

Abstract
Aims and Objectives:
This clinical study was conducted to compare the interactive self-ligating twin brackets and the standard double width brackets for their efficiency in Rate of Retraction.
Materials and Methods:
A total of 20 patients with Angle's class I or class II or class III dento-alveolar malocclusions between the age group of 18-25 years were selected. 10 patients in each group both males and females were randomly selected for the study. Ten patients were bonded using conventional brackets (Group I) the other ten patients were bonded using Interactive self-ligating brackets (Group II). The Rate of retraction was quantified using the scanned models. Pretreatment and post treatment models were taken and scanned to measure the amount of Incisor movement and Anchor loss.
Results:
(1) Interactive Self-ligating brackets showed significant Rate of retraction when compared with conventional brackets on right and left quadrant. (Group I 0.545 ± .205: Group II 0.827 ± .208 P = .013*) (Group I 0.598 ± .160: Group II 0.804 ± .268 P = .071) (2) Interactive self-ligating brackets when compared with conventional brackets had significant amount of incisor movement on right and left quadrant. (Group I 3.51 ± .548: Group II 4.38 ± .1.06 P = .047*) and (Group I 3.66 ± .899: Group II 4.67 ± 1.02 P = .047*) (3) Conventional brackets showed significant Amount of Anchor loss when compared with that of Interactive self-ligating brackets on right and left quadrant. (Group I .948 ± .392: Group II 0.501 ± .229 P = .013*). In the left side (Group I 0.861 ± .464: Group II 0.498 ± .227 P = .060).
Conclusion:
The interactive self-ligating brackets show more efficiency in Rate of Retraction, Amount of Incisor movement and Amount of Anchor loss when compared with the conventional brackets.
Keywords: Interactive brackets, self-ligating, sliding mechanics
Introduction
Anchorage requirements form a critical component of en masse retraction. The retraction of four incisors following canine retraction is accepted as a method to minimize the mesial movement of the posterior teeth, whereas en masse retraction of six anterior teeth may create anchorage problems.[1]
The conventional approach involved placing the rigid wires into brackets and ligating it using ligature wires or elastomeric ties during retraction phase. Many studies that had been carried out describing the various types of ligation and their role in friction had proved that the elastomeric ligation method produced more friction when compared to that of stainless steel (SS) ligation.[2,3]
Years of constant trial and clinical experimentation had led the orthodontic professionals to realize that the probable answer to efficient en masse retraction lies in an optimal bracket system (CB), one that could do away with the need to utilize conventional ligating methods. This view point laid the foundation for the emergence of self-ligating CB.
A resurgence in the popularity of self-ligation occurred in the 1990s, reflecting further refinement, with many self-ligating systems having since been patented. Active self-ligating appliances may allow better torque control with undersize arch wires than can be achieved with passive appliances; storage of potential energy in a spring clip may also enhance the potential for labiolingual alignment. The resistance to sliding is thought to be lower for passive appliances, however, which may improve the aligning capability of these systems.[4]
A newer advanced version, the interactive self-ligating brackets (SLBs) by American Orthodontics (AO), featured a familiar twin bracket in a low profile design, facilitating an easy transition to self-ligation. It had unique features that were unavailable with other brackets or system. Most importantly, it was very special due to its versatility. The interactive self-ligating system offered the benefits of less friction at the initial stages of treatment and more control in the later stages to assist with final torque and rotation. This advantage was unavailable with other SLBs, and often can be utilized to the benefit of the clinicians.[5]
Thus, a clinical study was conducted to compare the clinical efficiency of the interactive brackets in the rate of space closure with that of the standard conventional brackets (CBs). Assessment of molar anchor loss and the movement of permanent incisors when using interactive systems and CBs constituted the second part of the clinical study. The null hypotheses of the study state that there is a significant difference regarding the clinical efficiency between conventional and interactive SLBs.
Materials and Methods
It was conducted on patients who reported to the Department of Orthodontics who were willing to undergo orthodontic treatment. Ethical approval for the study was obtained from the concerned University Scientific Committee. The study sample size comprised twenty patients.
Only adolescent and young patients between the age group of 18 and 25 years were selected for this study as the alveolar bone become denser with age and this could alter the rate of tooth movement. Sample size was determined using n-master software (version 1.0 CMC, Vellore, India) with the power of 80% and α error as 5% by which the sample size as 10 per group was derived.
