

Abstract
The present study reports the case of a 79-year-old woman manifesting skin changes, a pancreatic neoplasm, enlarged lymph nodes, an eyelid mass and interstitial pneumonia over a 30-year period. At 2 months before admission to our hospital, the patient presented rapid vision loss in the left eye. Left optic nerve atrophy with a focal hyperintense lesion was documented on a T2-weighted magnetic resonance imaging (MRI) scan, and visual evoked potential implicit times were prolonged. Elevated serum immunoglobulin G4 (IgG4) concentrations and the presence of enriched IgG4-positive plasma cells in the lymph nodes established the diagnosis of IgG4-related optic neuropathy. Following oral treatment with methylprednisolone, the serum IgG4 levels fell to normal levels, and the left eye visual acuity improved to a level that remained stable over a 1-year follow-up period. After 4 months of methylprednisolone administration, the optic nerve appeared to be normal on an MRI scan. Prior reports on IgG4-related optic neuropathy involved an infiltrating mass, which was not observed in the present case. Similarly to the current study, previous cases have responded to treatment with glucocorticoids, indicating that the underlying mechanism of the disease may be common.
Keywords: immunoglobulin G4-related disease, optic nerve, vision loss, immunoglobulin G4, biopsy
Introduction
Immunoglobulin gG4-related disease (IgG4-RD) is a recently described disease entity characterized by tumefactive lesions, abundant tissue lymphoplasmacytic and IgG4-positive plasma cell infiltration, storiform fibrosis and elevated serum IgG4 concentrations (1). Since autoimmune pancreatitis, associated with high serum IgG4 expression levels, was first reported in 2001 (2), IgG4-RD has been described in various organ systems, including the pancreas, kidney, biliary tree, salivary glands and the nervous system (1,3–5). The disease is more common in middle-aged and elderly males (6). The incidence rate of IgG4-RD has not been established because of the relative rarity of this diagnosis (6). IgG4-RD typically responds significantly to treatment with immunosuppressants (7); treatment with systemic steroids is recommended, and a longer duration of treatment with steroids may decrease the rate of recurrence (7–9).
While optic nerve involvement is rare, a series of recent studies have reported the presence of a mass around the orbit (10–13). In the present study, a serologically and histopathologically documented IgG4-RD case is reported, which presented with rapid progressive optic neuropathy with no mass around the orbit. The current case also responded to glucocorticoid treatment, providing new insights into this form of IgG4-RD.
Case report
A 79-year-old woman was admitted at the China-Japan Friendship Hospital (Beijing, China) in October 2013, complaining of rapid loss of vision in the left eye that persisted for two months. The study was approved by the Institutional Review Board of the China-Japan Friendship Hospital, and written informed consent was obtained from the patient. Approximately 30 years earlier, the patient presented with symmetrical spot-like vitiligo of the skin around the two ankles, which has spread upward on both legs and lower abdomen. The patient was diagnosed with pancreatic neoplasm and diabetes 4 years before admission for vision loss, and treatment with oral hypoglycemic agents (30 mg acarbose, thrice daily for 4 years; Bayer AG, Leverkusen, Germany) was initiated to maintain normal blood glucose levels. In addition, the patient developed enlarged right cervical and double subaxillary painless lymph nodes 3.5 years before admission, and a right upper palpebral mass 3 years ago. Additional features of the patient's medical history were coronary artery disease for the past 8 years and hypertension for the past 7 years, which were treated with oral agents (30 mg adalat daily for 7 years; Bayer). Furthermore, the patient had undergone bilateral cataract surgery 7 years prior to admission; thereafter, visual acuity, as measured with a standard logarithmic letter chart ~6 months after cataract surgery, was maintained at 0.6–0.8/1.5 in both eyes.
During the initial evaluation in October 2013, the patient was awake, alert and oriented to time, place and persons. Symmetrical patchy depigmentation was identified on the legs and the lower abdomen. Submandibular and subaxillary enlarged lymph nodes were palpated. The results of a neurological examination (cranial nerve, motor and sensor system examinations) were normal, with the exception of vision loss on the left eye. At this point in time, visual acuity was 0.03/1.5 (left eye) and 0.6/1.5 (right eye). Dilated fundus examination by direct ophthalmoscopy revealed optic atrophy in the left eye and arteriosclerosis in both eyes.
