

Abstract
It is often difficult to differentiate gastric mucosa-associated lymphoid tissue (MALT) lymphoma from Helicobacter pylori-associated follicular gastritis, and thus, it becomes unclear how to manage these diseases. This study aimed to explore the management strategy for and the long-term outcomes of suspicious gastric MALT lymphoma detected by forceps biopsy during screening upper endoscopy. Between October 2003 and May 2013, consecutive subjects who were diagnosed with suspicious gastric MALT lymphomas by screening endoscopy in a health checkup program in Korea were retrospectively enrolled. Suspicious MALT lymphoma was defined as a Wotherspoon score of 3 or 4 upon pathological evaluation of the biopsy specimen. Of 105,164 subjects who underwent screening endoscopies, 49 patients with suspicious MALT lymphomas who underwent subsequent endoscopy were enrolled. Eight patients received a subsequent endoscopy without H. pylori eradication (subsequent endoscopy only group), and 41 patients received H. pylori eradication first followed by endoscopy (eradication first group). MALT lymphoma development was significantly lower in the eradication first group (2/41, 4.9%) than in the subsequent endoscopy only group (3/8, 37.5%, P = 0.026). Notably, among 35 patients with successful H. pylori eradication, there was only one MALT lymphoma patient (2.9%) in whom complete remission was achieved, and there was no recurrence during a median 45 months of endoscopic follow-up. H. pylori eradication with subsequent endoscopy would be a practical management option for suspicious MALT lymphoma detected in a forceps biopsy specimen obtained during screening upper endoscopy.
Keywords: Marginal Zone B-cell Lymphoma, Primary Gastric Lymphoma, Cancer Screening, Non-Hodgkin Lymphoma, Helicobacter pylori
Graphical Abstract
INTRODUCTION
Extranodal marginal zone B-cell lymphoma (MALT lymphoma) is a major type of lymphoma that arises in the stomach (1). Although primary gastric lymphomas account for only 3%–5% of gastric malignant tumors, gastric MALT lymphomas comprise nearly half of the lymphoma cases. MALT lymphomas are indolent in nature and show good responses to the eradication of Helicobacter pylori and consequent excellent prognosis in most cases (2). Histological diagnosis of MALT lymphoma is made by demonstrating the dense lymphoid infiltration occupying the lamina propria with the presence of prominent lymphoepithelial lesions (3). Although the stomach is typically devoid of lymphoid tissue, lymphoid follicles frequently develop after chronic H. pylori infection (4). Because most cases of gastric MALT lymphomas emerge from H. pylori-associated MALT, it is often difficult to differentiate these cases from H. pylori-associated follicular gastritis (5). This diagnostic ambiguity was addressed in the now widely accepted 5-grade histomorphological scoring system suggested by Wotherspoon et al. (3). Suspicious MALT lymphoma cases are categorized as a Wotherspoon score 3 (suspicious, probably reactive) or 4 (suspicious, probably neoplastic) (3).
Currently, it is not clear how to manage the lesions with Wotherspoon scores of 3 or 4 (6,7). A broadly used method to distinguish between gastritis and lymphoma is the evaluation of the clonality of B cells based on the analysis of rearranged immunoglobulin genes (8). However, the sensitivity and specificity of this method are limited (8,9), and may not be practical in some countries considering the high cost. Repeat endoscopy with extensive biopsy could also aid in making a definitive diagnosis when the initial endoscopic finding is strongly suggestive of malignancy (10,11). Another alternative would be to treat the suspicious lesion with H. pylori eradication (12,13). Although this option is practical and easy to adopt, it becomes no longer possible to differentiate between gastritis and lymphoma because both lesions respond to H. pylori eradication.
In Korea as well as in Japan, endoscopic screening for gastric cancer is widely performed (14,15). Consequently, subtle lesions with Wotherspoon scores of 3 or 4 are frequently encountered. Although a second endoscopy is conducted in some cases, the majority of patients are treated with H. pylori eradication and then followed up with endoscopy. However, there is no long-term follow-up data after H. pylori eradication for these ‘suspicious’ lesions, especially regarding the risk of MALT lymphoma development from these lesions.