All the patients were treated under the same protocol adopted by the institution with the following wire sequence, nickel titanium 0.016 inch, 0.016 × 0.022 inch, 0.017 × 0.025 inch, 0.019× 0.025 inch, and SS 0.019 × 0.025 inch in brackets with 0.022 × 0.028 inch slot.
The first group of CB system consisted of ten patients treated with conventional double width brackets (AO Master Series) tightly ligated with SS 0.009-inch ligatures. The second group of SLBs system consisted of ten patients treated with SLBs (AO Empower Interactive) of 0.022” slot with MBT prescription. To avoid any problem of standardization, the MBT prescription was selected in both the bracket system types. En masse space closure was done using an elastomeric module with SS 0.025-inch ligature wire tied from the first molar hook to the anterior soldered hook placed between the canine and lateral incisor in both the SLB and CB groups. Elastomeric modules were stretched twice the size (2–3 mm) for delivering 250 g of force for retraction, measured using dontrix gauge. The activations were done on a monthly appointment basis.[6,7]
Patient's case notes were utilized to extract demographic information, treatment duration, appointments, and clinical information for inclusion and exclusion criteria. Pre- and post-treatment dental casts were assessed for treatment outcome variables.
The requirements for inclusion in this study were patients needing extraction of four first premolars, without transverse discrepancies, use of conventional first molar anchorage, and no previous history of orthodontic or orthognathic surgery.
Cases excluded were based on the lack of data required for our research and use of additional anchorage reinforcement (mini-implant, head gear, trans-palatal arch, lingual arch, intermaxillary elastics, pendulum, twin block, and Nance and any removable appliances during active treatment).
Two implants were placed distal to the first permanent molars palatally using intraoral periapical X-ray as a guide, on either side of the arch before placing the posted arch wire. Implants with a diameter of 1.3 mm and a length of 8 mm were positioned between the roots of the first molar and the second molar from the palatal aspect in the upper arch. It was placed before upgrading to 0.019 × 0.025 SS posted arch wire. These implants were used as stable markers during the study. According to a study by Liou et al.,[8] microimplants do not remain stationary when orthodontically loaded, it moves in some patients depending on the loading characteristics. Hence, these implants were not loaded during the study. Impressions were made with the implants in place and models were poured. Preretraction records consisting of models and photos were taken [Figure 1]. Implant was used as a stable reference point in the model.
Figure 1.

Pre- and post-retraction intraoral images
Initially, during the first 5 months of retraction phase, the implants were not loaded to assess the efficacy of the bracket system, later engaged to the palatal attachment on the molars to gain the lost anchor and reinforce the anchorage to close the residual spaces. Records for the study consisting of models and photos were taken after 5 months of retraction.
Evaluation of the scanned models
Following markings were done in the models [Figure 2]:
Figure 2.
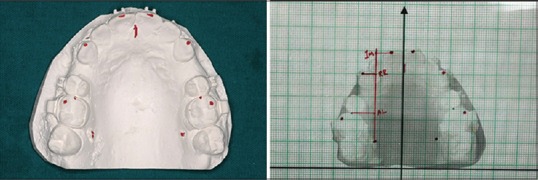
Markings on the model before scanning and scanned model superimposed on the graphical template with the points (IM, RR, and AL)
Tip of the maxillary central incisors right and left
Tip of the maxillary canine right and left
Mesial marginal ridge of the maxillary first molar right and left
Palatal implant right and left
Mid palatal line along the suture.
Models were scanned by placing the occlusal surface of the cast on the scanning panel of the device so that there was a three-point occlusal contact on the surface. By this method, the occlusal plane was standardized in such a way that it was parallel to the floor.[9]
All the casts were scanned along with a ruler so that the scanned images obtained were in 1:1 ratio [10] [Figure 3]. Measurements were recorded from the scanned images to avoid parallax error. A graphical template (symmetric grid) was made and the scanned image was superimposed on to the graphical template.[11] All the above standardizations were done using Corel Draw X6 soft ware (Ottawa, Canada).
Figure 3.

Scanned image of the models at 1:1 ratio
The vertical line, namely the mid-sagittal plane was drawn, and a parallel line was generated through the implant which was used as the vertical reference on which the horizontal lines perpendicular were projected that form the markings on the graphical template (symmetric grid) so that the point of intersection between the two lines was obtained. Then, the linear distance from the intersection point to the palatal micro-implant was measured in all the scanned images of the pre- and post-treatment dental models. The following parameters were measured; rate of retraction, amount of anchor loss, and amount of incisor movement.
