

Abstract
In the present study, we aimed to determine the differences in body image along with anxiety and depression levels, and also to evaluate their impact on disability parameters in patients with hepatitis B.
Our study comprised 77 patients with hepatitis B (n = 41, chronic active patients; n = 36, patients with inactive hepatitis B) and 53 healthy individuals (control group). Enrolled patients responded to several questionnaires, including a sociodemographic form, Sheehan Disability Scale (SDS), Hospital Anxiety and Depression Scale (HADS), and Somatosensory Amplification Scale.
Patients with chronic active hepatitis B (CAHB) had higher levels of somatosensory perception than patients with inactive hepatitis B (IHB) and control group (P < 0.001, P = 0.001, respectively). Patients with CAHB had high scores on all the 3 domains of SDS (work/school, P < 0.001; social life, P < 0.001; and family life, P < 0.001). Also, patients with CAHB had a significantly higher HADS total score, HADS anxiety score, and HADS depression score than control group (P < 0.001, P < 0.001, P < 0.001, respectively). No significant difference was noted between patients with CAHB and patients with IHB with regard to HADS depression score; however, HADS anxiety and HADS total scores were significantly higher in the CAHB group (NS, P = 0.027, P = 0.035, respectively). Moreover, the IHB group exhibited higher scores for the work/school and social life domains of SDS than those of the control group (P = 0.008, P = 0.047).
Although patients with CAHB may present with somatosensory amplification, anxiety, and depression, patients with IHB do not exhibit such symptoms. However, functionality is affected in both carrier and active patient groups. We believe that routine health checks of patients with hepatitis B should include psychiatric evaluation, psychiatric examination, and follow-up.
INTRODUCTION
Today, hepatitis B is recognized globally as a major cause of chronic hepatitis, cirrhosis, and hepatocellular carcinoma (HCC).1 Inadequate and incorrect data, concerning the transmission modes of the hepatitis B virus and its chronic course, may lead to isolation of the carriers in their social and work lives. The presence of a relationship between chronic physical conditions and psychiatric disorders (depression and anxiety being the foremost of the psychiatric conditions) has been reported in several studies.2,3 Psychosocial problems, such as exposure to significant levels of stress, depression, and isolation, associated with deterioration in social and occupational functionality along with negative changes in life style, may occur in patients with hepatitis. These patients may suffer from amplified bodily sensation, which they may perceive as disturbing, and negative experiences that lead to interpretation of normal bodily sensations as unfavorable and unhealthy.
Psychiatric disorders that may arise during and/or after drug therapy for chronic hepatitis have been investigated, and psychiatric symptoms have been found to be common under such conditions. Studies indicate that psychiatric profiles associated with chronic hepatitis and the social and economic outcomes of these profiles should be investigated in all patients.4,5
In the present study, we aimed to determine the differences between patients with chronic active hepatitis B (CAHB) and carriers of inactive hepatitis B (IHB) with regard to perception of bodily sensations, anxiety, and depression, in addition to studying the impact of these differences on functionality.
To explain somatization in patients with chronic diseases, a somatosensory amplification pattern is employed. Barsky et al were the first to use the term somatosensory amplification, which has been defined as somatization of normal bodily sensations as relatively intense and disturbing. The isolation of the carriers may stem from the infectious nature of the hepatitis B virus, inadequate knowledge on transmission modes, and baseless concerns about the transmissibility of the virus.6 In our opinion, somatic amplification, coupled with depression, anxiety, and disability, may further aggravate the burden of hepatitis, leading to elevated risk of hepatitis-related diseases. Our search of the literature revealed no studies showing an association between perception of bodily sensations and disability in patients with CAHB and IHB in a homogeneous group that consisted of patients with hepatitis B. Previous studies did not observe the 3 measures—Sheehan Disability Scale (SDS), Hospital Anxiety and Depression Scale (HADS), and Somatosensory Amplification Scale (SSAS)7,8—in hepatitis B patients. To the best of our knowledge, the present study is the first article over the relationship between somatic amplification and hepatitis-related disability using these 3 measures.