Therefore, in this study, we aimed to explore a management strategy for and the long-term outcome of the suspicious gastric MALT lymphomas detected in forceps biopsy specimens obtained during screening endoscopy.
MATERIALS AND METHODS
Patients
Our data were derived from those who visited the Seoul National University Hospital (SNUH) Healthcare System Gangnam Center for their health checkups and underwent upper endoscopy screenings between October 2003 and September 2013. Those patients who received an endoscopic forceps biopsy in which histological evaluation demonstrated suspicious MALT lymphoma were included in the study. Suspicious MALT lymphoma was defined as a Wotherspoon score of 3 or 4 (3). The subjects who did not have a subsequent endoscopy within 1 year were excluded. The medical records of the patients were reviewed with regard to demographics, endoscopic tumor findings, and histological findings.
Endoscopic screening protocol and histologic evaluation
Fifteen experienced board certified gastroenterologists performed all examinations using conventional white light video endoscopy (GIF H260; Olympus, Aizu, Japan/EG-450WR5 or EG-590WR; Fujinon, Saitama, Japan). During endoscopy, biopsies were taken from any seemingly abnormal lesions using biopsy forceps. The endoscopic appearances of the lesions were classified as superficial, polypoid, thickened fold, or ulcerative, and the superficial type was further subclassified as multinodular, multifocal atrophic, or erosions based on previous studies (16,17). The dominant location of the lesion was categorized as the upper, middle, or lower third of the stomach.
All histopathological diagnosis were made by 4 pathologists specialized in gastrointestinal pathology or hematopathology with > 10 years of experience. Hematoxylin-eosin staining of biopsy samples was routinely performed for histological evaluation, and immunohistochemical staining using CD3, CD20, Ki-67, and cytokeratin was carried out in most cases (5).
H. pylori infection status
H. pylori infection status was determined by serology, histology, rapid urease testing (CLOtest, Delta West, Bentley, Australia), and 13C-urea breath testing (UBiTkit, Otsuka Pharmaceutical, Tokyo, Japan). Anti-H. pylori IgG was measured using a commercially available enzyme-linked immunosorbent assay (H. pylori-EIA-Well, Radim, Rome, Italy) for serologic testing as previously described (18), and modified Giemsa staining was used for histological testing. When any of the tests except for serology were positive, H. pylori infection was considered to be present. H. pylori infection was judged as negative only when all of the tests, including serology, were negative. Cases where only the serology test was positive were considered as examples of past H. pylori infection.
Initial management strategy, treatment, and follow-up
On the first appointment after screening endoscopy, the patients with suspicious MALT lymphoma were recommended either to undergo a subsequent endoscopy without H. pylori eradication (subsequent endoscopy only group) or to receive H. pylori eradication first and then to undergo a subsequent endoscopy (eradication first group). The attending physician for each case decided which strategy to choose. Clonality analysis was not completed as a matter of practicality. The first line regimen we used for H. pylori eradication was a 7-day triple therapy with standard-dose proton-pump inhibitor (PPI) bid, clarithromycin 500 mg bid, and amoxicillin 1000 mg bid, and the second line regimen was a 7-day quadruple therapy with PPI standard dose bid, tripotassium dicitrato bismuthate 300 mg qid, metronidazole 500 mg tid, and tetracycline 500 mg qid. H. pylori eradication was evaluated in the follow-up endoscopy with histology and rapid urease testing.
The subsequent endoscopy was performed within 3 months of the initial screening endoscopy for both groups and at least 2 weeks after H. pylori eradication for the eradication first group. If the histological evaluation of the follow-up biopsy specimen resulted in a Wotherspoon score of 2 or less, the lesion was diagnosed as benign gastritis, and the patient was returned to our health checkup program and recommended to receive annual endoscopies. However, when gastric MALT lymphoma was confirmed by the follow-up biopsy during subsequent endoscopy, the stage was established in accordance with the Ann Arbor classification modified by Musshoff (19) using chest radiography, abdominal computed tomography, fluorine-18 fluorodeoxyglucose positron emission tomography, endoscopic ultrasound, and bilateral bone marrow biopsy. The treatment was conducted according to the international practice guidelines and consensus report (6,7), and the response to the treatment was reported based on the Groupe d’Etude des Lymphomes de l’Adult (GELA) grading system (20).