All the measurements were scored in millimeter (mm). Mitutoyo digital vernier caliper measuring to 0.01 mm was used for measuring all the measurements,[10] as all the measurements represented the linear distance between each point. That is, RR point (horizontal line passing through the cuspal tip of the canine and the vertical line passing through the microimplant) [Figure 4]:
Figure 4.
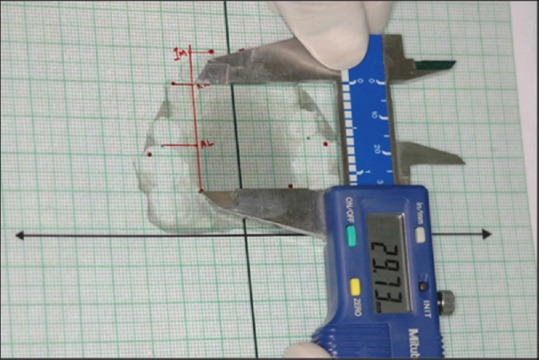
Measuring the amount of retraction from the implant to the tip of the canine (RR point)
AL point (horizontal line passing through the mesial marginal ridge of the first molar and the vertical line passing through the microimplant) [Figure 5] and
IM point (horizontal line passing through the incisal tip of the central incisors and the vertical line passing through the microimplant) [Figure 6].
Figure 5.
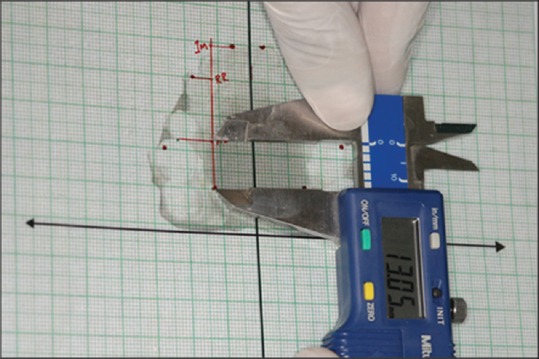
Measuring the amount of anchor loss from the implant to the mesial marginal ridge of the maxillary first molar (AL point)
Figure 6.
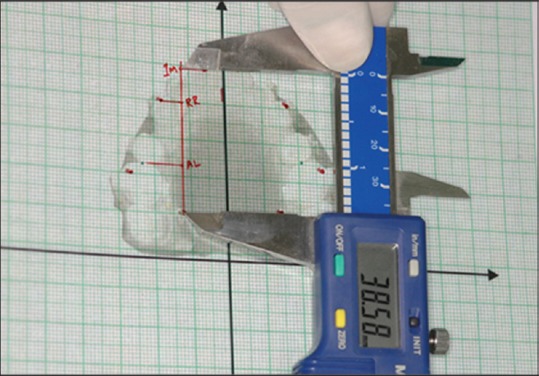
Measuring the amount of the incisor movement from the implant to the central incisor tip (IM point)
All the measurements were obtained directly from the scanned images of the maxillary model, which was calibrated in 1:1 ratio rather than intraorally. Proper positioning of the caliper was possible when using the graphical template which was essential for consistent accuracy. The collected data were statistically analyzed by independent t-test and NPar tests (Mann–Whitney U-test).
Results
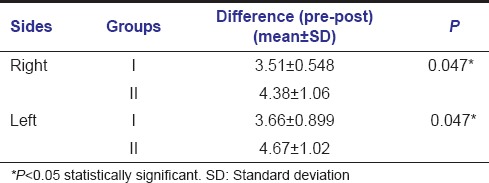
The results are summarized in Tables 1–3. The amount of retraction between Group I and Group II in the right side was Group I: 0.545 ± 0.205 and Group II: 0.827 ± 0.208; P = 0.013. In the left side, Group I was 0.598 ± 0.160 and Group II was 0.804 ± 0.268; P = 0.071 [Table 1]. The amount of incisor movement between Group I and Group II in the right and left side was Group I: 3.51 ± 0.548 and Group II: 4.38 ± 0.1.06; P = 0.047 and Group I: 3.66 ± 0.899 and Group II: 4.67 ± 1.02; P = 0.047 [Table 2]. The amount of anchor loss between Group I and Group II in the right side was Group I: 0.948 ± 0.392 and Group II: 0.501 ± 0.229; P = 0.013. In the left side, Group I was 0.861 ± 0.464 and Group II was 0.498 ± 0.227; P = 0.060 [Table 3].
