

Abstract
Mushroom exposures are increasing worldwide. The incidence and fatality of mushroom poisoning are reported to be increasing. Several new syndromes in mushroom poisoning have been described. Rhabdomyolytic mushroom poisoning is one of new syndromes. Russula subnigricans mushroom can cause delayed-onset rhabdomyolysis with acute kidney injury in the severely poisoned patient. There are few reports on the toxicity of R. subnigricans. This report represents the first record of R. subnigricans poisoning with rhabdomyolysis in Korea, describing a 51-year-old man who suffered from rhabdomyolysis, acute kidney injury, severe hypocalcemia, respiratory failure, ventricular tachycardia, cardiogenic shock, and death. Mushroom poisoning should be considered in the evaluation of rhabdomyolysis of unknown cause. Furthermore, R. subnigricans should be considered in the mushroom poisoning with rhabdomyolysis.
Keywords: Mushroom Poisoning, Rhabdomyolysis, Acute Kidney Injury, Respiratory Failure, Cardiogenic Shock
Graphical Abstract
INTRODUCTION
More leisure time for hobbies, hiking, and trekking has led to more mushroom exposures. Increased demands for uncultivated food or gastronomic delights have contributed to more mushroom poisoning. Amateur mushroom hunters occasionally confuse toxic mushrooms with edible ones. Although severe mushroom poisonings and fatalities remain infrequent, the proportions of fatal mushroom poisonings among confirmed mushroom ingestions seems to be increasing (1). In addition to increasing poisoning of known toxic mushroom, new mushroom syndromes have been described (2,3). Russula subnigricans mushroom poisoning can be classified as delayed-onset rhabdomyolytic syndrome. The severe patient with R. subnigricans mushroom poisoning was reported to present with rhabdomyolysis, severe electrolyte disturbance (hyperkalemia, hypocalcemia), acute renal failure, respiratory failure, pulmonary edema, ventricular tachycardia, and circulatory shock (4,5). In this case report, we present a patient poisoned by R. subnigricans mushroom complicated with rhabdomyolysis, acute kidney injury (AKI), severe hypocalcemia, respiratory failure, ventricular tachycardia, and cardiogenic shock, leading to death.
CASE DESCRIPTION
A 51-year old man had a breakfast cooked with wild mushrooms that he had gathered one day earlier during summer vacation in August, 2010 at the Jujak mountain located on the province of Jeollanam-do, the southern area of Korea. He was a bus driver. He had no particular past medical or social history other than the occasional ingestion of wild mushrooms during recreational hiking. He was healthy before this admission. He did not have a history of trauma, infection, other known underlying cause, or medication use that could explain the occurrence of rhabdomyolysis. He shared the meal with his wife and son who did not eat any more mushrooms due to nausea after ingesting a single piece of mushroom. However, he ate the mushrooms without immediate symptom. Six hours later, he began to complain of vomiting, diarrhea, and myalgia. He visited a local hospital where his general condition worsened and systolic BP fell to 60 mmHg requiring dopamine treatment and endotracheal intubation. Twenty-eight hours after ingestion of the mushrooms, he was transferred to the intensive