Statistical analysis
Data are expressed as the medians and ranges for continuous variables and as counts and percentages for categorical variables. To analyze differences between the groups, the Mann-Whitney U test was used for continuous variables, and the Pearson’s χ2 or Fisher’s exact test was used for categorical variables as appropriate. All statistical analyses were performed with SPSS (version 21.0; SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered significant.
Ethics statement
The study protocol was approved by the institutional review board of SNUH (IRB No. 1404-088-573), was exempted from the requirement to obtain informed consent, and conformed to the provisions of the Declaration of Helsinki, 2013.
RESULTS
Patients
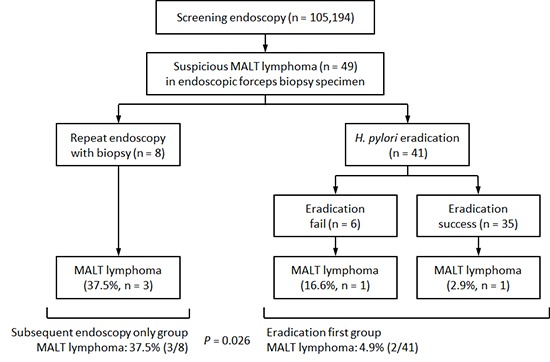
The study profile is described in Fig. 1. Between October 2003 and September 2013, a total of 121,802 men and women visited our healthcare center for routine checkups. Of these, 105,194 underwent 219,592 screening upper endoscopies, and 53,560 forceps biopsies were conducted during the procedures. Biopsy specimens were reported to be suspicious for MALT lymphoma when they received Wotherspoon scores of 3 or 4 in 72 subjects. After excluding 23 patients who failed to follow-up, the remaining 49 patients who received subsequent endoscopies without H. pylori eradication (subsequent endoscopy only group, n = 8) or who received H. pylori eradication first and then underwent subsequent endoscopy (eradication first group, n = 41) were included in the study.
Fig. 1.

Flow diagram showing the screening, enrollment, treatment, and follow-up of the patients with suspicious MALT lymphoma.
MALT, mucosa-associated lymphoid tissue; Hp, Helicobacter pylori.
The baseline characteristics are summarized in Table 1. The median patient age was 48.6 years (range, 29.0–71.9), and 55.1% (27 of 49) were male. The major endoscopic findings were erosions (30.6%, 15 of 49) and nodularity (26.5%, 13 of 49), and the endoscopic impression was MALT lymphoma only in 10.2% (5 of 49) of the patients. All patients were positive for H. pylori infection. There were no differences in the baseline characteristics according to the initial management strategy, except for age distribution, which was older in the subsequent endoscopy only group than in the eradication first group (P = 0.020, Table 1).
Table 1. Baseline characteristics of patients with suspicious MALT lymphoma.
