

Abstract
The posterior insular cortex—a complex structure interconnecting various brain regions for different functions—is a rare location for ischemic stroke. We report a patient with isolated left posterior insular infarction who presented with multiple cognitive impairment, including impairment in semantic and phonemic verbal fluency.
The insular cortex is a hidden structure located in the Sylvian fissure surrounded by the temporal, frontal, and parietal lobes. It is a complex structure interconnecting various brain regions that contribute to autonomic, gustatory, auditory, and speech and language function as well as somatosensory perception and emotional response (1). The arteries supplying the insular area mainly originate from the M2 segment of the middle cerebral artery (2). This article presents a case of isolated left posterior insular infarction (PII) resulting in impairment in multiple cognitive domains.
CASE REPORT
An 80-year-old right-handed man with 13 years of education woke up with a speech problem. Previously, he had childhood poliomyelitis, diabetes mellitus, coronary artery disease, and hypertension. After waking up, he could not speak fluently, although his comprehension was fully preserved. He also had mild right facial drooping and right-sided weakness.
His vital signs and general exam were normal. The body mass index was 25.4 kg/m2. He had right facial weakness, word-finding difficulty, and mild dysarthria. Apart from the lower-extremity weakness from childhood poliomyelitis, he had no other motor or sensory deficits.
Magnetic resonance imaging of the head demonstrated an acute infarction in the left posterior insular cortex (Figure 1), and imaging of the neck showed approximately 50% narrowing of the proximal right internal carotid artery. Transthoracic echocardiogram and telemetry were unremarkable. Aspirin 325 mg/day and atorvastatin 40 mg/day were started.
Figure 1.

Acute left posterior insular infarction demonstrated by (a) apparent diffusion coefficient imaging and (b) diffusion-weighted imaging.
Two days later, the patient's right facial drooping, dysarthria, and word-finding difficulty completely resolved. He scored 20 out of 30 in the Montreal Cognitive Assessment (Figure 2) (3, 4). A retrieval memory deficit was detected with delayed recall of 0/5 and a Memory Index Score of 8/15 (5). He also had impairment in semantic fluency (7 words in 1 minute) and phonemic fluency (4 words in 1 minute). Impairment in repetition of complex sentences was detected. He did not demonstrate any naming problem when evaluated by the shortened Boston Naming Test (6). Based on clinical interview and the Geriatric Depression Scale (7), he did not have any affective disturbance that could impair his cognition. The Modified Rankin Scale score was 1 at discharge.
Figure 2.

The performance of this patient on the Montreal Cognitive Assessment.
DISCUSSION
Isolated PII is a rare condition. In one study, among 4800 patients with their first episode of ischemic stroke, only 4 patients (0.08%) had isolated insular infarction (8). The findings of multidomain cognitive impairment in this patient suggest that the posterior insular cortex is a convergent structure; thus, the deficits caused by PII are more likely to be the consequence of diaschisis rather than damage of a specialized or isolated center itself (Figure 3).
Figure 3.
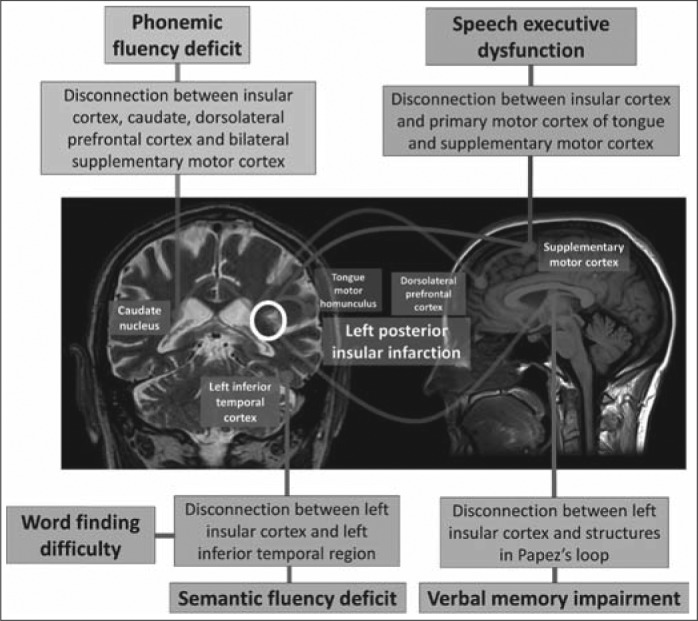
The role of the posterior insular cortex and its connecting areas in multiple cognitive domains including phonemic and semantic verbal fluency, speech executive function, language function, and verbal memory. The posterior insular cortex is a convergent structure connecting with multiple brain regions; thus, the deficits caused by posterior insular infarction are more likely to be the consequence of diaschisis than damage to a specialized or isolated center.
