

Abstract
[Purpose] The aim of this study was to analyze the crutch position in the horizontal plane to confirm the stability of the axillary pad during double-crutch walking. [Subjects] Twelve healthy young subjects (6 males and 6 females). [Methods] The subjects were asked to walk in a straight line, using double crutches, for a distance of 5 m, 5 times. Crutch position data were obtained using four infrared reflective markers attached to both crutches (two markers each on both crutches). The crutch angles of each subject were compared across three time points during the crutch stance phase (crutch contact, mid stance, and crutch off). [Results] Crutch angles of each of the two crutches were significantly different across the crutch stance phase of 11 of the 12 subjects. Phasic differences were shown by 4 of the 12 subjects, and a strong correlation was observed between the left and right crutch angles of all subjects. [Conclusion] External rotation of the crutch throughout the stance phase was very important for keeping the axillary pad in the axilla, not only for single-crutch walking, but also for double-crutch walking. In addition, symmetry of the crutch positioning is one of the most important factors for safe double-crutch walking.
Key words: Crutch walking, Crutch position, Axillary pad stability
INTRODUCTION
The axillary crutch is an assistive device that supports the gait of patients with lower limb impairments. However, crutch walking has several unresolved issues, including the appropriate length of the crutch1), crutch palsy2), palmar pain during crutch weight bearing3), and deviation of the axillary pad from the axilla during the crutch stance phase4). In particular, the axillary pad often deviates from the axilla during the crutch stance phase, and this is one of the main issues for safe crutch walking. If the axillary pad is not held firmly against the chest wall, the crutch tends to be easily displaced from the axilla, possibly leading to falls. Therefore, the cause of the axillary pad deviation from the axilla needs be identified to ensure user safety. We previously showed that external rotation of the crutch throughout the crutch stance phase ensured that the axillary pad was held tightly against the chest wall during single-crutch walking5). However, this observation is thought to apply only to single-crutch walking. Thus, the aim of this study was to analyze the crutch position in the horizontal plane to confirm the stability of the axillary pad during double-crutch walking.
SUBJECTS AND METHODS
Twelve healthy young subjects were enrolled in this study (6 males and 6 females; mean age, 22.1 ± 0.5 years; mean height, 168.7 ± 8.0 cm; mean weight, 63.3 ± 11.3 kg). This study was performed in accordance with the ethical principles of the Declaration of Helsinki and was approved by the ethics committee of Kyushu University of Nursing and Social Welfare. All subjects received a description of this study and provided their written, informed consent before participating in this study. Before carrying out the measurements, the crutches were adjusted to the appropriate length for each subject, and adequate practice of crutch walking was done. The appropriate crutch length was determined using the standard method described by Rusk and Lowman6). Double-crutch walking was performed using a three-point gait (swing-through gait) with a pseudo-affected left leg.
For this study, a new crutch was created that had stepless adjustments for the height of the hand grip and the crutch length to enable its adaptation to all subjects. The new crutch had an extension that was attached to the axillary pad so that a straight line connecting the two infrared reflective markers indicated the long axis of the axillary pad (Fig. 1).
Fig. 1.
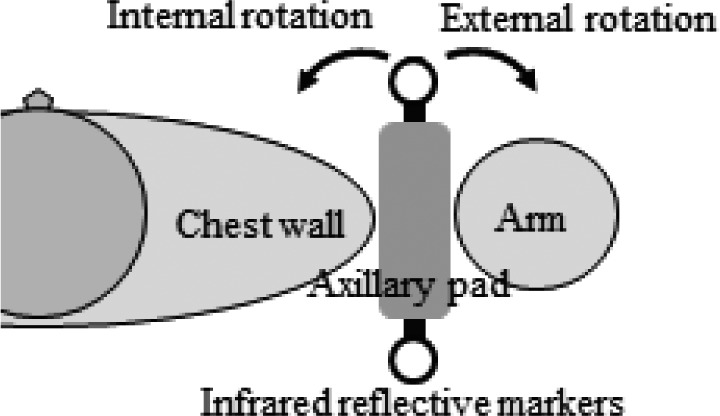
Schematic diagram of the crutch position
The measuring system consisted of a three-dimensional motion capture system (Vicon Nexus, UK), comprising nine infrared cameras and six force plates (AMTI, USA) and a digital video camera (JVC, Japan). The sampling rates were 100 Hz. The crutch position in the horizontal plane was defined as the angle between the sagittal (YZ) plane and the long axis of the axillary pad. The direction of the crutch position was determined as internal rotation when the crutch turned toward the body, and external rotation when the crutch turned away from the body (Fig. 1). Crutch angles and ground reaction forces were measured. The crutch position data were obtained using four infrared reflective markers attached to both crutches (two markers each on the right and left crutches), and the results were calculated using the data collected by the motion capture system. The positions of both crutches, that were measured during the crutch walking, were calculated using the data of the ground reaction forces. Crutch angles were normalized against 100% of the crutch-walking cycle. All subjects were asked to perform a 5-m straight walk using double-crutch walking. No instructions regarding step length and walking speed were provided. The participants repeated the activity five times.