METHODS
Study Population
The present study was carried out as a joint research project between the departments of Family Medicine and Infectious Diseases at Dicle University Faculty of Medicine Hospital, from May 15, 2015 to October 15, 2015. CAHB and IHB were defined according to the European Association for the Study of the Liver Guidelines (EASL).9
Inactive hepatitis B was defined as the presence of hepatitis B virus with no necrosis or inflammation in the liver, in addition to finished or limited viral replication rates HBV surface antigen (HbsAg) positivity for longer than 6 months, Hepatitis Be antigen (HBeAg) [−]/anti-HBeAg [+], Hepatitis B Virus-Deoxyribose Nükleik acid (HBV-DNA) <2000 IU/mL, permanently normal alanine transaminase [ALT] level).
Chronic active hepatitis B was defined as the presence of HBeAg(−) and HBV-DNA >2000 IU/mL, permanent or intermittent increases in ALT level.
A total of 36 IHB and 41 patients with CAHB were included in the study. Inclusion criteria for patients with hepatitis were as follows: no signs of cirrhosis or cancer, age range 18 to 70 years, and no known psychiatric disease or history of treatment with psychiatric drugs.
In our study, the patient group with CAHB was classified as HBeAg-negative CHB according to EASL 2012 Clinical Practice Guidelines. The control group consisted of 53 healthy individuals with no complaints of symptoms.
Once diagnosed, our patients were enrolled into the study. Testing of psychiatric scales was not performed within certain periods. They were not receiving any antiretroviral drugs and treatment related to their clinical conditions during enrolment. No additional organ damage was developed during their follow-up. Our control group consisted of healthy volunteers without any disorder manifesting who acknowledged psychiatric self-rating scales.
Before the patient and control groups selection, 22 patients were excluded because of known psychiatric disease and a history of recent psychiatric drug treatment (both psychiatric disease and treatment with psychiatric drugs were revealed through psychiatric consultation) or refusal to consent to participation in the study. No human immunodeficiency virus (HIV) or hepatitis C virus infection was detected.
Before responding to questionnaires, subjects received information on the aim, design, and possible scientific contributions of the present study, and were informed of their rights. We used the personal interview technique to collect study data via questionnaires, which included the SSAS, SDS, and HADS. A descriptive characteristics form was included with the questionnaires to provide information on participants’ age, sex, marital status, and educational background, and also on characteristics related to hepatitis. The study was approved by the “Noninterventional Clinical Researches Ethics Committee” on May 14, 2015 (approval number #295).
Data Collection and Measurements
Interview Form
The interview form was prepared by the authors to collect demographic variables including age, sex, educational level, and marital status of the participants and to determine patients’ attitudes toward their diagnosis.
SSAS
The SSAS assesses the tendency to perceive normal bodily sensations as being relatively intense and disturbing. This self-report scale, designed by Barsky et al,10 consists of 10 items as follows:
I can’t stand smoke, smog, or pollutants in the air
I am often aware of various things happening within my body
When I bruise myself, it stays noticeable for a long time
I sometimes can feel the blood flowing in my body
Sudden loud noises really bother me
I can sometimes hear my pulse or my heartbeat throbbing in my ear
I hate to be too hot or too cold
I am quick to sense the hunger contractions in my stomach
Even something minor, like an insect bite or a splinter really bothers me
I can’t stand pain
Each item was assessed on a 5-point scale ranging from 1 (not at all) to 5 (all the time).11 The statements describe physical discomfort and are not suggestive of disease. Total amplification score is calculated by totalling each score. The reliability and validity of the Turkish version was shown by Gulec al.12
SDS
The SDS was developed to assess functional impairment in 3 domains: work/school, social life/leisure activities, and family life/home responsibilities. The patient rates the impairment levels of the above-mentioned domains on a 10-point scale.13
HADS
The HADS was developed by Zigmond and Snaith.14 The validity and reliability of the Turkish version was shown by Aydemir et al.15 The HADS is a 14-item, self-report scale, which consists of depression and anxiety subscales, each with 7 items. In Turkish version of HADS forms, cut-off points for the Anxiety Subscale (HAD-A) and Depression Subscale (HAD-D) were determined as 10/11 and 8, respectively.16 The minimal and maximal scores that any patient can obtain from both of the subscales are 0 and 21, respectively.