| Characteristics | Overall (n = 49) |
Initial management strategy | ||
|---|---|---|---|---|
| Subsequent endoscopy only (n = 8) |
Eradication first (n = 41) |
P value* | ||
| Median age, yr (range) | 48.6 (29.0–71.9) | 55.0 (41.3–67.1) | 45.9 (29.0–71.9) | 0.020 |
| Gender, No. (%) | 0.440 | |||
| Male | 27 (55.1) | 3 (37.5) | 24 (58.5) | |
| Female | 22 (44.9) | 5 (62.5) | 17 (41.5) | |
| Endoscopic location, No. (%) | 0.247† | |||
| Upper | 9 (18.4) | 2 (25.0) | 7 (17.1) | |
| Middle | 16 (29.3) | 4 (50.0) | 12 (29.3) | |
| Lower | 22 (53.7) | 2 (25.0) | 22 (53.7) | |
| Endoscopic appearance, No. (%) | 0.333‡ | |||
| Polypoid | 3 (6.1) | 2 (25.0) | 1 (2.4) | |
| Thickened fold | 2 (4.1) | 1 (12.5) | 1 (2.4) | |
| Multinodular | 13 (26.5) | 1 (12.5) | 12 (29.3) | |
| Multifocal atrophic | 11 (22.4) | 2 (25.0) | 9 (22.0) | |
| Erosions | 15 (30.6) | 2 (25.0) | 13 (31.7) | |
| Ulcerative | 5 (10.2) | 0 (0.0) | 5 (12.2) | |
| Impression, No. (%) | 1.000§ | |||
| Lymphoma | 5 (10.2) | 1 (12.5) | 4 (9.8) | |
| Gastric cancer | 1 (2.0) | 0 (0.0) | 1 (2.4) | |
| Gastric polyp | 7 (14.3) | 1 (12.5) | 6 (14.6) | |
| Atrophy, metaplasia, gastritis | 11 (22.4) | 2 (25.0) | 9 (22.0) | |
| Erosion | 17 (34.7) | 3 (37.5) | 14 (34.1) | |
| Gastric ulcer | 6 (12.2) | 0 (0.0) | 6 (14.6) | |
| Others | 2 (4.1) | 1 (12.5) | 1 (2.4) | |
| Wotherspoon score, No. (%) | 1.000 | |||
| 3 | 4 (8.2) | 0 (0.0) | 4 (9.8) | |
| 4 | 45 (91.8) | 8 (100.0) | 37 (90.2) | |
| H. pylori positivity, No. (%) | 49 (100.0) | 8 (100.0) | 41 (100.0) | NA |
MALT, mucosa-associated lymphoid tissue; NA, not applicable.
*Comparison between the subsequent endoscopy only group and the eradication first group; †Comparison between upper/middle vs. lower third; ‡Comparison between superficial lesions (multinodular, multifocal atrophic, or erosions) vs. others (polypoid, thickened fold, or ulcerative); §Comparison between lymphoma vs. others.
Diagnosis of MALT lymphoma among the patients with suspicious lesions
Of those 49 patients, 5 (10.2%) were diagnosed with gastric MALT lymphoma in the subsequent endoscopy performed at a median of 43 days (range, 19–98) after the initial screening endoscopy (Fig. 1 and Table 2). Development of gastric MALT lymphoma was significantly lower in the eradication first group (2 of 41, 4.9%) than in the subsequent endoscopy only group (3 of 8, 37.5%, P = 0.026). H. pylori eradication was successful in 85.4% (35 of 41) of patients treated. Among the eradication first group, one MALT lymphoma patient was confirmed among the 6 patients who failed eradication, and the other MALT lymphoma patient was among the 35 patients with successful eradication. When H. pylori infection was successfully eradicated, gastric MALT lymphoma was diagnosed in only 2.9% of the patients (1 of 35). On the contrary, when H. pylori eradication was not attempted or failed, the diagnosis rate of gastric MALT lymphoma was significantly higher (28.6%, 4 of 14, P = 0.019).
Table 2. Clinical features of 7 cases with MALT lymphoma or recurrent suspicious MALT lymphoma.
