal femoral physeal involvement was 5.40% with a simulated 9-mm-diameter drill, and although they simulated drilling an independent anteromedial tunnel, the authors did not investigate the effect of altering tunnel angle via various femoral tunnel drilling techniques. Kercher et al16 also used 3D modeling of the distal femoral and proximal tibial physes to estimate the mean volume of physis removed after simulated transphyseal tunnel drilling. The authors simulated ACL tunnel drilling in 3D MRI models of 31 skeletally immature patients to estimate the volume of physis removed relative to graft diameter as well as tunnel trajectory (ie, angle). In addition to increased graft diameter, the authors found that decreasing tunnel drill angle within the proximal tibia was associated with an increased amount of tibial physis removed; however, they did not examine tunnel drill angle related to the amount of distal femoral physis removed. Kachmar et al14 compared transtibial and anteromedial surgical techniques during transphyseal ACL reconstruction utilizing 3D MRI in simulated patients. Similar to the present study, the authors found that independent (anteromedial) tunnel drilling was more likely to remove a larger volume of physis as well as violate the physis at a more eccentric location (more lateral).14 Osier et al30 used computed tomography scans to compare distal femoral physeal scar defects between independent and transtibial femoral tunnel drilling in 10 adult cadaveric knees (5 each group). The authors found that independent tunnel drilling created larger and more lateral tunnel defects at the level of the physeal scar compared with transtibial drilling.
Thus, while computer and cadaveric modeling has suggested that more horizontal tunnels may remove more physeal tissue, to the authors’ knowledge, this relationship has not been studied in a clinical cohort. The results presented in this study demonstrate that transphyseal femoral tunnels created with an independent technique create tunnels that are more oblique and thus may affect a greater percentage of physeal area than those drilled more vertically via a transtibial approach. In animal models, larger areas of physeal damage (>7% total area) may be associated with increased risk of growth disturbance.13,26,36 In this study, we found that the estimated percentage of distal femoral physeal area involvement was inversely correlated with the femoral tunnel drill angle (see Figure 2). Although only 1 patient in our series had a >7% area of estimated physeal damage, because of the findings of this study, the authors suggest that surgeons exercise caution when creating obliquely oriented, transphyseal femoral tunnels in skeletally immature patients. Alternatively, femoral physeal injury with an all-epiphyseal technique has been shown to be minimal and may offer another way to minimize damage to the physis.29 In the absence of long-term clinical data evaluating the relationship between tunnel diameter/inclination angle and distal femoral physeal growth disturbance, these data would suggest that when performing transphyseal ACL reconstruction, surgeons should consider using drilling techniques that minimize the obliquity of the femoral tunnel as it is drilled across the physis, for example, drilling more vertical tunnels via an independent outside-in technique.
The other major difference with more oblique femoral tunnels is the eccentricity of the potential physeal damage. Tunnels that were drilled using an independent technique were significantly more eccentrically located compared with those drilled via a transtibial technique (see Table 1). This may have implications in patients with significant growth remaining since eccentrically placed drill holes within the femoral (or tibial) physes are known to have increased risk of growth arrest and/or development of angular deformity.7,32
Limitations
This investigation has several limitations. Other studies have used 3D computer modeling to accurately calculate physeal damage during simulated ACL reconstruction. However, our study utilized 2-dimensional and axial imaging only and thus should be interpreted as an estimate of physeal damage. While computer modeling may provide a more precise approximation of physeal involvement, modeling is performed on “ideal” tunnels and not on the real-life application of a technique. We also used a single observer to obtain measurements, and while the observer was blinded to the surgical technique used, inherent differences in postsurgical radiographs had the potential to bias measurements. Although the methods used in the current study are likely less accurate than would be possible with postoperative 3D imaging, they were measured in a clinical cohort, utilized techniques that are readily available in the clinical setting, and thus may confirm the results from prior simulation studies.
This study was a retrospective review and may be affected by selection bias. However, we strictly defined our patient cohort and included all skeletally immature patients who underwent transphyseal ACL reconstruction during a specified time period via an independent femoral tunnel drilling technique. These patients were then age- and sex-matched with those who underwent transtibial drilling during the same time period to provide a matched cohort for comparison. This study also examines a relatively small cohort of patients but did not suffer from lack of power as evidenced by the statistical significance of our primary and secondary outcomes. With these positive findings, there could not have been a type II error, which would be a concern of any study that is potentially underpowered.