Table 1.
Comparison of rate of retraction on the right and left side between Groups I and II
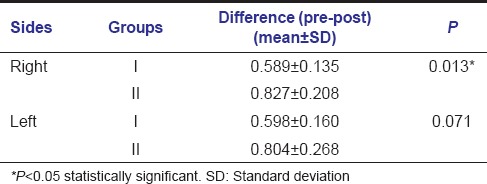
Table 3.
Comparison of amount of anchor loss on the right and left side between Groups I and II
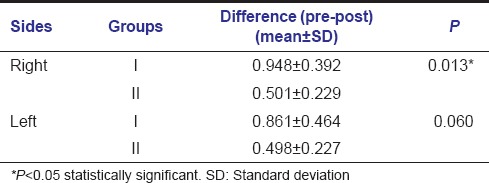
Table 2.
Comparison of amount of incisor movement on the right and left side between Groups I and II
Discussion
There was a significant difference in the right side between the two groups when rate of retraction was assessed at the end of 5 months. The data represented in CBs were comparatively lesser than that of SLBs which indicated that there was more amount of retraction in the right side in SLBs when compared with that of conventional system. Krishnan et al.[12] in their study stated that retraction is more on the left side of the patient when compared to that of the right side owing to the habitual mastication. The study by Singh and Shetty (1999)[13] also reinforced the concept of more movement of teeth on the side where the masticatory function was more. This could be attributed to the fact that the right-handed persons chew more on the right side [14] leading to trampoline effect.[15]
There was no significant difference in the left side between the two groups. According to Fleming and O'Brien (2013),[16] there was a slight benefit with respect to the rate of space closure using SLB system when compared with the CB system which concurred with this study, i.e., rate of space closure was slightly faster in SLB system when compared with CB system.
In comparison of incisor movement at the end of 5 months between CB and SLB, there was a significant difference observed between the two groups. This indicated that there was a difference in the efficiency of incisor movement in SLB, i.e., interactive brackets. According to Chen et al.,[10] there was a good torque control and more bodily movement of incisors commencing from alignment to the retraction phase while using self-ligating system.
In comparison to the amount of anchor loss (mean indices and standard deviation) at the end of 5 months between CB and SLB, there was a significant difference in the right side between the two groups. The data indicated that there was more amount of anchor loss in the right side in CB than in the SLB. There was no significant difference in the left side between the two groups. There were many studies which stated that there was no significant difference of anchor loss between self-ligating and CB system, which was not concordant to this study.[17,18,19]
According to Muguruma et al.,[20] SLBs produced less static friction when compared with CBs, which might lead to better anchorage control in SLB system, and Chen et al.[10] stated that there was better anchorage control in interactive SLB system when compared with CB system, which concurred with the study, i.e., anchor loss was less in interactive SLB system when compared with CB system. The null hypothesis had been proved as stated.
Conclusion
The following observations were drawn from the study:
Interactive SLBs showed a significant rate of retraction when compared with CBs
Interactive SLBs when compared with CBs had a significant amount of incisor movement
CBs showed a significant amount of anchor loss when compared with that of interactive SLBs.