Statistical Analysis
SPSS software V.18.0 (SPSS for Windows software; SPSS, Inc, Chicago, IL, USA) was used for statistical analyses. Mean values of the groups were compared with a 1-way analysis of variance (ANOVA) or Kruskal–Wallis tests. The paired comparisons were performed using a post-hoc test or a Mann–Whitney U test.
RESULTS
Our study included 77 patients—36 IHB (27.7%) and 41 CAHB (31.5%)—and 53 (40.8%) healthy controls. Seventy-three of the participants (56.2%) were female and 57 (43.8%) were male. The mean age was 36 ± 9.02 in the patient group and 36 ± 6.4 in the control group. In the IHB group, the mean age was 36.5 ± 10.2, whereas 17 (47.2%) were male and 19 (52.8%) were female. In the CAHB group, the mean age was 35.56 ± 7.8 years, whereas 19 (46.3%) were male and 22 (53.7%) were female. The other sociodemographic characteristics and biochemical data are shown in Table 1.
TABLE 1.
Sociodemographic Features and Laboratory Parameters of the Groups
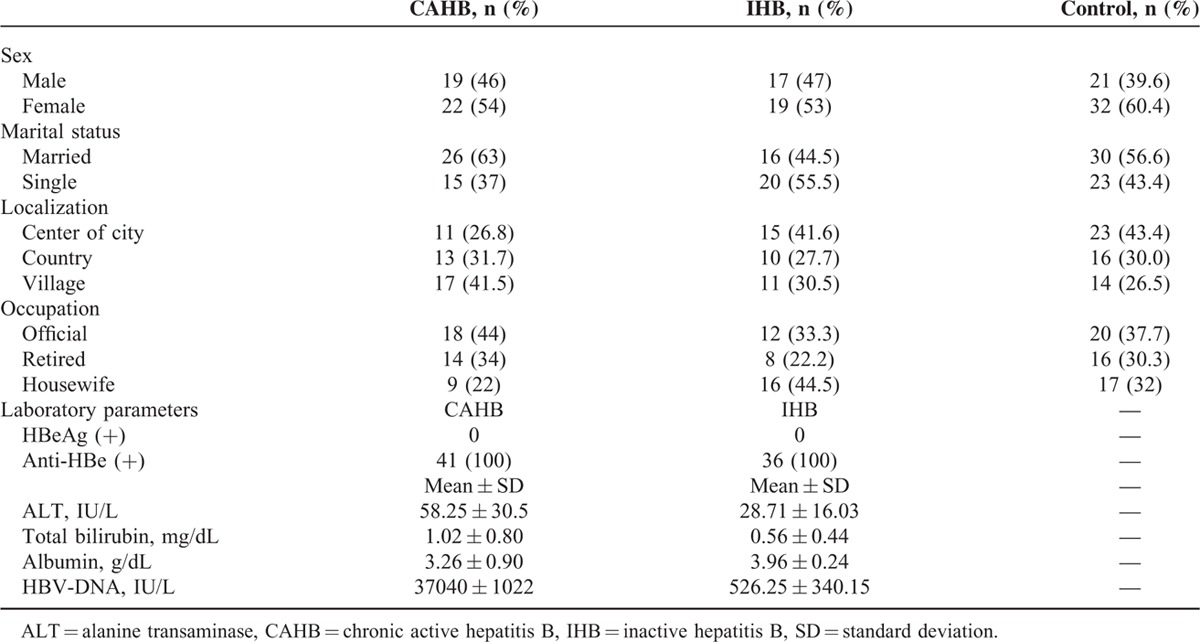
Depression scoring for HAD yielded as 47.2%, 60%, and 25% in IHB, CAHB, and controls, respectively. When assessed in terms of HAD anxiety scores, they were above their cut-off values, with 33.5%, 48.7%, and 20.7% in IHB, CAHB, and controls, respectively.