Due to the complexity of the cognitive process, it is challenging to draw conclusions about the role of the insular cortex in speech production. In one study, the anterior insular cortex was a common area of infarction in all 25 stroke cases with disorder of motor planning in articulation (9). Left PII was previously reported to cause both dysarthria and aphasia in a single case (8). The insular cortex is activated in the phonological process during reading in functional magnetic resonance imaging (10). Executive function is also required in planning of articulation. Therefore, PII may cause a disconnection between the primary and supplementary motor cortex, leading to executive dysfunction of motor speech (8, 11).
The insular cortex is associated with gustatory, visual, and verbal memory (12–14). Patients with a left insular stroke have more impairment in verbal memory and logical memory than patients with a right insular stroke (13). The disruption of the connection between the left temporal lobe and the left insular cortex may play a role in this deficit. Positron emission tomography in healthy volunteers showed a correlation between cerebral blood flow in the insular cortex and the verbal memory task (15). Improvement with cue may imply that the memory impairment was primarily from deficits in retrieval of the previously registered information, not the encoding process.
Phonemic fluency is primarily mediated by the frontal lobe, while semantic fluency requires lexicosemantic memory, which is functioned mainly by the temporal cortex. In 48 patients with a left-hemisphere stroke, voxel-based lesion symptom mapping showed the association between the phonemic fluency task and the insular cortex lesion (16). The left anterior insular infarction was reported to cause executive dysfunction, including impairment of semantic and phonemic fluency, which may be a result of neuronal network disruption between the anterior insula and frontal lobe and/or cingulate regions (17). To the best of our knowledge, this is the first report of a verbal fluency deficit in a patient with an isolated left PII. Since the posterior insular cortex is adjacent to the semantic storage areas, this infarction may cause network disconnection between these areas, resulting in difficulty retrieving previously learned knowledge.
Even though various types of aphasia were reported in strokes involving the insular cortex (8, 18, 19), pure insular infarction with aphasia is very uncommon. Anatomically, the insular lobe is in the central part of the structures that are important in language functions, including the frontal operculum and Wernicke's area. The disconnection of these structures and insular area may contribute to language dysfunction after insular damage.
The prognosis of the isolated insular infarction is favorable. In a case series, more than half of patients with isolated insular infarction or minimal extension to adjacent areas completely recovered or had minimal deficits within 48 hours, and all had a Modified Rankin Scale score of 0 to 2 at 6 months (18).
References
- 1.Ibañez A. Gleichgerrcht E. Manes F. Clinical effects of insular damage in humans. Brain Struct Funct. 2010;214(5–6):397–410. doi: 10.1007/s00429-010-0256-y. [DOI] [PubMed] [Google Scholar]
- 2.Türe U. Yaşargil MG. Al-Mefty O. Yaşargil DC. Arteries of the insula. J Neurosurg. 2000;92(4):676–687. doi: 10.3171/jns.2000.92.4.0676. [DOI] [PubMed] [Google Scholar]
- 3.Nasreddine ZS. Phillips NA. Bédirian V. Charbonneau S. Whitehead V. Collin I. Cummings JL. Chertkow H. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi: 10.1111/j.1532-5415.2005.53221.x. [DOI] [PubMed] [Google Scholar]
- 4.Julayanont P. Phillips N. Chertkow H. Nasreddine ZS. Larner AJ. Cognitive Screening Instruments. London: Springer; 2013. Montreal Cognitive Assessment (MoCA): concept and clinical review; pp. 111–151. [Google Scholar]