| Case | Age, yr/Sex | Endoscopic location/appearance | Hp | WS | IHC | Initial management | Final dx | Time to final dx, day | Treatment | Response | Follow-up | F/u duration, mon |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 52/F | Middle third/erosions | + | 4 | CD3: nonspecific | Subsequent endoscopy only | MALToma, stage IE | 34 | Hp eradication | CR | MALToma recur → 2nd line Hp eradication → CR | 100 |
| CD20: positive | ||||||||||||
| Ki-67: focal positive | ||||||||||||
| Cytokeratin: presence of LEL | ||||||||||||
| 2 | 59/F | Upper third/ multifocal atrophic | + | 4 | CD3: focal positive | Subsequent endoscopy only | MALToma, stage IE | 43 | Hp eradication | PR | under follow-up | 9 |
| CD20: positive | ||||||||||||
| Ki-67: positive in 20% | ||||||||||||
| Cytokeratin: suspicious LEL | ||||||||||||
| 3 | 51/F | Upper third/Multinodular | + | 4 | CD3: focal positive | Subsequent endoscopy only | MALToma, stage IE | 19 | Hp eradication | PR | under follow-up | 13 |
| CD20: positive | ||||||||||||
| Ki-67: positive in 2% | ||||||||||||
| Cytokeratin: presence of LEL | ||||||||||||
| 4 | 56/F | Lower third/multifocal atrophic | + | 4 | CD3: nonspecific | Hp eradication → fail | MALToma, stage IE | 98 | 2nd line Hp eradication |
CR | No recur | 75 |
| CD20: positive | ||||||||||||
| Ki-67: focal positive | ||||||||||||
| Cytokeratin: suspicious LEL | ||||||||||||
| 5 | 53/F | Upper third/multifocal atrophic | + | 4 | CD3: focal positive | Hp eradication → success | MALToma, stage IE | 28 | Follow-up | CR | No recur | 99 |
| CD20: diffuse positive | ||||||||||||
| Ki-67: positive in 5% | ||||||||||||
| Cytokeratin: presence of LEL | ||||||||||||
| 6 | 48/M | Lower third/multinodular | + | 4 | CD3: nonspecific | Hp eradication → success | Gastritis | 75 | - | - | WS 4 lesion recur → repeat Hp eradication → regression | 35 |
| CD20: positive | ||||||||||||
| Ki-67: focal positive | ||||||||||||
| Cytokeratin: suspicious LEL | ||||||||||||
| 7 | 42/F | Upper third/erosions | + | 4 | CD3: focal positive | Hp eradication → success | Gastritis | 96 | - | - | WS 4 lesion recur → repeat Hp eradication → regression | 19 |
| CD20: positive | ||||||||||||
| Ki-67: positive in 5% | ||||||||||||
| Cytokeratin: presence of LEL |
MALT, mucosa-associated lymphoid tissue; Hp, Helicobacter pylori; WS, Wotherspoon score; IHC, immunohistochemistry; dx, diagnosis; f/u, follow-up; LEL, lymphoepithelial lesion; MALToma, extranodal marginal zone B-cell lymphoma mucosa-associated lymphoid tissue type; IE, I Extranodal; CR, complete remission; PR, partial remission.
Treatment of MALT lymphoma and long-term follow-up of all patients
All patients were followed for a median of 45.5 months (range, 1.8–108.6). Table 2 shows a summary of the clinical courses of 5 patients with MALT lymphoma and 2 patients with follicular gastritis but developed recurrent suspicious lesion during the follow-up period.
The initial stage was IE in all 5 patients with MALT lymphoma. The 4 patients (cases 1–4) who were diagnosed as MALT lymphoma while being H. pylori-positive were treated with H. pylori eradication; 2 patients achieved complete remission at 8 and 21 months of follow-up, respectively, and 2 showed partial remission at 7 and 13 months of follow-up, respectively, and are currently under follow-up. One of the 2 patients with complete remission developed a recurrence of MALT lymphoma after an additional 9 months of follow-up, was treated with second line eradication regimen, and then accomplished a second complete remission. However, 1 patient (case 5) who was diagnosed as MALT lymphoma despite successful eradication was followed without additional treatment and then achieved complete remission 11 months later.
As mentioned above, 2 of 34 patients (cases 6 and 7) who were initially confirmed as gastritis after H. pylori eradication developed Wotherspoon score 4 lesions with re-infection of H. pylori at 26 and 12 months of follow-up, respectively. H. pylori eradication was repeated in those patients, and the lesions regressed.