Immunoglobulin G (IgG) and IgG4 serum levels were elevated to 3,150 and 2,440 mg/dl on admission, respectively (IgG reference range, 694–1,620 mg/dl; IgG4 reference range, 3.0–201 mg/dl). The erythrocyte sedimentation rate of the patient was 53 mm/h (reference range, 0–20 mm/h). Normal immunofixation electrophoresis was noted in blood and urine samples. Visual evoked potentials (VEPs; Medtronic, Minneapolis, MN, USA) were obtained to a 26-degree square pattern of 1-degree high contrast black and white checks that reversed at 1 Hz. VEP implicit times were prolonged when the left eye was stimulated, but not when the right eye was tested (Fig. 1). At presentation, cranial magnetic resonance imaging (MRI; Gyroscan 1.5 T; Philips Healthcare, DA Best, The Netherlands) showed atrophy of the left optic nerve with a focal hyperintense lesion, as shown in a T2-weighted image (Fig. 2A). The MRI analysis revealed the absence of any mass surrounding the optic nerve or any other orbital areas. Furthermore, a thoracic computed tomography (CT; Aquilion; Toshiba, Tokyo, Japan) scan showed diffused interstitial pneumonia. No abnormalities were detected on fundus fluorescein angiography, electromyography, abdominal-pelvic CT, specific autoimmune testing, hematological examination, serum angiotensin-converting enzyme (ACE) and other immunoglobulin (IgA, IgM and IgE) levels.
Figure 1.

Visual evoked potentials (VEPs) obtained at presentation upon left (upper waveform) or right (lower waveform) eye stimulation (1 Hz contrast reversal of 1 degree black and white checks). VEP obtained upon left eye stimulation was delayed and reduced in amplitude. Major components of the response (N75, P100 and N145) are indicated.
Figure 2.
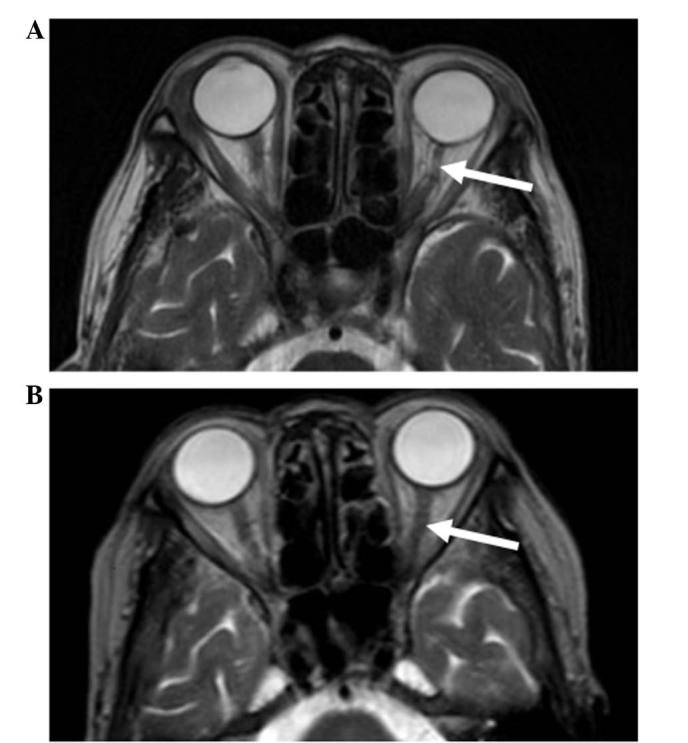
Cranial magnetic resonance T2-weighted images obtained: (A) At presentation, showing a thinner left optic nerve (arrow) compared with the right optic nerve, and presence of a hyperintense lesion; and (B) after 4 months of oral methylprednisolone therapy, showing that the appearance of the left optic nerve (arrow) was similar to that of the right optic nerve and the hyperintense lesion had resolved.
Clinicopathological examination of cervical lymph node by needle biopsy revealed diffuse lymphoplasmacytic infiltration and storiform fibrosis. An immunohistochemical stain against IgG4 demonstrated that the number of IgG4-positive plasma cells were elevated to >50 cells per high-power field (Fig. 3A), as compared to the 0–20 cells per high-power field observed in normal biopsy specimens (14,15). In addition, an IgG4/IgG plasma cell ratio of >40% was observed (Fig. 3B), which was much higher compared with the 6% ratio typically observed in normal subjects. A labial gland biopsy revealed lymphoplasmacytic focal infiltration in the salivary gland stroma with mild changes in the acinus and ducts, but was negative for IgG4. Upon analysis of the skin biopsy, IgG4-positive plasma cells were absent from the dermis and epidermis.
Figure 3.