The independent tunnel cohort examined in this study represented our institution’s early experience with independent tunnel drilling. In this study, it is important to note that independent tunnel drilling was essentially a marker for horizontal tunnel orientation. Based on these data, we cannot advocate for or against a particular technique of femoral tunnel drilling (independent vs transtibial) during pediatric transphyseal ACL reconstruction. Whether there is a difference in clinical outcomes or growth disturbance between the 2 techniques was not investigated in this study. Rather, we estimate that tunnels drilled at greater angles relative to the transcondylar axis of the femur involve less area of the distal femoral physis. This can be true regardless of drilling technique. Relatively vertical tunnels can be created using an independent drilling technique and relatively horizontal tunnels can be created with modified transtibial techniques. Therefore, the results of this study confirm previous findings that obliquely drilled transphyseal tunnels may involve a greater area of physis and that surgeons should be aware of this during transphyseal ACL reconstruction regardless of femoral tunnel drilling technique.
Conclusion
Transphyseal ACL reconstruction is an accepted reconstruction technique for skeletally immature patients with minimal remaining growth and has been shown to be both safe and effective. The safety of this technique, however, is predicated on the fact that the femoral tunnel is vertically oriented, and most descriptions of transphyseal ACL reconstruction have utilized a transtibial approach to femoral tunnel drilling. Compared with transtibial femoral tunnel drilling, independent tunnel drilling techniques create more oblique femoral tunnels. Surgeons should be aware that increased tunnel obliquity is associated with greater area of physeal disruption and more eccentrically placed tunnels at the level of the physis. Femoral tunnel obliquity should therefore be minimized as much as possible to limit physeal disruption during transphyseal ACL reconstruction.
Footnotes
The authors reported that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Abebe ES, Utturkar GM, Taylor DC, et al. The effects of femoral graft placement on in vivo knee kinematics after anterior cruciate ligament reconstruction. J Biomech. 2011;44:924–929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Anderson AF. Transepiphyseal replacement of the anterior cruciate ligament in skeletally immature patients. A preliminary report. J Bone Joint Surg Am. 2003;85–A: 1255–1263. [DOI] [PubMed] [Google Scholar]
- 3. Calvo R, Figueroa D, Gili F, et al. Transphyseal anterior cruciate ligament reconstruction in patients with open physes: 10-year follow-up study. Am J Sports Med. 2015;43:289–294. [DOI] [PubMed] [Google Scholar]
- 4. Cohen M, Ferretti M, Quarteiro M, et al. Transphyseal anterior cruciate ligament reconstruction in patients with open physes. Arthroscopy. 2009;25:831–838. [DOI] [PubMed] [Google Scholar]
- 5. Dodwell ER, Lamont LE, Green DW, Pan TJ, Marx RG, Lyman S. 20 years of pediatric anterior cruciate ligament reconstruction in New York State. Am J Sports Med. 2014;42:675–680. [DOI] [PubMed] [Google Scholar]
- 6. Fabricant PD, Jones KJ, Delos D, et al. Reconstruction of the anterior cruciate ligament in the skeletally immature athlete: a review of current concepts: AAOS exhibit selection. J Bone Joint Surg Am. 2013;95:e28. [DOI] [PubMed] [Google Scholar]
- 7. Ford LT, Key JA. A study of experimental trauma to the distal femoral epiphysis in rabbits. J Bone Joint Surg Am. 1956;38–A: 84–92. [PubMed] [Google Scholar]
- 8. Frosch KH, Stengel D, Brodhun T, et al. Outcomes and risks of operative treatment of rupture of the anterior cruciate ligament in children and adolescents. Arthroscopy. 2010;26:1539–1550. [DOI] [PubMed] [Google Scholar]