DISSCUSSION
In the present study, we evaluated H. pylori eradication as a management strategy for suspicious MALT lymphoma detected in screening endoscopy with forceps biopsy. We found that the eradication first strategy was associated with a significantly lower risk of MALT lymphoma development compared with the subsequent endoscopy only strategy. In particular, when the eradication was successful, the risk of developing MALT lymphoma was only 2.9%, and there was no recurrence of MALT lymphoma during a median 45 months of follow-up.
When suspicious MALT lymphoma was encountered in endoscopic forceps biopsy, the best management in principle would be making a definitive diagnosis between MALT lymphoma and follicular gastritis with additional tests, such as clonality analysis or a second endoscopy with gastric mapping (8,9,10,11), because lymphoma and gastritis have different treatment outcomes and prognoses. Although these additional evaluations would identify more MALT lymphomas from suspicious cases, the remaining cases still pose a risk of MALT lymphoma because the sensitivity of clonality analysis for MALT lymphoma was reported to be 92% (8) and that of second round endoscopy with biopsy was reported to be 83.3% (10). Thus, even after the diagnostic test has resulted in gastritis rather than lymphoma, many patients still want to receive H. pylori eradication therapy and follow-up endoscopy in clinical practice. Given this practical matter, H. pylori eradication followed by a subsequent endoscopy could be the most efficient strategy for the management of suspicious MALT lymphoma. In theory, it is expected that the long-term outcome after H. pylori eradication for suspicious MALT lymphoma would be excellent considering the favorable long-term outcome even in the patients with gastric MALT lymphoma (2). Our study proved this theoretical prediction to be clinically feasible, demonstrating that when H. pylori were eradicated, MALT lymphoma occurred in approximately 3% of patients during 4 years of endoscopic follow-up. Moreover, our study also showed that all 4 H. pylori-positive patients with MALT lymphoma showed complete or partial response to H. pylori eradication therapy. This observation suggests that our strategy of ‘H. pylori eradication first’ could have been applied safely to the 14 patients who received a second endoscopy without H. pylori eradication or when H. pylori eradication failed.
It is noteworthy that the lesions with Wotherspoon scores of 4 reappeared with H. pylori re-infection in the 2 of 34 patients who had been confirmed as gastritis after successful H. pylori eradication. Although this did not lead to the development of MALT lymphoma, it suggests that endoscopic follow-up is necessary after H. pylori eradication and regression of the suspicious lesion, especially in areas where the risk of H. pylori re-infection is high. Considering the necessity of endoscopic follow-up in all patients with suspicious MALT lymphoma, the H. pylori eradication followed by a subsequent endoscopy would not be the first-choice strategy in areas with low accessibility to upper endoscopy. However, in the context of active endoscopic screening for gastric cancer coupled with high prevalence of H. pylori infection in Far Eastern countries including Korea and Japan, the eradication first strategy would be a practical alternative option.
A major advantage of our study is that the study population was based on a large group of health checkup subjects who can be considered representative of the general population. However, there are also several limitations in this study. First, this was a retrospective study and had a potential for missing cases and selection bias. In particular, the treatment plan was not randomized, and some patients did not return for subsequent endoscopy. Second, this study considered a small number of patients and lacked molecular analyses such as clonality evaluation or MALT1 gene rearrangement analysis. However, our results may warrant further prospective studies incorporating molecular analyses, although this is not easy due to the rarity of the disease. Third, considering our study setting of endoscopic screening, the current results should be carefully extrapolated to the outpatient clinic-based settings where patients are usually symptomatic.
In conclusion, our data indicate that H. pylori eradication would be a practical management option for suspicious MALT lymphomas detected in forceps biopsy specimens from screening upper endoscopy. Further large prospective studies including molecular analysis are required.
ACKNOWLEDGMENT
The authors gratefully acknowledge the invaluable assistance of the following endoscopists at SNUH Healthcare System Gangnam Center in application of surveillance protocol as well as meticulous endoscopy procedures, Jeong Yoon Yim, Ji Hyun Song, Sun Young Yang, Mi Na Kim, Min-Sun Kwak, Donghee Kim, Goh Eun Chung, Jung Mook Kang, Seung Joo Kang, and Min Jung Park.