The interactive SLBs show more efficiency in the rate of retraction, amount of incisor movement, and amount of anchor loss, when compared with the CBs. Further, comparative clinical studies using three-dimensional models are need to be performed on these interactive SLBs with an increase in the sample size and also the number of parameters to prove its total clinical efficiency.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Park HS, Kwon TG. Sliding mechanics with microscrew implant anchorage. Angle Orthod. 2004;74:703–10. doi: 10.1043/0003-3219(2004)074<0703:SMWMIA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Edwards GD, Davies EH, Jones SP. The ex vivo effect of ligation technique on the static frictional resistance of stainless steel brackets and archwires. Br J Orthod. 1995;22:145–53. doi: 10.1179/bjo.22.2.145. [DOI] [PubMed] [Google Scholar]
- 3.Khambay B, Millett D, McHugh S. Evaluation of methods of archwire ligation on frictional resistance. Eur J Orthod. 2004;26:327–32. doi: 10.1093/ejo/26.3.327. [DOI] [PubMed] [Google Scholar]
- 4.Fleming PS, DiBiase AT, Lee RT. Self-ligating appliances: Evolution or revolution? Aust Orthod J. 2008;24:41–9. [PubMed] [Google Scholar]
- 5.Valant JR. Time: A self-ligating interactive bracket system. Semin Orthod. 2008;14:46–53. [Google Scholar]
- 6.Bennett JC, McLaughlin RP. Controlled space closure with a preadjusted appliance system. J Clin Orthod. 1990;24:251–60. [PubMed] [Google Scholar]
- 7.Johansson K, Lundström F. Orthodontic treatment efficiency with self-ligating and conventional edgewise twin brackets: A prospective randomized clinical trial. Angle Orthod. 2012;82:929–34. doi: 10.2319/101911-653.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Liou EJ, Pai BC, Lin JC. Do miniscrews remain stationary under orthodontic forces? Am J Orthod Dentofacial Orthop. 2004;126:42–7. doi: 10.1016/j.ajodo.2003.06.018. [DOI] [PubMed] [Google Scholar]
- 9.Dungarwal N, Rahalkar JS, Deshmukh S, Prakash A, Dhoka N, Shyagali TR. Evaluation of maxillary interpremolar, molar width by DRNA indices and arch dimension, arch form in Maratha population. J Indian Orthod Soc. 2013;47:461–7. [Google Scholar]
- 10.Chen XH, Hua YM, Xie XQ, Yu XJ, Wang J, Liu LM. Clinical study of extraction treatment of class II division I malocclusion with empower self-ligating brackets. Shanghai Kou Qiang Yi Xue. 2013;22:316–21. [PubMed] [Google Scholar]
- 11.Ferrari S, Bellincampi M, Sfondrini MF, Caprioglio A, Gandini P. Finishing effectiveness of different archwires using SmartClip™ self-ligating brackets: A clinical study. Int Orthod. 2014;12:125–38. doi: 10.1016/j.ortho.2013.12.001. [DOI] [PubMed] [Google Scholar]
- 12.Krishnan P, Shetty S, Husain A. An adjunctive minor surgical procedure for increased rate of retraction. J Pharm Bioallied Sci. 2013;5(Suppl 1):S39–42. doi: 10.4103/0975-7406.113293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Singh G, Shetty VS. Extraction space closure in the stage II of Begg technique. J Indian Orthod Soc. 1999;32:58–64. [Google Scholar]
- 14.Nissan J, Gross MD, Shifman A, Tzadok L, Assif D. Chewing side preference as a type of hemispheric laterality. J Oral Rehabil. 2004;31:412–6. doi: 10.1111/j.1365-2842.2004.01256.x. [DOI] [PubMed] [Google Scholar]
- 15.Bennett JC, Mclaughlin RP. Orthodontic Treatment Mechanics and the Preadjusted Appliance. London: Mosby Wolfe Publication; 1993. [Google Scholar]
- 16.Fleming PS, O'Brien K. Self-ligating brackets do not increase treatment efficiency. Am J Orthod Dentofacial Orthop. 2013;143:11–9. doi: 10.1016/j.ajodo.2012.10.012. [DOI] [PubMed] [Google Scholar]
- 17.Miles PG. Self-ligating vs conventional twin brackets during en-masse space closure with sliding mechanics. Am J Orthod Dentofacial Orthop. 2007;132:223–5. doi: 10.1016/j.ajodo.2007.04.028. [DOI] [PubMed] [Google Scholar]
- 18.Chen SS, Greenlee GM, Kim JE, Smith CL, Huang GJ. Systematic review of self-ligating brackets. Am J Orthod Dentofacial Orthop 2010;137:726. 2010;137:726.e1–18. doi: 10.1016/j.ajodo.2009.11.009. [DOI] [PubMed] [Google Scholar]
- 19.Mezomo M, Lima ES, Menezes LM, Weissheimer A, Allgayer S. Maxillary canine retraction with self-ligating and conventional brackets: A randomized clinical trial. Angle Orthod. 2011;81:292–7. doi: 10.2319/062510-348.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Muguruma T, Iijima M, Brantley WA, Ahluwalia KS, Kohda N, Mizoguchi I. Effects of third-order torque on frictional force of self-ligating brackets. Angle Orthod. 2014;84:1054–61. doi: 10.2319/111913-845.1. [DOI] [PMC free article] [PubMed] [Google Scholar]