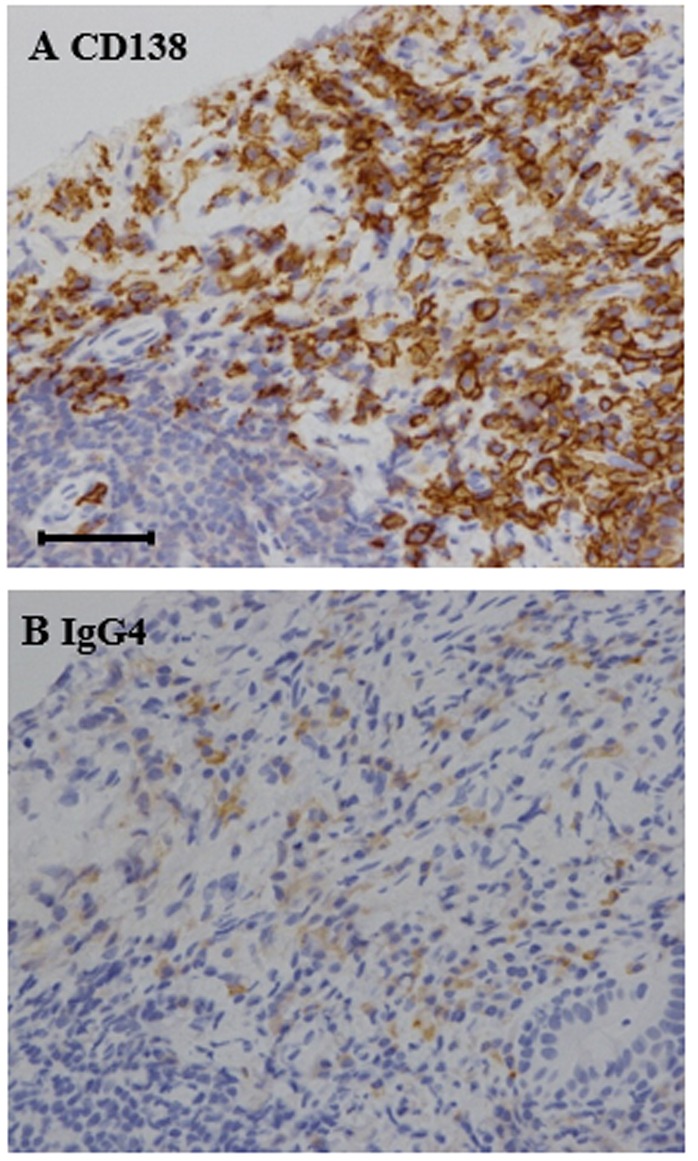
Histopathological findings in cervical lymph node biopsy. (A) CD138 immunohistochemical staining (brown) identified plasma cellular infiltration in the cervical lymph node (magnification, ×400). (B) Immunoglobulin G4 (IgG4) immunohistochemical staining (brown) labeled a large number of IgG4-positive plasma cells among the inflammatory infiltrates (magnification, ×400). The ratio of IgG4/IgG cells was >40%, which was much higher compared with the 6% ratio typically observed in normal subjects. Scale bar=50 µm.
The patient was diagnosed with IgG4-RD and began oral administration of methylprednisolone (Pfizer, Inc., New York, NY, USA) at 40 mg/day (1 mg/kg/day), followed by gradual reduction of the dose (~1 pill per month reduction) within a period of 24 weeks, maintaining a dose of 4 mg/day for ~1 year. This treatment resulted in a decrease in serum IgG and IgG4 levels to 732 mg/dl and 259 mg/dl, respectively. The visual acuity in the left eye was stabilized and improved to 0.3/1.5, which persisted over a 1-year post-treatment period. After 4 months of therapy, the left optic nerve had a normal appearance on an MRI scan (Fig. 2B). The last follow-up date was January 2014.
Discussion
The present study reported the case of a woman with unilateral vision loss in addition to involvement of salivary gland, lymph node, lung, pancreas, eyelid and skin. Other systemic diseases that may cause similar vision loss include the Vogt-Koyanagi-Harada syndrome, sarcoidosis, Sjögren's syndrome and systemic vasculitis. In the present case, these conditions were excluded by normal fundus fluorescein angiography, negative serum ACE, specific autoantibody testing and labial biopsy. Lymphoma was also excluded by normal hematological testing. The diagnosis of the patient conformed to the 2011 diagnostic criteria for IgG4-RD based on organs affected, enriched IgG4-positive plasma cells in involved tissues and high serum IgG4 concentration (7). Using the key words ‘optic nerve’ and ‘IgG4-related disease’, a literature search was performed using PubMed (http://www.ncbi.nlm.nih.gov/pubmed).