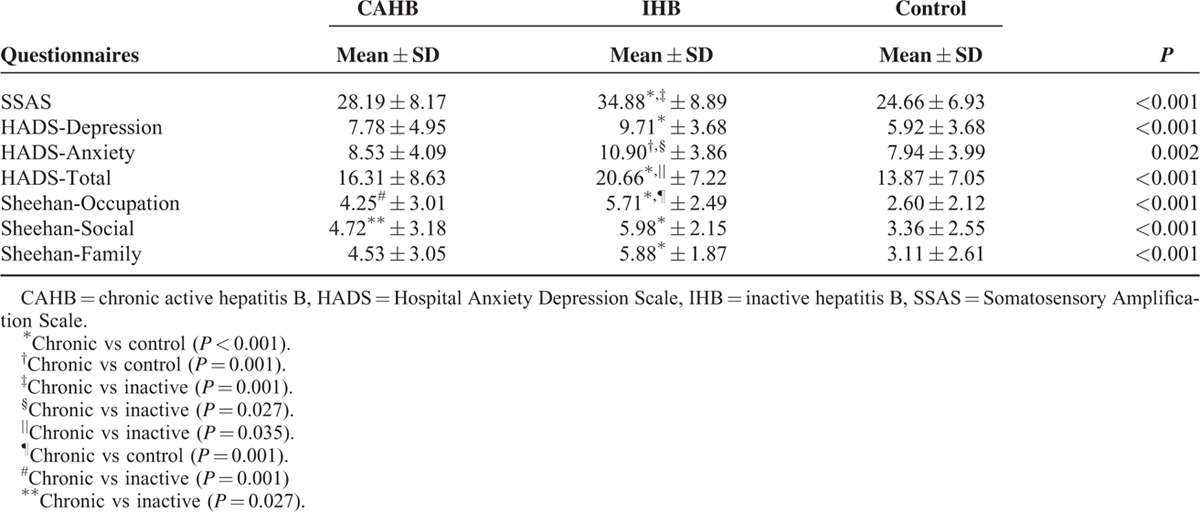
Patients with CAHB had higher levels of somatosensory amplification when compared to control and IHB group (34.88 ± 8.89 vs 24.66 ± 6.93; P < 0.001; 34.88 ± 8.89 vs 28.19 ± 8.17; P = 0.001, respectively). Patients with CAHB had significantly higher HAD total, HAD anxiety and HAD depression scores when compared with control group (20.66 ± 7.22 vs 13.87 ± 7.05; P < 0.001, 10.90 ± 3.86 vs 7.94 ± 3.99; P = 0.002, 9.71 ± 3.68 vs 5.92 ± 3.68; P < 0.001, respectively). Between patients with CAHB and IHB, no significant difference was found with regard to HADS depression score; however, patients with CAHB had significantly higher HADS anxiety and HADS total scores (NS, 10.90 ± 3.86 vs 8.53 ± 4.09; P = 0,027, 20.66 ± 7.22 vs 16.31 ± 8.63; P = 0.035, respectively). Moreover, according to SDS, significant differences were noted in all 3 domains between the CAHB and control groups (P < 0.001), whereas a significant difference was noted only in the work/school domain between the CAHB and IHB groups (P < 0.001). The IHB group had higher scores for the work/school and social life domains of SDS when compared with the control group (4.25 ± 3.01 vs 2.60 ± 2.12; P = 0.008, 4.72 ± 3.18 vs 3.36 ± 2.55; P = 0.047), whereas no significant difference was noted between the IHB and control group in the remaining Sheehan domains, HADS parameters, and SSAS parameters (NS) (Table 2).
TABLE 2.
The Comparisons of SSAS, HADS, SDS Scores of the Groups
DISCUSSION
In the present study, the patients with CAHB demonstrated marked deterioration in depression and anxiety scores, disability levels, and somatosensory amplification.