care unit of our hospital. At the time of admission, he was alert, but acute ill-looking. He complained of generalized myalgia, chest discomfort, palpitations, and dyspnea. Blood pressure was 80/56 mmHg, heart rate 121/min, respiratory rate 25/min, and body temperature 36.3oC. Oliguria was noted with no response to intravenous fluid and furosemide. Systolic murmurs were present on auscultation. Laboratory tests showed the following: hemoglobin 15.9 g/dL, hematocrit 45.9%, leukocyte count 20,740/μL with neutrophil 89.6%, platelet 253,000/μL, C-reactive protein (CRP) 8.36 mg/dL, blood urea nitrogen (BUN) 38.5 mg/dL, serum creatinine 2.84 mg/dL, serum osmolarity 314 mOsm/kg, sodium 140 mEq/L, potassium 4.7 mEq/L, chloride 100 mEq/L, ionized calcium 0.75 mmol/L, glucose 187 mg/dL, cholesterol 221 mg/dL, albumin 4.0 g/dL, aspartate aminotransferase (AST) 1,214 U/L, alanine aminotransferase (ALT) 343 U/L, total bilirubin 0.51 mg/dL, alkaline phosphatase 92 IU/L, creatine kinase (CK) 69,121 U/L, CK-MB > 500 ng/mL, lactate dehydrogenase (LDH) 2,196 U/L, troponin I 1.86 ng/mL, N-terminal pro brain natriuretic peptide (NT-pro BNP) 7,414 pg/mL, amylase 1,930 U/L, lipase 18 U/L, prothrombin time (PT) 10.2 seconds. (INR 0.86), activated partial thromboplastin time (aPTT) 28.2 seconds, urine osmolarity 341 mOsm/kg, sodium 22 mEq/L, potassium 59.2 mEq/L, chloride 14 mEq/L, creatinine 123.8 mg/dL, myoglobin 51.7 ng/mL, and fractional excretion of sodium 0.36%. Urine analysis showed pH 5.0, specific gravity 1.020, protein 2+, ketone 2+, blood 4+, RBC 5-9/high-power field, and WBC 0-1/high-power field. Blood and urine cultures were all negative for microorganism. Arterial blood gas analysis was pH 7.04, PaCO2 69 mmHg, PaO2 172 mmHg, and HCO3 - 18.7 mmol/L. Chest radiographs revealed mild cardiomegaly without lung lesion. Electrocardiogram (ECG) showed sinus tachycardia with QT prolongation. The enlarged left ventricle (LV), severe LV systolic dysfunction (ejection fraction 30%), and akinesia of LV mid to apex wall suggesting stress induced cardiomyopathy were noted on echocardiography. He received ventilator support, hemodynamic monitoring, continuous venovenous hemodiafiltration, and conservative care including intravenous fluid and electrolyte repletion. Seventy hours after ingestion of the mushrooms, BUN 41.9 mg/dL, serum creatinine 3.46 mg/dL, AST 3,271 U/L, ALT 1,254 U/L, total bilirubin 1.55 mg/dL, CK 121,397 U/L, CK-MB >500 ng/mL, LDH 6,102 U/L, troponin I 11.77 ng/mL, amylase 2,779 U/L, lipase 601 U/L, PT 42.1 seconds. (INR 3.34), and aPTT > 150 seconds. Blood pressure continued to decrease despite intravenous fluid and inotropics. Ventricular tachycardia developed, and he died due to cardiogenic shock 72 hours after ingestion of the mushrooms.
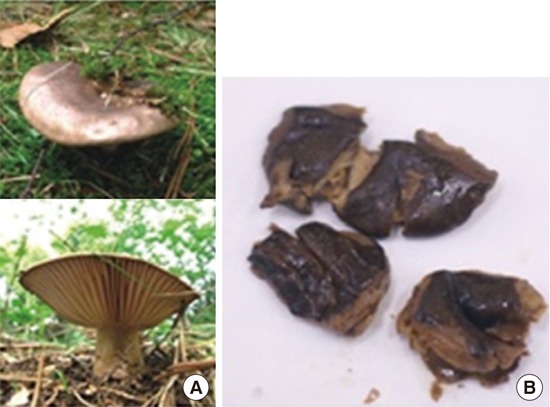
The leftover samples of the mushrooms that he had ingested were sent to Agricultural Microbiology Division, National Academy of Agricultural Science, Rural Development Administration, Suwon, Korea. Those were identified as R. subnigricans by their gross morphology (Fig. 1). Further examination by microscopy also confirmed the presence of spores from R. subnigricans.
Fig. 1.
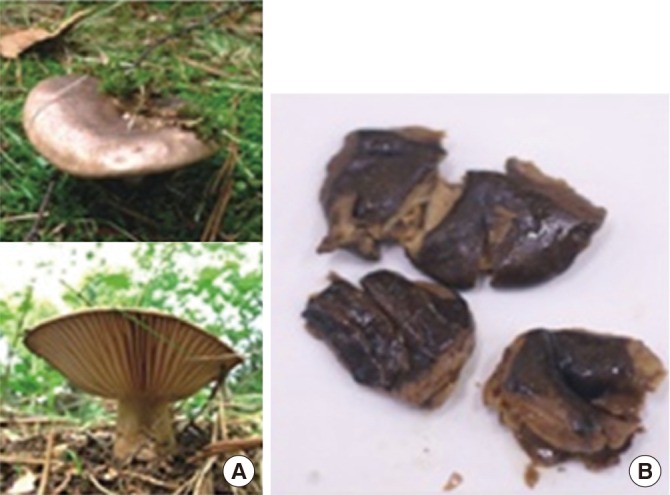
Gross morphology of Russula subnigricans mushroom (A) and the leftover samples (B) of our case.