Footnotes
Funding: This work was supported by grant No. 34-2014-0230 from the SK Telecom Research Fund through Seoul National University Hospital.
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Conception and design: Yang HJ, Lim SH, Lee C. Acquisition of data: Yang HJ, Lee C, Yang JI, Chung SJ, Choi SH. Analysis and interpretation of data: Yang HJ, Lee C, Choi JM, Im JP, Kim SG, Kim JS. Drafting manuscript: Yang HJ, Lee C. Critical revision of manuscript: Lim SH, Choi JM, Yang JI, Chung SJ, Choi SH, Im JP, Kim SG, Kim JS. Final approval of manuscript: all authors.
References
- 1.Ferrucci PF, Zucca E. Primary gastric lymphoma pathogenesis and treatment: what has changed over the past 10 years? Br J Haematol. 2007;136:521–538. doi: 10.1111/j.1365-2141.2006.06444.x. [DOI] [PubMed] [Google Scholar]
- 2.Zullo A, Hassan C, Ridola L, Repici A, Manta R, Andriani A. Gastric MALT lymphoma: old and new insights. Ann Gastroenterol. 2014;27:27–33. [PMC free article] [PubMed] [Google Scholar]
- 3.Wotherspoon AC, Doglioni C, Diss TC, Pan L, Moschini A, de Boni M, Isaacson PG. Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type after eradication of Helicobacter pylori . Lancet. 1993;342:575–577. doi: 10.1016/0140-6736(93)91409-f. [DOI] [PubMed] [Google Scholar]
- 4.Achyut BR, Moorchung N, Srivastava AN, Gupta NK, Mittal B. Risk of lymphoid follicle development in patients with chronic antral gastritis: role of endoscopic features, histopathological parameters, CagA status and interleukin-1 gene polymorphisms. Inflamm Res. 2008;57:51–56. doi: 10.1007/s00011-007-7033-2. [DOI] [PubMed] [Google Scholar]
- 5.Doglioni C, Ponzoni M, Ferreri AJ, Savio A. Gruppo Italiano Patologi Apparato Digerente (GIPAD); Società Italiana di Anatomia Patologica e Citopatologia Diagnostica/International Academy of Pathology, Italian division (SIAPEC/IAP). Gastric lymphoma: the histology report. Dig Liver Dis. 2011;43(Suppl 4):S310–8. doi: 10.1016/S1590-8658(11)60587-2. [DOI] [PubMed] [Google Scholar]
- 6.Ruskoné-Fourmestraux A, Fischbach W, Aleman BM, Boot H, Du MQ, Megraud F, Montalban C, Raderer M, Savio A, Wotherspoon A, EGILS group EGILS consensus report. Gastric extranodal marginal zone B-cell lymphoma of MALT. Gut. 2011;60:747–758. doi: 10.1136/gut.2010.224949. [DOI] [PubMed] [Google Scholar]
- 7.Zucca E, Dreyling M, ESMO Guidelines Working Group Gastric marginal zone lymphoma of MALT type: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(Suppl 5):v175–6. doi: 10.1093/annonc/mdq182. [DOI] [PubMed] [Google Scholar]
- 8.Hummel M, Oeschger S, Barth TF, Loddenkemper C, Cogliatti SB, Marx A, Wacker HH, Feller AC, Bernd HW, Hansmann ML, et al. Wotherspoon criteria combined with B cell clonality analysis by advanced polymerase chain reaction technology discriminates covert gastric marginal zone lymphoma from chronic gastritis. Gut. 2006;55:782–787. doi: 10.1136/gut.2005.080523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wündisch T, Neubauer A, Stolte M, Ritter M, Thiede C. B-cell monoclonality is associated with lymphoid follicles in gastritis. Am J Surg Pathol. 2003;27:882–887. doi: 10.1097/00000478-200307000-00002. [DOI] [PubMed] [Google Scholar]