It was suggested that there was a close correlation between severe liver disease and psychiatric disorders according to the studies. Increased liver damage also increases the tendency towards psychiatric disorders. It occurs more prominently in conditions where severe liver damages develop such as HCC and cirrhosis. Psychiatric disorders are incontrovertible as seen in hepatitis B and C.17 No correlation has been suggested between these disorders and antiviral therapy, but a close correlation with interferon treatment has been suggested.18,19 Moreover, the effect of interferon administration in hepatitis B and C has been studied, and psychiatric disorders have been observed more in those patients with hepatitis C using interferon.20
It is recognized that during chronic diseases, social isolation may occur in patients, predisposing them to development of anxiety and depression due to perception of infectiousness by the general population.21 Patients’ high levels of anxiety may be explained by frequency of follow-up visits, requirement of assessments, reception of treatment, and information on possible complications in patients with chronic hepatitis. Generally, studies on patients with hepatitis B focus on drug treatment and subsequent psychiatric disorders.22–24 Lok et al6 investigated the psychosocial influence of carrying hepatitis B virus in 40 British patients, and found that 90% of the 40 patients were negatively affected with regard to their sexual, occupational, social, family, and physical lives; they observed that the majority of the problems were associated with infectivity. In the study by Kunkel et al,8 46% of patients experienced depressive symptoms, whereas depression was found to be significantly related to liver dysfunction and low psychosocial functioning in a heterogeneous patient group with hepatitis B-related diseases (ie, physically healthy carriers of the virus and patients with HCC and hepatic cirrhosis). The superiority of our study was that patients who were under medical treatment and had additional psychiatric disorders were excluded.
Demir et al7 evaluated 444 patients with hepatitis B (n = 249 healthy carriers; n = 195 chronic patients) by using the Hamilton Depression and Anxiety Scale, and noted significantly higher scores in the chronic hepatitis B group compared with the carriers.
In a study by Inci et al, which was conducted on a total of 82 patients (n = 32 patients with chronic hepatitis B; n = 50 healthy carriers), evaluated with the Beck Depression Scale, the patients with chronic hepatitis B had significantly higher scores when compared with the hepatitis B carriers.25 In another study, patients with chronic hepatitis B were evaluated with the Beck Depression Scale.26
All of studies suggested higher anxiety and depression scores, but no comparison was made to control groups. However, in our study, anxiety and depression scores from the CAHB group were both compared with the healthy control and to the IHB group, suggesting a higher value as compared with both groups. For all groups, depression scores from our study were found independently to be higher than those indicated in the literature, which, in turn, can be accounted by sociodemographic features of patients involved.
The aforementioned studies did not exclude widely used drugs for hepatitis B in active patients. It is known that the use of these drugs, which have been shown to have psychiatric side effects, has an impact on study reliability. The present study was a higher-value study in this regard, since none of our patients had been treated with drugs. Somatosensory amplification and disability have been studied in patients with commonly encountered chronic diseases,27,28 but hepatitis B, also a commonly encountered disease, seems to not have been included in any of these studies. Previous studies have shown that somatosensory amplification may occur in hypochondriasis.10,29 The patients with CAHB developed a concomitant hypochondriasis during this sickness. Therefore, there is a possible relationship between somatosensory amplification and hypochondriasis instead of CAHB. However, the superiority of our study was that patients who were under medical treatment and had additional psychiatric disorders including hypochondriasis were excluded in our study. Consequently, the somatosensory amplification might be developed due to CAHB, but not the hypochondriasis. We believed that we achieved more reliable results because the patients with comorbidities and drug usage were excluded from the study, and the inclusion of healthy control subjects, which was another superior aspect of our study as compared with previous studies, were included.
Thus far, psychiatric symptoms, such as disability and functional deterioration, have not been viewed as important as physical symptoms in chronic diseases during flare-up periods. An understanding of the importance of feelings of self-destruction, disability, and functional deterioration in the course of psychiatric diseases has been recently observed.30 Studies on chronic diseases, such as multiple sclerosis vitiligo, schizophrenia, and AIDS, have revealed the presence of disability and have suggested awareness and precaution for psychiatric symptoms.31,32 Hepatitis B, a commonly occurring disease, which is also endemic in our region, can cause disability that leads to serious loss of manpower. The presence of psychiatric symptoms in hepatitis B, in addition to symptoms related to the disease, indicates that functionality and disability assessments should be included in the follow-ups of patients with hepatitis. Findings of the present study suggest that psychiatric symptoms tend to occur mainly in hepatitis cases with complications, such as cirrhosis or HCC, but that these symptoms also occur in patients with CAHB and in IHB. As expected, the patients with CAHB displayed a higher level of disability when compared with the IHB group.