Repeated-measures analysis of variance and Tukey’s honest significance test were used to compare crutch angles across three time points during the crutch stance phase (crutch contact, mid stance, and crutch off) of each subject. All data were analyzed using standard statistics software (IBM SPSS Statistics ver. 19.0). P values of less than 0.05 were considered significant. Cross-correlation coefficients were used to examine the symmetry of the left and right crutch angles during the crutch walking cycle of each subject.
RESULTS
Table 1 shows the crutch angles of both sides in each phase of the crutch stance of each subject. Crutch angles of each of the two crutches were significantly different across the crutch stance phase of 11 of the 12 subjects. (all subjects except subject 12). Post hoc analysis showed significant differences for 6 of the 11 subjects (subjects 2, 3, 6, 7, 9, and 10) in three comparisons (crutch contact vs. mid stance, crutch contact vs. crutch off, and mid stance vs. crutch off) on both sides. Four other subjects (subjects 1, 4, 5, and 8) showed significant differences in three comparisons on one side, whereas the other side showed significant differences in two of three comparisons (significance was always observed in the comparison of crutch contact vs. crutch off). The remaining subject (subject 11) showed significant differences in one or two of three comparisons on both sides (significance was always observed in the comparison of crutch contact vs. crutch off). Finally, subject 12 showed significant differences in three comparisons on one side, but the other side did not show significant differences in these three comparisons.
Table 1. Crutch angles of each phase of the crutch walking of each subject.
| Subject | Crutch angle (degrees) | Direction of crutch rotation between crutch contact and crutch off |
|||
|---|---|---|---|---|---|
| Crutch contact | Mid stance | Crutch off | |||
| 1 | Rt. | −9.3 ± 1.9 | −3.9 ± 2.1* | 0.3 ± 2.3*, # | External rotation |
| Lt. | −7.8 ± 2.0 | −6.7 ± 0.9 | −2.7 ± 2.6*, # | ||
| 2 | Rt. | −9.2 ± 1.7 | 0.0 ± 1.1* | 5.4 ± 1.4*, # | |
| Lt. | −11.7 ± 2.2 | −5.0 ± 1.5* | −0.3 ± 4.9*, # | ||
| 3 | Rt. | −14.0 ± 1.5 | −5.2 ± 1.2* | −1.4 ± 2.0*, # | |
| Lt. | −12.8 ± 1.5 | −3.2 ± 1.2* | 0.7 ± 2.0*, # | ||
| 4 | Rt. | −5.2 ± 1.4 | 2.0 ± 1.9* | 2.6 ± 1.2* | |
| Lt. | −5.6 ± 1.3 | −1.7 ± 2.1* | 2.6 ± 4.1*, # | ||
| 5 | Rt. | −1.5 ± 2.7 | 3.8 ± 1.4* | 6.1 ± 2.7* | |
| Lt. | −1.0 ± 2.1 | 3.9 ± 1.7* | 9.9 ± 2.1*, # | ||
| 6 | Rt. | −4.8 ± 1.9 | −0.1 ± 5.9* | 5.9 ± 3.4*, # | |
| Lt. | −7.5 ± 2.4 | −1.1 ± 1.1* | 4.7 ± 2.0*, # | ||
| 7 | Rt. | −6.3 ± 1.9 | −0.7 ± 2.7* | 3.9 ± 3.1*, # | |
| Lt. | −11.5 ± 3.6 | −2.9 ± 4.6* | 2.4 ± 3.9*, # | ||
| 8 | Rt. | −9.1 ± 3.1 | −3.2 ± 2.5* | 9.2 ± 2.9*, # | |
| Lt. | −3.1 ± 2.0 | −1.6 ± 2.0 | 9.5 ± 2.4*, # | ||
| 9 | Rt. | −3.8 ± 2.1 | 3.9 ± 1.7* | 12.2 ± 5.2*, # | |
| Lt. | −5.0 ± 2.9 | 2.1 ± 1.2* | 6.2 ± 1.6*, # | ||
| 10 | Rt. | −7.0 ± 1.0 | −2.0 ± 3.5* | 2.8 ± 2.0*, # | |
| Lt. | −4.7 ± 0.5 | 2.0 ± 2.4* | 12.8 ± 1.7*, # | ||
| 11 | Rt. | −12.9 ± 1.7 | −10.4 ± 1.2 | −5.4 ± 2.2*, # | |
| Lt. | −14.5 ± 0.5 | −11.4 ± 1.1 | −10.2 ± 3.4* | ||
| 12 | Rt. | −7.3 ± 2.5 | −1.8 ± 3.5* | 3.9 ± 5.1*, # | External rotation |
| Lt. | −0.7 ± 2.0 | 5.9 ± 5.0 | 5.6 ± 3.6 | No rotation | |
Data are means ± SD. *p<0.05 compared with crutch contact. #p<0.05 compared with mid stance. Negative values indicate internal rotation, positive values indicate external rotation.
