

Abstract
A 22-year-old man was hospitalized with a sternoclavicular joint (SCJ) dislocation caused by a traffic accident. Surgical reduction and fixation of the SCJ were performed using a T-plate. SCJ dislocation is rare, accounting for less than 1% of all dislocations, and is usually treated conservatively, although severe cases may require surgery. Surgery typically involves joint reduction and fixation using an autologous tendon graft, but this has disadvantages such as the requirement for additional surgery to obtain autologous tissue and an extended operative time. To overcome these issues, here, we performed a simple SCJ reduction and fixation using a T-plate and achieved good results.
Keywords: Sternum, T-plate
A 22-year-old man was hospitalized with anterior thoracic wall pain that occurred after he became caught between two automobiles during work. His vital signs were good at the time of hospitalization, and there were no specific physical findings on either arm except for impaired movement. A simple thoracic radiograph showed no signs of thoracic wall or clavicle fracture but confirmed a dislocation of the manubrioclavicular junction (Fig. 1). No organ injury was observed on a three-dimensional chest computed tomography scan, but a hematoma near the sternoclavicular joint (SCJ) and posterior dislocation of the manubrium were noted (Fig. 1). The patient chose surgical treatment because he had persistent severe pain in his arms and was unable to elevate them completely. Surgery was performed in a supine position. After exposing the sternum with a midline vertical incision from the sternal notch to a point 2 cm inferior to the Louis angle, an SCJ manual reduction was performed; while hyperextension of the Louis angle was maintained, T-plate fixation of the manubrium and sternal body was performed and the operation was completed (Fig. 2). After surgery, at the time of discharge, the patient was advised to use slings on both arms to maintain SCJ stabilization. Outpatient examination 6 months after the surgery revealed that the patient was pain free and showed normal bilateral movement of the arms (Fig. 3).
Fig. 1.

Dislocated sternoclavicular joint on lateral view. (A) Angle of Louis 160′ and (B) reconstruction view on computed tomography.
Fig. 2.

(A) Dislocation of SCJ and clavicle head (*) at intraoperation. (B) Reduction SCJ & fixation of Louis angle with T-plate. SCJ, sternoclavicular joint.
Fig. 3.
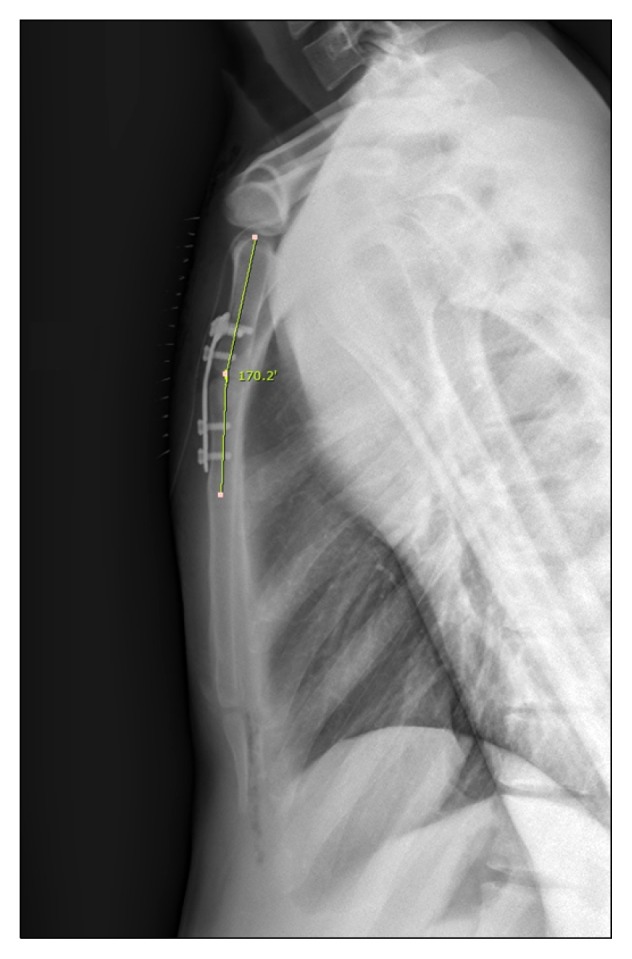
Lateral view of postoperation (angle of Louis 170′).
SCJ dislocation is rare, accounting for less than 1% of all dislocations, and the majority of cases reportedly occur due to traffic accidents [1]. They can be divided into anterior and posterior dislocations, the latter of which is much rarer, and can be accompanied by fatal structural injury [1,2]. Anterior dislocation is usually treated conservatively; however, surgical treatment can be considered for recurrent or severe dislocations [1–3]. Surgical treatment usually involves joint reduction using an autologous tendon graft and stable fixation [1–3], but it is also possible to secure unstable joint fixation using other suture materials [4].
SCJ stabilization using an autologous tendon is a larger-scale surgical procedure that requires extended operative time, and obtaining the tendon graft carries a risk of injury to other organs. Moreover, during surgery, there is a high risk of injury to the large vessels that run close to the SCJ [5].
The present surgical method reduces the risk of large vessel or organ injury during graft tissue harvesting and decreases the surgical time. However, our study findings are limited because this was the first time that we attempted the procedure, and no long-term follow-up was performed nor were comparisons with other surgical or conservative treatments made.
Footnotes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1.Guan JJ, Wolf BR. Reconstruction for anterior sternoclavicular joint dislocation and instability. J Shoulder Elbow Surg. 2013;22:775–81. doi: 10.1016/j.jse.2012.07.009. [DOI] [PubMed] [Google Scholar]
- 2.Singer G, Ferlic P, Kraus T, Eberl R. Reconstruction of the sternoclavicular joint in active patients with the figure-of-eight technique using hamstrings. J Shoulder Elbow Surg. 2013;22:64–9. doi: 10.1016/j.jse.2012.02.009. [DOI] [PubMed] [Google Scholar]
- 3.Bak K, Fogh K. Reconstruction of the chronic anterior unstable sternoclavicular joint using a tendon autograft: medium-term to long-term follow-up results. J Shoulder Elbow Surg. 2014;23:245–50. doi: 10.1016/j.jse.2013.05.010. [DOI] [PubMed] [Google Scholar]
- 4.Janson JT, Rossouw GJ. A new technique for repair of a dislocated sternoclavicular joint using a sternal tension cable system. Ann Thorac Surg. 2013;95:e53–5. doi: 10.1016/j.athoracsur.2012.10.047. [DOI] [PubMed] [Google Scholar]
- 5.Ponce BA, Kundukulam JA, Pflugner R, et al. Sternoclavicular joint surgery: how far does danger lurk below? J Shoulder Elbow Surg. 2013;22:993–9. doi: 10.1016/j.jse.2012.10.037. [DOI] [PubMed] [Google Scholar]