Although SDS is a significant criterion for assessing the functionality, no study has been conducted to assess the functionality of patients with hepatitis B using SDS so far. It provides us with a more detailed assessment opportunity to use multiple scales by adding such scales. In our study, disorders both in each of 3 SDS fields for those with CAHB, and in occupational and social fields of the same scale for those with IHB suggest that negative expectations, regarding the disease course and possible side effects of the treatment, may lead to disability in patients with CAHB. Although depression and anxiety may be the culprits behind disability, we believe that social isolation stemming from concerns over the infectious nature of the disease may also cause such an outcome.
Somatosensory amplification is just another way of displaying somatic symptoms that may accompany the psychiatric symptoms of chronic diseases. It has been shown that psychosomatic symptoms may increase along with psychiatric disorders such as anxiety and depression.23 The body has a primary role in the individual's interaction and communication with the outside world. In cases where verbal communication is inadequate or blocked, bodily symptoms tend to occur. Particularly in patients with a chronic disease who develop anxiety and depression, the attention tends to be overly concentrated on one's body, leading to disturbing perceptions of normal sensations. Somatosensory amplification may lead to an increase in the time required for diagnosis and unnecessary increase in cost of treatment.33 To our knowledge, no study has been published on somatosensory amplification in patients with hepatitis B. Exaggeration of physical perception is an important area of research. Regarding this issue, Yavuz et al27 studied the relationship of migraine (a chronic disease) to anxiety-depression and somatic senses by using the Depression–Anxiety Stress Scale and the SSAS, and found significantly higher SSAS scores in the group with increased depression-anxiety scores when compared with the control group.
We believe that, in our study, increased somatosensory amplification in CAHB group may have been associated with the anxiety and depression in these patients. Also, another reason of increased somatosensory amplification in CAHB patients could be related to a significant decrease in the somatosensory threshold in their peripheral somatosensory receptors, or in the amplification of their somatosensory responses in the brain via internal neuronal noise sources in the brain and spinal cord.34,35 It would be interesting to perform future experiments to explore these issues in the somatosensory system and also in other sensory modalities.
Moreover, the present study is the first to show elevated levels of somatosensory amplification in patients with hepatitis B. IHB may lead to the isolation of these patients from their social and work lives.6 One US study focusing on patients with hepatitis C showed that the patients felt stigmatized and invaluable.36 Similar to studies in the literature, the present study shows that patients with IHB are at risk for psychiatric disorders while exhibiting no additional psychiatric complaints and disability. Hepatitis B carriers were found to suffer from disability in their social and work lives when compared with control group. Since Turkey has a rapidly developing sociocultural and economic structure, the stigmatization of patients with IHB may be explained by the prevailing beliefs that the disease advances in time and that they might possibly infect the people around them.
Limitations
Although our study has introduced new findings, its limitations are listed as follows at some points: no assessment was performed depending on the results of quantitative HbsAg antigen measurement. Our study was cross-sectional with no follow-up data being examined. Our patient population consisted of individuals with relatively low levels of education and financial capability based on sociodemographic nature of our region as compared with nationwide. Furthermore, we were unable to make a comparison because there were no cut-off values of Sheehan disability and somatosensory amplification scales in the literature. Yet, only an average of these values was compared for 3 groups enrolled.
CONCLUSIONS
In conclusion, we believe that patients with CAHB suffer from amplified bodily sensations and anxiety-depression disorders, both of which have an impact on functionality. Although high levels of psychopathology and somatosensory amplification were not noted in the carrier group, the functionality of members of this group seemed to be compromised. Patients with hepatitis should be evaluated by a psychiatrist for anxiety-depression and somatosensory amplification during routine check-ups. Such evaluations would minimize and/or prevent unnecessary diagnostic and therapeutic interventions for amplified symptoms. In addition, early psychiatric evaluations would be helpful in diagnosing psychiatric conditions before they have had a chance to become severe, thereby improving patients’ quality of life. Future studies focusing on the aspect of comprehensive psychiatric evaluation are required to further investigate the impact of somatosensory amplification and psychiatric disorders in hepatitis-related disability.