DISCUSSION
The worldwide incidence of mushroom poisoning appears to be increasing due to increased human demands for uncultivated food or hallucinogenic mushrooms. The proportion of severe and fatal mushroom poisonings among confirmed mushroom ingestions has demonstrated statistically significant increases. Deaths, although rare, occurred most commonly from the ingestion of Amanita species, primarily Amanita phalloides, in adult amateur mushroom hunters (1,6). In addition to increasing poisons following ingestions of known species, formerly edible or new mushroom species are causing newly recognized syndromes from mushroom poisonings. Several new syndromes in mushroom poisoning have been described since the early 1990s (1,2,3): accelerated nephrotoxicity (non-orellanine-induced renal failure), erythromelalgia, rhabdomyolysis, and delayed neurotoxicity (convulsive or non-convulsive encephalopathy).
Rhabdomyolysis is a new type of mushroom poisoning caused by ingestion of Tricholoma equestre (1,3,4,7). Some of these cases with rhabdomyolysis are associated not only with renal dysfunction and electrolyte disturbance (hyperkalemia, hypocalcemia), but also with respiratory and cardiac complications (arrhythmia, cardiovascular collapse) leading to death (4). Some other mushrooms are suspected to have a similar effect (8,9,10). An outbreak of Russula subnigricans poisoning with rhabdomyolysis occurred in Taiwan (5). The most severely ill patient presented with rhabdomyolysis, severe electrolyte disturbance (hyperkalemia, hypocalcemia), respiratory failure, acute renal failure, pulmonary edema, ventricular tachycardia, and circulatory shock. Japan has also experienced several cases of fatal poisoning with rhabdomyolysis caused by ingestion of this mushroom (3,11). Russula species is found worldwide. R. eccentrica, R. nigricans and R. subnigricans have been recorded in Korea (12). These are commonly found during the summer and fall in Korea. Poisonous R. subnigricans can be mistaken with non-poisonous, edible R. eccentrica and R. nigricans. R. subnigricans can be found associated with broad-leaved evergreen tree habitat which is present and restricted to the southern area of Korean peninsula. This report of our case represents the first record of R. subnigricans poisoning with rhabdomyolysis in Korea.
Rhabdomyolysis, the dissolution of skeletal muscle, is a rare but potentially fatal condition. The common causes of rhabdomyolysis are trauma, exertion, muscle hypoxia, infections, body temperature changes, metabolic and electrolyte disorders, drug and toxins, and genetic defects. The incidence of rhabdomyolysis in acute poisonings was the highest in poisonings with opiates, pesticides, neuroleptics, anticonvulsants, and ethyl alcohol (13,14). In our case, severe rhabdomyolysis with AKI, severe hypocalcemia, respiratory failure, ventricular tachycardia, and cardiogenic shock were noted throughout the clinical course. There was no history of trauma, strenuous exercise, seizures, and loss of consciousness. He had no particular past medical or drug history. There was no evidence of infections, hyperthermia or hypothermia, hypokalemia or hypophosphatemia. The possible cause of rhabdomyolysis after ingestion of the mushroom may be the mushroom toxin, such as cycloprop-2-ene carboxylic acid, isolated from R. subnigricans. This compound may be responsible for fatal rhabdomyolysis as a toxic trigger for some biochemical reactions (10,11). The mechanism involved in the pathogenesis of rhabdomyolysis is depletion of ATP within the myocyte, leading to an unregulated increase in intracellular calcium, resulting in disintegration of the myocyte. Hypocalcemia noted in our case is a common complication of rhabdomyolysis. It usually results from calcium entering the damaged myocyte and from the precipitation of calcium phosphate in necrotic muscle. AKI is a potential complication of rhabdomyolysis. Intrarenal vasoconstriction, direct and ischemic tubular injury, and tubular obstruction all may play a role in myoglobin-induced AKI (13). R. subnigricans poisoning might influence cardiac function. Cardiogenic shock due to severe LV systolic dysfunction might be caused by the mushroom toxin (4,5,15,16).