- 9. Gausden EB, Calcei JG, Fabricant PD, Green DW. Surgical options for anterior cruciate ligament reconstruction in the young child. Curr Opin Pediatr. 2015;27:82–91. [DOI] [PubMed] [Google Scholar]
- 10. Guzzanti V, Falciglia F, Gigante A, Fabbriciani C. The effect of intra-articular ACL reconstruction on the growth plates of rabbits. J Bone Joint Surg Br. 1994;76:960–963. [PubMed] [Google Scholar]
- 11. Houle JB, Letts M, Yang J. Effects of a tensioned tendon graft in a bone tunnel across the rabbit physis. Clin Orthop Relat Res. 2001;391:275–281. [DOI] [PubMed] [Google Scholar]
- 12. Hui C, Roe J, Ferguson D, Waller A, Salmon L, Pinczewski L. Outcome of anatomic transphyseal anterior cruciate ligament reconstruction in Tanner stage 1 and 2 patients with open physes. Am J Sports Med. 2012;40:1093–1098. [DOI] [PubMed] [Google Scholar]
- 13. Janarv PM, Wikstrom B, Hirsch G. The influence of transphyseal drilling and tendon grafting on bone growth: an experimental study in the rabbit. J Pediatr Orthop. 1998;18:149–154. [PubMed] [Google Scholar]
- 14. Kachmar M, Piazza SJ, Bader DA. Comparison of growth plate violations for transtibial and anteromedial surgical techniques in simulated adolescent anterior cruciate ligament reconstruction. Am J Sports Med. 2016;44:417–424. [DOI] [PubMed] [Google Scholar]
- 15. Keller TC, Tompkins M, Economopoulos K, et al. Tibial tunnel placement accuracy during anterior cruciate ligament reconstruction: independent femoral versus transtibial femoral tunnel drilling techniques. Arthroscopy. 2014;30:1116–1123. [DOI] [PubMed] [Google Scholar]
- 16. Kercher J, Xerogeanes J, Tannenbaum A, Al-Hakim R, Black JC, Zhao J. Anterior cruciate ligament reconstruction in the skeletally immature: an anatomical study utilizing 3-dimensional magnetic resonance imaging reconstructions. J Pediatr Orthop. 2009;29:124–129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Kim SJ, Shim DW, Park KW. Functional outcome of transphyseal reconstruction of the anterior cruciate ligament in skeletally immature patients. Knee Surg Relat Res. 2012;24:173–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Kocher MS, Hovis WD, Curtin MJ, Hawkins RJ. Anterior cruciate ligament reconstruction in skeletally immature knees: an anatomical study. Am J Orthop (Belle Mead NJ). 2005;34:285–290. [PubMed] [Google Scholar]
- 19. Kocher MS, Saxon HS, Hovis WD, Hawkins RJ. Management and complications of anterior cruciate ligament injuries in skeletally immature patients: survey of the Herodicus Society and the ACL Study Group. J Pediatr Orthop. 2002;22:452–457. [PubMed] [Google Scholar]
- 20. Kocher MS, Smith JT, Zoric BJ, Lee B, Micheli LJ. Transphyseal anterior cruciate ligament reconstruction in skeletally immature pubescent adolescents. J Bone Joint Surg Am. 2007;89:2632–2639. [DOI] [PubMed] [Google Scholar]
- 21. Kohl S, Stutz C, Decker S, et al. Mid-term results of transphyseal anterior cruciate ligament reconstruction in children and adolescents. Knee. 2014;21:80–85. [DOI] [PubMed] [Google Scholar]
- 22. Koman JD, Sanders JO. Valgus deformity after reconstruction of the anterior cruciate ligament in a skeletally immature patient. A case report. J Bone Joint Surg Am. 1999;81:711–715. [DOI] [PubMed] [Google Scholar]
- 23. Larsen MW, Garrett WE, Jr, Delee JC, Moorman CT., 3rd Surgical management of anterior cruciate ligament injuries in patients with open physes. J Am Acad Orthop Surg. 2006;14:736–744. [DOI] [PubMed] [Google Scholar]
- 24. Lawrence JT, Bowers AL, Belding J, Cody SR, Ganley TJ. All-epiphyseal anterior cruciate ligament reconstruction in skeletally immature patients. Clin Orthop Relat Res. 2010;468:1971–1977. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Luhmann SJ. Acute traumatic knee effusions in children and adolescents. J Pediatr Orthop. 2003;23:199–202. [PubMed] [Google Scholar]