Footnotes
Abbreviations: ALT = alanine transaminase, CAHB = chronic active hepatitis B, DNA = deoxyribonucleic acid, HADS = Hospital Anxiety and Depression Scale, HCC = hepatocellular carcinoma, HIV = human immunodeficiency virus, IHB = inactive hepatitis B, NS = nonsignificant, SD = standard deviation, SDS = Sheehan Disability Scale, SSAS = Somatosensory Amplification Scale.
Conflict of interest: The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
REFERENCES
- 1.Dayan S, Tekin A, Tekin R, et al. HBsAg, anti-HCV, anti-HIV 1/2 and syphilis seroprevalence in healthy volunteer blood donors in southeastern Anatolia. J Infect Dev Ctries 2013; 7:665–669. [DOI] [PubMed] [Google Scholar]
- 2.Wells KB, Golding JM, Burnam MA. Psychiatric-disorder in a sample of the general-population with and without chronic medical conditions. Am J Psychiatry 1988; 145:976–981. [DOI] [PubMed] [Google Scholar]
- 3.Harter M, Reuter K, Aschenbrenner A, et al. Psychiatric disorders and associated factors in cancer: results of an interview study with patients in inpatient, rehabilitation and outpatient treatment. Eur J Cancer 2001; 37:1385–1393. [DOI] [PubMed] [Google Scholar]
- 4.Ozkan M, Corapcioglu A, Balcioglu I, et al. Psychiatric morbidity and its effect on the quality of life of patients with chronic hepatitis B and hepatitis C. Int J Psychiatry Med 2006; 36:283–297. [DOI] [PubMed] [Google Scholar]
- 5.Atesci FC, Cetin BC, Oguzhanoglu NK, Karadag F, Turgut H. Psychiatric disorders and functioning in hepatitis B virus carriers. Psychosomatics 2005; 46:142–147. [DOI] [PubMed] [Google Scholar]
- 6.Lok AS, van Leeuwen DJ, Thomas HC, Sherlock S. Psychosocial impact of chronic infection with hepatitis B virus on British patients. Genitourin Med 1985; 61:279–282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Demir NA, Çelik M, Kölgelier S, et al. Comparison of depression and anxiety levels of inactive hepatitis B carriers and chronic hepatitis B patients. Turkish J Psychiatry 2013; 24:248–252. [PubMed] [Google Scholar]
- 8.Kunkel EJ, Kim JS, Hann HW, et al. Depression in Korean immigrants with hepatitis B and related liver diseases. Psychosomatics 2000; 41:472–480. [DOI] [PubMed] [Google Scholar]
- 9.Liver EAFTSOT. EASL clinical practice guidelines: management of chronic hepatitis B virus infection. J Hepatol 2012; 57:167–185. [DOI] [PubMed] [Google Scholar]
- 10.Barsky AJ, Wyshak G, Klerman GL. The somatosensory amplification scale and its relationship to hypochondriasis. J Psychiatric Res 1990; 24:323–334. [DOI] [PubMed] [Google Scholar]
- 11.Barsky AJ, Goodson JD, Lane RS, et al. The amplification of somatic symptoms. Psychosom Med 1988; 50:510–519. [DOI] [PubMed] [Google Scholar]
- 12.Gulec H, Sayar K. Reliability and validity of the Turkish form of the Somatosensory Amplification Scale. Psychiatry Clin Neurosci 2007; 61:25–30. [DOI] [PubMed] [Google Scholar]
- 13.Leon AC, Olfson M, Portera L, et al. Assessing psychiatric impairment in primary care with the Sheehan Disability Scale. Int J Psychiatry Med 1997; 27:93–105. [DOI] [PubMed] [Google Scholar]
- 14.Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983; 67:361–370. [DOI] [PubMed] [Google Scholar]
- 15.Aydemir O, Guvenir T, Kuey L, Kultur S. Validity and reliability of Turkish version of hospital anxiety and depression scale. Turk Psikiyatri Derg 1997; 8:280–287. [Google Scholar]
- 16.Yesilova Y, Bez Y, Arı M, et al. Effects of isotretinoin on obsessive compulsive symptoms, depression, and anxiety in patients with acne vulgaris. J Dermatological Treatment 2012; 23:268–271. [DOI] [PubMed] [Google Scholar]
- 17.Kuo G, Choo QL, Alter HJ, et al. An assay for circulating antibodies to a major etiologic virus of human non-A, non-B hepatitis. Science 1989; 244:362–364. [DOI] [PubMed] [Google Scholar]