Orbital involvement in IgG4-RD has been previously reported to affect nearly every orbital structure, including lacrimal glands, extra-ocular muscles and the trigeminal nerve (16,17). The term IgG4-related ophthalmic disease (IgG4-ROD) has been suggested for IgG4-RD with ophthalmic involvement (18). According to Kashii (18), IgG4-ROD is characterized by bilateral lacrimal gland enlargement accompanied by three distinctive features, including infraorbital nerve enlargement, extraocular myositis and compressive optic neuropathy. Comparing the characteristics of the patient of the current study to this classification, we note that an upper eyelid mass was present, which was consistent with lacrimal gland enlargement; however, this disappeared spontaneously and prior to methylprednisolone treatment. The patient subsequently developed rapid loss of vision only on the left eye. Cranial MRI scans documented the presence of optic nerve atrophy with focal lesion, but did not identify any masses infiltrating the optic nerve or orbit, distinguishing this case from previous cases (summarized in Table I). We hypothesize that the underlying pathophysiologic mechanism may involve inflammatory demyelination of the optic nerve based on the findings of MRI, VEP implicit time delays and positive response to glucocorticoid treatment. Although this mechanism was not confirmed through optic nerve biopsy, this hypothesis raises a novel pathogenic feature that should be addressed in future cases of IgG4-related optic neuropathy.
Table I.
Summary of recent literature documenting optic nerve involvement in immunoglobulin G4-related disease.
| Authors | Clinical presentation | Mechanism | Treatment | Refs. |
|---|---|---|---|---|
| Takahashi et al | 1 case of bilateral blurred vision with orbital apices masses and sinusitis | Compressive optic neuropathy | Prednisolone | (10) |
| Takahira et al | 2 cases with optic neuropathy | Optic neuropathy infiltrated by surrounding masses | Steroids | (11) |
| Ramirez et al | 1 case of bilateral vision loss with headache | Optic neuropathy secondary to hypertrophic pachymeningitis | Steroids | (12) |
| Sogabe et al | 6 cases of visual disturbance due to optic nerve disturbance | Optic neuropathy compressed by supraorbital nerve lesion in 2 patients; localized orbital mass in 2 patients; diffuse orbital fat lesion in 1 patient; enlarged extraocular muscle; and localized orbital mass in 1 patient | N/A | (13) |
IgG4-ROD usually responds favorably to systemic glucocorticoids (19). A recent case has shown evident improvement to normal vision after a 3-month course of steroid treatment (10). By contrast, the vision of the current patient did not reach normal levels within the 1-year follow-up period. This may reflect the presence of an irreversible optic atrophy or reflect more severe fundus arteriosclerosis in the left eye of the patient.
In conclusion, the current study presented a case of IgG4-RD with ocular symptoms that were rapidly improved by glucocorticoid treatment. The current case did not involve focal mass infiltration of any orbital structure. By broadening the spectrum of IgG4-ROD, the present case provides new information regarding the underlying pathogenic mechanisms of IgG4-related optic neuropathy.
Acknowledgements
The authors would like to thank their colleagues from the Department of Rheumatology and Respirology (China-Japan Friendship Hospital, Beijing, China) for their support. The present study was sponsored by the Wu Jieping Medical Foundation (grant no. 1117) and the Yough Foundation of the China-Japan Friendship Hospital (grant no. 2015-1-QN-12).