- 10.Xu W, Zhou C, Zhang G, Wang H, Wang L, Guo J. Repeating gastric biopsy for accuracy of gastric lymphoma diagnosis. Gastroenterol Nurs. 2010;33:313–317. doi: 10.1097/SGA.0b013e3181ea9035. [DOI] [PubMed] [Google Scholar]
- 11.Taal BG, Boot H, van Heerde P, de Jong D, Hart AA, Burgers JM. Primary non-Hodgkin lymphoma of the stomach: endoscopic pattern and prognosis in low versus high grade malignancy in relation to the MALT concept. Gut. 1996;39:556–561. doi: 10.1136/gut.39.4.556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Stolte M. Helicobacter pylori gastritis and gastric MALT-lymphoma. Lancet. 1992;339:745–746. doi: 10.1016/0140-6736(92)90645-j. [DOI] [PubMed] [Google Scholar]
- 13.Rudolph B, Bayerdörffer E, Ritter M, Müller S, Thiede C, Neubauer B, Lehn N, Seifert E, Otto P, Hatz R, et al. Is the polymerase chain reaction or cure of Helicobacter pylori infection of help in the differential diagnosis of early gastric mucosa-associated lymphatic tissue lymphoma? J Clin Oncol. 1997;15:1104–1109. doi: 10.1200/JCO.1997.15.3.1104. [DOI] [PubMed] [Google Scholar]
- 14.Chung SJ, Park MJ, Kang SJ, Kang HY, Chung GE, Kim SG, Jung HC. Effect of annual endoscopic screening on clinicopathologic characteristics and treatment modality of gastric cancer in a high-incidence region of Korea. Int J Cancer. 2012;131:2376–2384. doi: 10.1002/ijc.27501. [DOI] [PubMed] [Google Scholar]
- 15.Choi KS, Jun JK, Lee HY, Park S, Jung KW, Han MA, Choi IJ, Park EC. Performance of gastric cancer screening by endoscopy testing through the National Cancer Screening Program of Korea. Cancer Sci. 2011;102:1559–1564. doi: 10.1111/j.1349-7006.2011.01982.x. [DOI] [PubMed] [Google Scholar]
- 16.Nakamura T, Seto M, Tajika M, Kawai H, Yokoi T, Yatabe Y, Nakamura S. Clinical features and prognosis of gastric MALT lymphoma with special reference to responsiveness to H. pylori eradication and API2-MALT1 status. Am J Gastroenterol. 2008;103:62–70. doi: 10.1111/j.1572-0241.2007.01521.x. [DOI] [PubMed] [Google Scholar]
- 17.Kolve M, Fischbach W, Greiner A, Wilms K, German Gastrointestinal Lymphoma Study Group Differences in endoscopic and clinicopathological features of primary and secondary gastric non-Hodgkin’s lymphoma. Gastrointest Endosc. 1999;49:307–315. doi: 10.1016/s0016-5107(99)70006-4. [DOI] [PubMed] [Google Scholar]
- 18.Lim SH, Kwon JW, Kim N, Kim GH, Kang JM, Park MJ, Yim JY, Kim HU, Baik GH, Seo GS, et al. Prevalence and risk factors of Helicobacter pylori infection in Korea: nationwide multicenter study over 13 years. BMC Gastroenterol. 2013;13:104. doi: 10.1186/1471-230X-13-104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Musshoff K. Clinical staging classification of non-Hodgkin’s lymphomas (author’s transl) Strahlentherapie. 1977;153:218–221. [PubMed] [Google Scholar]
- 20.Shiozawa E, Norose T, Kaneko K, Yamochi-Onizuka T, Takimoto M, Imawari M, Ota H. Clinicopathological comparison of the World Health Organization/Wotherspoon score to the Groupe d’Etude des Lymphomes de l’Adult grade for the post-treatment evaluation of gastric mucosa-associated lymphoid tissue lymphoma. J Gastroenterol Hepatol. 2009;24:307–315. doi: 10.1111/j.1440-1746.2008.05639.x. [DOI] [PubMed] [Google Scholar]