General management of mushroom poisoning is fluid resuscitation, early gastric decontamination by both gastric lavage and multiple dose activated charcoal, and baseline laboratory assessment. Since mushroom-poisoned patients often experience vomiting and diarrhea, emetics and cathartics are rarely indicated. Treatment should be directed by the patient's clinical manifestation (1,17). The mushroom poisoning with rhabdomyolysis is usually associated with volume depletion that is due to the sequestration of water in damaged muscles. Therefore, the early, aggressive repletion of fluids is the main step of management. Hyperkalemia must be corrected promptly. However, early hypocalcemia should not be treated unless it is symptomatic or unless severe hyperkalemia is present, since the calcium load could increase the precipitation of calcium phosphate in necrotic muscle (13). Continuous venovenous hemofiltration or hemodiafiltration has shown some efficacy in removing myoglobin (18). However, the evidence is from case reports, and the effect on outcomes is unknown. Acute neuromuscular syndrome often requires seizure prophylaxis and ventilator support. If renal or hepatic function is worsening, patients should be transferred to the hospital equipped for hemodialysis and kidney or liver transplantation (1). Intra-aortic balloon counterpulsation can be considered as a final treatment option in the mushroom poisoning with cardiogenic shock (15). Primary prevention of mushroom poisoning is to avoid consuming uncultivated mushrooms. Correct categorization and better understanding are essential for the safe and healthy consumption of mushrooms (19). Since mushroom toxicity may be dose-related, overconsuming mushrooms should be avoided (1).
Mushroom poisoning should be considered in the evaluation of rhabdomyolysis of unknown cause. Furthermore, R. subnigricans should be considered in the mushroom poisoning with rhabdomyolysis. To confirm the exact diagnosis, leftover raw or cooked mushrooms should be collected and sent to a mycologist for gross and spore identification.
ACKNOWLEDGMENT
We appreciate Dr. Soon-Ja Seok, working at National Academy of Agricultural Science, for her technical support and identification of the mushroom.
Footnotes
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Conception of the study: Cho JT. Acquisition of data: Han JH. Data review: Cho JT, Han JH. Manuscript preparation: Cho JT. Manuscript approval: all authors.
References
- 1.Diaz JH. Evolving global epidemiology, syndromic classification, general management, and prevention of unknown mushroom poisonings. Crit Care Med. 2005;33:419–426. doi: 10.1097/01.ccm.0000153530.32162.b7. [DOI] [PubMed] [Google Scholar]
- 2.Diaz JH. Syndromic diagnosis and management of confirmed mushroom poisonings. Crit Care Med. 2005;33:427–436. doi: 10.1097/01.ccm.0000153531.69448.49. [DOI] [PubMed] [Google Scholar]
- 3.Saviuc P, Danel V. New syndromes in mushroom poisoning. Toxicol Rev. 2006;25:199–209. doi: 10.2165/00139709-200625030-00004. [DOI] [PubMed] [Google Scholar]
- 4.Bedry R, Baudrimont I, Deffieux G, Creppy EE, Pomies JP, Ragnaud JM, Dupon M, Neau D, Gabinski C, De Witte S, et al. Wild-mushroom intoxication as a cause of rhabdomyolysis. N Engl J Med. 2001;345:798–802. doi: 10.1056/NEJMoa010581. [DOI] [PubMed] [Google Scholar]