References
- 1.Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012;366:539–551. doi: 10.1056/NEJMra1104650. [DOI] [PubMed] [Google Scholar]
- 2.Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, Fukushima M, Nikaido T, Nakayama K, Usuda N, Kiyosawa K. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344:732–738. doi: 10.1056/NEJM200103083441005. [DOI] [PubMed] [Google Scholar]
- 3.Kamisawa T, Okamoto A. IgG4-related sclerosing disease. World J Gastroenterol. 2008;14:3948–3955. doi: 10.3748/wjg.14.3948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wallace ZS, Carruthers MN, Khosroshahi A, Carruthers R, Shinagare S, Stemmer-Rachamimov A, Deshpande V, Stone JH. IgG4-related disease and hypertrophic pachymeningitis. Medicine (Baltimore) 2013;92:206–216. doi: 10.1097/MD.0b013e31829cce35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ohyama K, Koike H, Iijima M, Hashimoto R, Tomita M, Kawagashira Y, Satou A, Nakamura S, Sobue G. IgG4-related neuropathy: A case report. JAMA Neurol. 2013;70:502–505. doi: 10.1001/jamaneurol.2013.658. [DOI] [PubMed] [Google Scholar]
- 6.Wallace ZS, Deshpande V, Mattoo H, Mahajan VS, Kulikova M, Pillai S, Stone JH. IgG4-related disease: Clinical and laboratory features in one hundred twenty-five patients. Arthritis Rheumatol. 2015;67:2466–2475. doi: 10.1002/art.39205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Islam AD, Selmi C, Datta-Mitra A, Sonu R, Chen M, Gershwin ME, Raychaudhuri SP. The changing faces of IgG4-related disease: Clinical manifestations and pathogenesis. Autoimmun Rev. 2015;14:914–92. doi: 10.1016/j.autrev.2015.06.003. [DOI] [PubMed] [Google Scholar]
- 8.Zen Y, Nakanuma Y. IgG4-related disease: A cross-sectional study of 114 cases. Am J Surg Pathol. 2010;34:1812–1819. doi: 10.1097/PAS.0b013e3181f7266b. [DOI] [PubMed] [Google Scholar]
- 9.Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, Matsui S, Yoshino T, Nakamura S, Kawa S, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012;22:21–30. doi: 10.3109/s10165-011-0571-z. [DOI] [PubMed] [Google Scholar]
- 10.Takahashi Y, Kitamura A, Kakizaki H. Bilateral optic nerve involvement in immunoglobulin G4-related ophthalmic disease. J Neuroophthalmol. 2014;34:16–19. doi: 10.1097/WNO.0b013e3182a304f4. [DOI] [PubMed] [Google Scholar]
- 11.Takahira M, Ozawa Y, Kawano M, Zen Y, Hamaoka S, Yamada K, Sugiyama K. Clinical aspects of IgG4-related orbital inflammation in a case series of ocular adnexal lymphoproliferative disorders. Int J Rheumatol. 2012;2012:635473. doi: 10.1155/2012/635473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ramirez L, D'Auria A, Popalzai A, Sanossian N. Bilateral vision loss secondary to pachymeningitis in a patient with IgG4-related disease. Front Neurol. 2014;5:192. doi: 10.3389/fneur.2014.00192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sogabe Y, Ohshima K, Azumi A, Takahira M, Kase S, Tsuji H, Yoshikawa H, Nakamura T. Location and frequency of lesions in patients with IgG4-related ophthalmic diseases. Graefes Arch Clin Exp Ophthalmol. 2014;252:531–538. doi: 10.1007/s00417-013-2548-4. [DOI] [PubMed] [Google Scholar]
- 14.Kitagawa S, Zen Y, Harada K, Sasaki M, Sato Y, Minato H, Watanabe K, Kurumaya H, Katayanagi K, Masuda S, et al. Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Küttner's tumor) Am J Surg Pathol. 2005;29:783–791. doi: 10.1097/01.pas.0000164031.59940.fc. [DOI] [PubMed] [Google Scholar]
- 15.Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, Klöppel G, Heathcote JG, Khosroshahi A, Ferry JA, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25:1181–1192. doi: 10.1038/modpathol.2012.72. [DOI] [PubMed] [Google Scholar]
- 16.Hagiya C, Tsuboi H, Yokosawa M, Hagiwara S, Hirota T, Takai C, Asashima H, Miki H, Umeda N, Horikoshi M, et al. Clinicopathological features of IgG4-related disease complicated with orbital involvement. Mod Rheumatol. 2014;24:471–476. doi: 10.3109/14397595.2013.844307. [DOI] [PubMed] [Google Scholar]
- 17.Wallace ZS, Deshpande V, Stone JH. Ophthalmic manifestations of IgG4-related disease: Single-center experience and literature review. Semin Arthritis Rheum. 2014;43:806–817. doi: 10.1016/j.semarthrit.2013.11.008. [DOI] [PubMed] [Google Scholar]
- 18.Kashii S. IgG4-related disease: A neuro-ophthalmological perspective. J Neuroophthalmol. 2014;34:400–407. doi: 10.1097/WNO.0000000000000193. [DOI] [PubMed] [Google Scholar]
- 19.Masaki Y, Dong L, Kurose N, Kitagawa K, Morikawa Y, Yamamoto M, Takahashi H, Shinomura Y, Imai K, Saeki T, et al. Proposal for a new clinical entity, IgG4-positive multiorgan lymphoproliferative syndrome: Analysis of 64 cases of IgG4-related disorders. Ann Rheum Dis. 2009;68:1310–1315. doi: 10.1136/ard.2008.089169. [DOI] [PubMed] [Google Scholar]