- 18.Balfour HH., Jr Antiviral drugs. N Engl J Med 1999; 340:1255–1268. [DOI] [PubMed] [Google Scholar]
- 19.Dusheiko G. Side effects of alpha interferon in chronic hepatitis C. Hepatology 1997; 26 (3 suppl 1):112S–121S. [DOI] [PubMed] [Google Scholar]
- 20.Davis GL, Balart LA, Schiff ER, et al. Assessing health-related quality of life in chronic hepatitis C using the Sickness Impact Profile. Clin Therapeut 1994; 16:334–343.[discussion 271–332]. [PubMed] [Google Scholar]
- 21.Kibrisli E, Bez Y, Yilmaz A, et al. High social anxiety and poor quality of life in patients with pulmonary tuberculosis. Medicine 2015; 94:e413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ho SB, Nguyen H, Tetrick LL, et al. Influence of psychiatric diagnoses on interferon-alpha treatment for chronic hepatitis C in a veteran population. Am J Gastroenterol 2001; 96:157–164. [DOI] [PubMed] [Google Scholar]
- 23.Marcellin P, Lau GK, Zeuzem S, et al. Comparing the safety, tolerability and quality of life in patients with chronic hepatitis B vs chronic hepatitis C treated with peginterferon alpha-2a. Liver Int 2008; 28:477–485. [DOI] [PubMed] [Google Scholar]
- 24.Çeler A, Kara İH, Baltacı A, Çeler H. Investigation of the relationship of job satisfaction and depression level among medical faculty research assistants. Konuralp Medical J 2015; 7:125–133. [Google Scholar]
- 25.Inci A. The investigation of the depression levels of chronic hepatitis B patients. Viral Hepatitis J 2013; 19: [Google Scholar]
- 26.Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology 2001; 34:1225–1241. [DOI] [PubMed] [Google Scholar]
- 27.Yavuz BG, Aydinlar EI, Dikmen PY, et al. Association between somatic amplification, anxiety, depression, stress and migraine. J Headache Pain 2013; 14:10.1186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Carpenter JS, Igega CM, Otte JL, et al. Somatosensory amplification and menopausal symptoms in breast cancer survivors and midlife women. Maturitas 2014; 78:51–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Jimenez Moron D, Saiz Ruiz J. [Amplification: somatosensory or cognitive?]. Actas luso-espanolas de neurologia, psiquiatria y ciencias afines 1996; 24:1–6. [PubMed] [Google Scholar]
- 30.Weissman MM. The assessment of social adjustment. A review of techniques. Arch Gen Psychiatry 1975; 32:357–365. [DOI] [PubMed] [Google Scholar]
- 31.Ertekin Ö, Özakbaş S, İdiman E, et al. The effects of low and severe disability on walking abilities and quality of life in multiple sclerosis patients: 6-month follow-up study. Arch Neuropsychiatry 2013; 50:23–29. [Google Scholar]
- 32.Bennett L, Rose D, Jackson A, et al. Psychological and socio-medical aspects of HIV/AIDS: a reflection on publications in AIDS care (1989–1995). AIDS Care 1998; 10:115–121. [DOI] [PubMed] [Google Scholar]
- 33.Özen EM, Serhadlı ZN, Türkcan AS, Ülker GE. Somatization in depression and anxiety disorders. The J Psychiatry Neurolog Sci 2010; 23:60–65. [Google Scholar]
- 34.Manjarrez E, Diez-Martinez O, Mendez I, et al. Stochastic resonance in human electroencephalographic activity elicited by mechanical tactile stimuli. Neurosci Lett 2002; 324:213–216. [DOI] [PubMed] [Google Scholar]
- 35.Manjarrez E, Rojas-Piloni G, Mendez I, et al. Stochastic resonance within the somatosensory system: effects of noise on evoked field potentials elicited by tactile stimuli. J Neurosc 2003; 23:1997–2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zickmund S, Masuda M, Ippolito L, et al. They treated me like a leper. J Gen Intern Med 2003; 18:835–844. [DOI] [PMC free article] [PubMed] [Google Scholar]