- 5.Gan SQ, McBride OW, Idler WW, Markova N, Steinert PM. Organization, structure, and polymorphisms of the human profilaggrin gene. Biochemistry. 1990;29:9432–9440. doi: 10.1021/bi00492a018. [DOI] [PubMed] [Google Scholar]
- 6.Schenk-Jaeger KM, Rauber-Lüthy C, Bodmer M, Kupferschmidt H, Kullak-Ublick GA, Ceschi A. Mushroom poisoning: a study on circumstances of exposure and patterns of toxicity. Eur J Intern Med. 2012;23:e85–91. doi: 10.1016/j.ejim.2012.03.014. [DOI] [PubMed] [Google Scholar]
- 7.Chodorowski Z, Waldman W, Sein Anand J. Acute poisoning with Tricholoma equestre. Przegl Lek. 2002;59:386–387. [PubMed] [Google Scholar]
- 8.Bickel M, Ditting T, Watz H, Roesler A, Weidauer S, Jacobi V, Gueller S, Betz C, Fichtlscherer S, Stein J. Severe rhabdomyolysis, acute renal failure and posterior encephalopathy after 'magic mushroom' abuse. Eur J Emerg Med. 2005;12:306–308. doi: 10.1097/00063110-200512000-00011. [DOI] [PubMed] [Google Scholar]
- 9.Nieminen P, Kirsi M, Mustonen AM. Suspected myotoxicity of edible wild mushrooms. Exp Biol Med (Maywood) 2006;231:221–228. doi: 10.1177/153537020623100213. [DOI] [PubMed] [Google Scholar]
- 10.Yin X, Feng T, Shang JH, Zhao YL, Wang F, Li ZH, Dong ZJ, Luo XD, Liu JK. Chemical and toxicological investigations of a previously unknown poisonous European mushroom Tricholoma terreum. Chemistry. 2014;20:7001–7009. doi: 10.1002/chem.201400226. [DOI] [PubMed] [Google Scholar]
- 11.Matsuura M, Saikawa Y, Inui K, Nakae K, Igarashi M, Hashimoto K, Nakata M. Identification of the toxic trigger in mushroom poisoning. Nat Chem Biol. 2009;5:465–467. doi: 10.1038/nchembio.179. [DOI] [PubMed] [Google Scholar]
- 12.Park MS, Lee H, Oh SY, Jung PE, Seok SJ, Fong JJ, Lim YW. Species delimitation of three species within the Russula subgenus Compacta in Korea: R. eccentrica, R. nigricans, and R. subnigricans . J Microbiol. 2014;52:631–638. doi: 10.1007/s12275-014-4168-z. [DOI] [PubMed] [Google Scholar]
- 13.Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361:62–72. doi: 10.1056/NEJMra0801327. [DOI] [PubMed] [Google Scholar]
- 14.Janković SR, Stosić JJ, Vucinić S, Vukcević NP, Ercegović GV. Causes of rhabdomyolysis in acute poisonings. Vojnosanit Pregl. 2013;70:1039–1045. doi: 10.2298/vsp1311039j. [DOI] [PubMed] [Google Scholar]
- 15.Aygul N, Duzenli MA, Ozdemir K, Altunkeser BB. A case report of an unusual complication of Amanita phalloides poisoning: development of cardiogenic shock and its successful treatment with intra-aortic balloon counterpulsation. Toxicon. 2010;55:630–632. doi: 10.1016/j.toxicon.2009.10.022. [DOI] [PubMed] [Google Scholar]
- 16.Altintepe L, Yazici R, Yazici M, Solak Y, Topal M, Isik A, Guney I. Temporary left ventricular dysfunction in mushroom poisoning: report of three cases. Ren Fail. 2014;36:1337–1339. doi: 10.3109/0886022X.2014.930649. [DOI] [PubMed] [Google Scholar]
- 17.Eren SH, Demirel Y, Ugurlu S, Korkmaz I, Aktas C, Güven FM. Mushroom poisoning: retrospective analysis of 294 cases. Clinics (Sao Paulo) 2010;65:491–496. doi: 10.1590/S1807-59322010000500006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ronco C. Extracorporeal therapies in acute rhabdomyolysis and myoglobin clearance. Crit Care. 2005;9:141–142. doi: 10.1186/cc3055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jo WS, Hossain MA, Park SC. Toxicological profiles of poisonous, edible, and medicinal mushrooms. Mycobiology. 2014;42:215–220. doi: 10.5941/MYCO.2014.42.3.215. [DOI] [PMC free article] [PubMed] [Google Scholar]