- 26. Makela EA, Vainionpaa S, Vihtonen K, Mero M, Rokkanen P. The effect of trauma to the lower femoral epiphyseal plate. An experimental study in rabbits. J Bone Joint Surg Br. 1988;70:187–191. [DOI] [PubMed] [Google Scholar]
- 27. Mall NA, Paletta GA. Pediatric ACL injuries: evaluation and management. Curr Rev Musculoskelet Med. 2013;6:132–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Milewski MD, Beck NA, Lawrence JT, Ganley TJ. Anterior cruciate ligament reconstruction in the young athlete: a treatment algorithm for the skeletally immature. Clin Sports Med. 2011;30:801–810. [DOI] [PubMed] [Google Scholar]
- 29. Nawabi DH, Jones KJ, Lurie B, Potter HG, Green DW, Cordasco FA. All-inside, physeal-sparing anterior cruciate ligament reconstruction does not significantly compromise the physis in skeletally immature athletes: a postoperative physeal magnetic resonance imaging analysis. Am J Sports Med. 2014;42:2933–2940. [DOI] [PubMed] [Google Scholar]
- 30. Osier CJ, Espinoza-Ervin C, Diaz De Leon A, Sims G, Ellis HB L, Jr, Wilson P. A comparison of distal femoral physeal defect and fixation position between two different drilling techniques for transphyseal anterior cruciate ligament reconstruction. J Pediatr Orthop B. 2015;24:106–113. [DOI] [PubMed] [Google Scholar]
- 31. Osti M, Krawinkel A, Ostermann M, Hoffelner T, Benedetto KP. Femoral and tibial graft tunnel parameters after transtibial, anteromedial portal, and outside-in single-bundle anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43:2250–2258. [DOI] [PubMed] [Google Scholar]
- 32. Peterson HA. Partial growth plate arrest and its treatment. J Pediatr Orthop. 1984;4:246–258. [DOI] [PubMed] [Google Scholar]
- 33. Redler LH, Brafman RT, Trentacosta N, Ahmad CS. Anterior cruciate ligament reconstruction in skeletally immature patients with transphyseal tunnels. Arthroscopy. 2012;28:1710–1717. [DOI] [PubMed] [Google Scholar]
- 34. Shea KG, Belzer J, Apel PJ, Nilsson K, Grimm NL, Pfeiffer RP. Volumetric injury of the physis during single-bundle anterior cruciate ligament reconstruction in children: a 3-dimensional study using magnetic resonance imaging. Arthroscopy. 2009;25:1415–1422. [DOI] [PubMed] [Google Scholar]
- 35. Shifflett GD, Green DW, Widmann RF, Marx RG. Growth arrest following ACL reconstruction with hamstring autograft in skeletally immature patients: a review of 4 cases. J Pediatr Orthop. 2016;36:355–361. [DOI] [PubMed] [Google Scholar]
- 36. Stadelmaier DM, Arnoczky SP, Dodds J, Ross H. The effect of drilling and soft tissue grafting across open growth plates. A histologic study. Am J Sports Med. 1995;23:431–435. [DOI] [PubMed] [Google Scholar]
- 37. Steiner ME. Independent drilling of tibial and femoral tunnels in anterior cruciate ligament reconstruction. J Knee Surg. 2009;22:171–176. [DOI] [PubMed] [Google Scholar]
- 38. Steiner ME, Battaglia TC, Heming JF, Rand JD, Festa A, Baria M. Independent drilling outperforms conventional transtibial drilling in anterior cruciate ligament reconstruction. Am J Sports Med. 2009;37:1912–1919. [DOI] [PubMed] [Google Scholar]
- 39. Streich NA, Barie A, Gotterbarm T, Keil M, Schmitt H. Transphyseal reconstruction of the anterior cruciate ligament in prepubescent athletes. Knee Surg Sports Traumatol Arthrosc. 2010;18:1481–1486. [DOI] [PubMed] [Google Scholar]
- 40. Tasdemir Z, Gulabi D, Saglam F, Tokgoz Ozal S, Elmali N. Does the anteromedial portal provide clinical superiority compared to the transtibial portal in anterior cruciate ligament reconstruction in nonprofessional athletes in short-term follow-up? Acta Orthop Traumatol Turc. 2015;49:483–491. [DOI] [PubMed] [Google Scholar]
- 41. Tompkins M, Cosgrove CT, Milewski MD, Brockmeier SF, Hart JM, Miller MD. Anterior cruciate ligament reconstruction femoral tunnel characteristics using an accessory medial portal versus traditional transtibial drilling. Arthroscopy. 2013;29:550–555. [DOI] [PubMed] [Google Scholar]