Table 2 shows the correlation coefficients and phasic differences between the left and right crutch angles during the crutch-walking cycle of each subject. A strong correlation was observed between the left and right crutch angles in all subjects. However, phasic differences were shown by 4 of the 12 subjects (subjects 1, 4, 5 and 11), and subject 4 had an especially large phasic difference of 6%.
Table 2. Correlation coefficients and phasic differences between the left and right crutch angles of each subject.
| Subject | CC | Phasic difference |
|---|---|---|
| 1 | 0.85 | 1% |
| 2 | 0.95 | 0% |
| 3 | 0.95 | 0% |
| 4 | 0.90 | 6% |
| 5 | 0.91 | 1% |
| 6 | 0.93 | 0% |
| 7 | 0.93 | 0% |
| 8 | 0.98 | 0% |
| 9 | 0.95 | 0% |
| 10 | 0.89 | 0% |
| 11 | 0.90 | 1% |
| 12 | 0.87 | 0% |
CC: correlation coefficient. Phasic difference as a percentage of the whole crutch-walking cycle.
DISCUSSION
Sasaki et al. reported that, when the shoulder joint was positioned in an internally rotated position, the axillary pad was not fixed against the chest wall and could easily slide backward from the axilla4). In other words, it is very important for safe crutch walking that the axillary pad is kept in the axilla during crutch walking. In an earlier study, we suggested that analysis of the crutch position in the horizontal plane during single-crutch walking would be necessary to ensure safe crutch walking5). We also showed that external rotation of the crutch throughout the crutch stance phase ensured that the axillary pad was held tightly against the chest wall during single-crutch walking. The reason for this is that external rotation of the crutch throughout the crutch stance phase is related to the shape of the chest wall (Fig. 2). That is, because the chest wall is rounded, the axillary pad moves along the chest wall. However, this only applies to single-crutch walking. Therefore, the aim of this study was to analyze the crutch position in the horizontal plane to confirm the stability of the axillary pad during double-crutch walking.
Fig. 2.
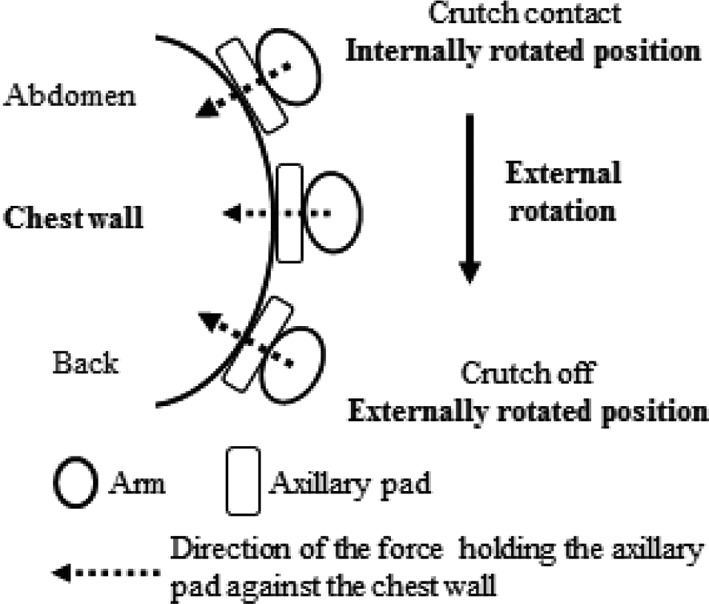
Relationship between the chest wall and the position of the axillary pad during the crutch stance phase
This study found that the crutch rotated externally in the horizontal plane during the crutch stance phase of 11 subjects, although there was inter-subject variation in the angle. We consider that these variations are dependent on: crutch tip contact position, transfer and/or position of center of gravity, and difference of crutch walking pattern (step length, walking speed). Regarding the crutch tip contact position, the crutch angle is posited to become externally rotated when the width between the left and right crutch tips becomes wider. Conversely, when the width becomes narrower, the crutch angle tends to be internally rotated. In both cases, external rotation of the crutch throughout the stance phase probably ensured that the axillary pad was held tightly against the chest wall during double-crutch walking, as in single-crutch walking. In the one atypical subject (subject 12), the crutch rotated externally on one side, but did not rotate on the other side during the crutch stance phase. In this case, it is likely the crutch deviated from the chest wall on the side that did not rotate externally, and the subject’s crutch gait was unstable. In a review of the video recordings, subject 12 was one of the subjects who lacked skill in crutch walking, even though sufficient training was performed in advance; i.e., subject 12 exhibited many failures of the measurement and large body sway during crutch walking. Therefore, external rotation of the crutch throughout the stance phase appears to be very important for keeping the axillary pad in the axilla, not only during single-crutch walking, but also during double-crutch walking.