- 5.Julayanont P. Brousseau M. Chertkow H. Phillips N. Nasreddine ZS. Montreal Cognitive Assessment Memory Index Score (MoCA-MIS) as a predictor of conversion from mild cognitive impairment to Alzheimer's disease. J Am Geriatr Soc. 2014;62(4):679–684. doi: 10.1111/jgs.12742. [DOI] [PubMed] [Google Scholar]
- 6.Mack WJ. Freed DM. Williams BW. Henderson VW. Boston Naming Test: shortened versions for use in Alzheimer's disease. J Gerontol. 1992;47(3):154–158. doi: 10.1093/geronj/47.3.p154. [DOI] [PubMed] [Google Scholar]
- 7.Yesavage JA. Brink TL. Rose TL. Lum O. Huang V. Adey M. Leirer VO. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982–1983;17(1):37–49. doi: 10.1016/0022-3956(82)90033-4. [DOI] [PubMed] [Google Scholar]
- 8.Cereda C. Ghika J. Maeder P. Bogousslavsky J. Strokes restricted to the insular cortex. Neurology. 2002;59(12):1950–1955. doi: 10.1212/01.wnl.0000038905.75660.bd. [DOI] [PubMed] [Google Scholar]
- 9.Dronkers NF. A new brain region for coordinating speech articulation. Nature. 1996;384(6605):159–161. doi: 10.1038/384159a0. [DOI] [PubMed] [Google Scholar]
- 10.Borowsky R. Cummine J. Owen WJ. Friesen CK. Shih F. Sarty GE. FMRI of ventral and dorsal processing streams in basic reading processes: insular sensitivity to phonology. Brain Topogr. 2006;18(4):233–239. doi: 10.1007/s10548-006-0001-2. [DOI] [PubMed] [Google Scholar]
- 11.Baier B. zu Eulenburg P. Glassl O. Dieterich M. Lesions to the posterior insular cortex cause dysarthria. Eur J Neurol. 2011;18(12):1429–1431. doi: 10.1111/j.1468-1331.2011.03473.x. [DOI] [PubMed] [Google Scholar]
- 12.Suto T. Meguro K. Nakatsuka M. Kato Y. Tezuka K. Yamaguchi S. Tashiro M. Disorders of “taste cognition” are associated with insular involvement in patients with Alzheimer's disease and vascular dementia: “memory of food is impaired in dementia and responsible for poor diet. Int Psychogeriatr. 2014;26(7):1127–1138. doi: 10.1017/S1041610214000532. [DOI] [PubMed] [Google Scholar]
- 13.Manes F. Springer J. Jorge R. Robinson RG. Verbal memory impairment after left insular cortex infarction. J Neurol Neurosurg Psychiatry. 1999;67(4):532–534. doi: 10.1136/jnnp.67.4.532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.O’Brien LD. Sticht MA. Mitchnick KA. Limebeer CL. Parker LA. Winters BD. CB1 receptor antagonism in the granular insular cortex or somatosensory area facilitates consolidation of object recognition memory. Neurosci Lett. 2014;578:192–196. doi: 10.1016/j.neulet.2014.06.056. [DOI] [PubMed] [Google Scholar]
- 15.Grasby PM. Frith CD. Friston KJ. Simpson J. Fletcher PC. Frackowiak RS. Dolan RJ. A graded task approach to the functional mapping of brain areas implicated in auditory-verbal memory. Brain. 1994;117(Pt 6):1271–1282. doi: 10.1093/brain/117.6.1271. [DOI] [PubMed] [Google Scholar]
- 16.Baldo JV. Schwartz S. Wilkins D. Dronkers NF. Role of frontal versus temporal cortex in verbal fluency as revealed by voxel-based lesion symptom mapping. J Int Neuropsychol Soc. 2006;12(6):896–900. doi: 10.1017/S1355617706061078. [DOI] [PubMed] [Google Scholar]
- 17.Markostamou I. Rudolf J. Tsiptsios I. Kosmidis MH. Impaired executive functioning after left anterior insular stroke: a case report. Neurocase. 2015;21(2):148–153. doi: 10.1080/13554794.2013.878725. [DOI] [PubMed] [Google Scholar]
- 18.Lemieux F. Lanthier S. Chevrier M-C. Gioia L. Rouleau I. Cereda C. Nguyen DK. Insular ischemic stroke: clinical presentation and outcome. Cerebrovasc Dis Extra. 2012;2(1):80–87. doi: 10.1159/000343177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Carota A. Annoni J-M. Marangolo P. Repeating through the insula: evidence from two consecutive strokes. Neuroreport. 2007;18(13):1367–1370. doi: 10.1097/WNR.0b013e328277ef72. [DOI] [PubMed] [Google Scholar]