In double-crutch walking, the symmetry of the right and left crutch positions appears to be an important factor of safe crutch walking, in addition to external rotation of the crutches. Figure 3 shows the ideal crutch transition during double-crutch walking. As shown in Fig. 3, the symmetry of the right and left crutch positions is required for straight walking throughout double-crutch walking. If the positions of both crutches are not synchronized, straight walking becomes unstable because the direction of the force holding the axillary pad against the chest wall becomes asymmetrical. The present study confirmed that there was a similarity between the left and right crutch angles during crutch walking of all subjects. However symmetry was not demonstrated by several subjects (Table 2). Incidentally, assuming the crutch-walking cycle is the same as the normal walking cycle, the phase from crutch contact to mid stance is about 30% of whole crutch-walking cycle. This phase is a very important phase for weight bearing. Further, the length of this phase is less than one second. As shown in Table 2, a phasic difference of 6% was exhibited in this phase by subject 4. It means that there was a considerable discrepancy in the symmetry of the left and right crutch angles in this phase for subject 4. Therefore, it is likely that the crutch stance phase of subject 4 was negatively impacted because this subject lacked skill in crutch walking. It is our opinion that symmetry of crutch positioning is one of the important factors for safe double-crutch walking. These results may lead to the prevention of falls among crutch users.
Fig. 3.
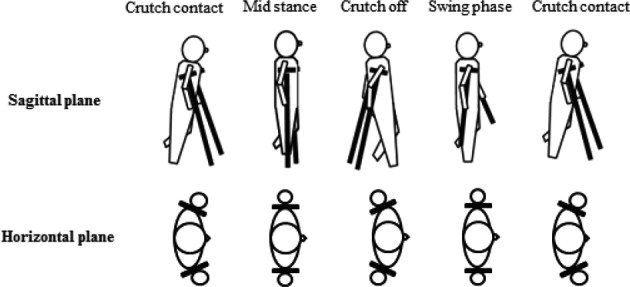
The ideal crutch transition during crutch walking (conceptual illustration)
In conclusion, the crutch positions of both sides were measured in the horizontal plane in order to confirm the stability of the axillary pad during double-crutch walking. External rotation of the crutch throughout the stance phase is very important for keeping the axillary pad in the axilla, not only during single-crutch walking, but also during double-crutch walking. In addition, symmetry of crutch positioning appears to be one of the important factors for safe double-crutch walking. These results may lead to the prevention of falls among crutch users. However, we think our findings are not sufficient to recommend their application in clinical settings, because the subjects were healthy. Therefore, the selection of subjects requiring crutches is needed to confirm our findings in further studies.
Acknowledgments
Part of this work was supported by JSPS KAKENHI Grant Number 25560273 and Kitakyushu Foundation for the Advancement of Industry, Science and Technology (FAIS).
REFERENCES
- 1.Crosbie J, Armstrong E, Kempson J: Is walking aid height critical? Aust J Physiother, 1992, 38: 261–266. [DOI] [PubMed] [Google Scholar]
- 2.Raikin S, Froimson MI: Bilateral brachial plexus compressive neuropathy (crutch palsy). J Orthop Trauma, 1997, 11: 136–138. [DOI] [PubMed] [Google Scholar]
- 3.Sala DA, Leva LM, Kummer FJ, et al. : Crutch handle design: effect on palmar loads during ambulation. Arch Phys Med Rehabil, 1998, 79: 1473–1476. [DOI] [PubMed] [Google Scholar]
- 4.Sasaki S, Nose Y, Shimada S, et al. : The biomechanics of crutches and canes. Rigaku Ryoho, 2000, 17: 814–823(in Japanese). [Google Scholar]
- 5.Nagasaki T, Katoh H, Arizono H, et al. : Analysis of crutch position in the horizontal plane to estimate the stability of the axillary pad in the axilla during single-crutch walking. J Phys Ther Sci, 2014, 26: 1753–1756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lowman EW, Rusk HA: Self-help devices, crutch prescription: measurement. Postgrad Med, 1962, 31: 303–305. [Google Scholar]