

Abstract
Background
Millions of villagers in Bangladesh remain exposed to high levels of arsenic (As) from drinking untreated well-water even though the scale of the problem was recognized 15 years ago. Water treatment at the household-level has been promoted as a viable complement but few longitudinal studies of their efficacy using an objective measure of exposure have been conducted. Participants (N=622) of a nutrition trial in Araihazar, Bangladesh were each provided with READ-F filters at the beginning of the study and encouraged to use them over the 6 month duration of the intervention. Well-water As, treated water As, and urinary As were monitored periodically during the trial and measured again one year after the trial ended.
Results
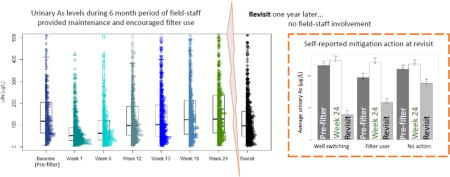
The READ-F filters were initially well received and median urinary As levels for participants declined from 117 μg/L to 51 μg/L within a single week. However, median urinary As levels gradually rose back to 126 μg/L by the end of the trial. Fifty filters were replaced over the course of the trial because of insufficient As removal or reduced flow. With these exceptions, most of the treated water met the WHO guideline for As in drinking water of 10 μg/L. One year after the nutritional trial ended, 95% of participants had abandoned their filter citing inconvenience as the primary reason. At that time, median urinary As levels for 10 participants who had switched to a nearby low-As well had declined to 63 μg/L.
Conclusions
Participants were probably no longer using the READ-F filter long before the 6 month nutritional intervention ended despite claiming that they were using them. Household-level treatment is likely to continue to play a minor role in the effort to reduce As exposure in Bangladesh. Understanding the limitations of such expensive interventions is important for future policy regarding As mitigation.
Keywords: Arsenic, groundwater, treatment, biomarker, longitudinal study, water filters
Graphical abstract
1. Introduction
Identifying sustainable ways of reducing exposure to arsenic (As) naturally contained in groundwater is a major public health challenge given the wide range of diseases it can cause (Straif, Benbrahim-Tallaa et al. 2009, Danielle J. Carlin, Heacock et al. 2015). Bangladesh is particularly affected, with the most recent national survey conducted in 2013 showing about 20 million villagers still routinely drink and cook with water containing >50 μg/L As, the national standard, and 40 million people consume water that does not meet the WHO guideline of 10 μg/L (BBS/UNICEF 2015). Well testing and, as a result, households switching to a nearby private low-As well or a deep low-As community well have by far had the largest impact on exposure reduction to date in Bangladesh (Ahmed, Ahuja et al. 2006, Chen, van Geen et al. 2007, Johnston, Hug et al. 2014). But with probably less than half of the originally exposed population of Bangladesh currently served by these relatively simple forms of mitigation, there is still considerable interest in the many different ways As can be removed from drinking water (Singh, Singh et al. 2015).
In 2009, the Bangladesh Council of Scientific and Industrial Research provisionally approved six arsenic-mitigation technologies for public use (Johnston, Hanchett et al. 2010). Testing was conducted in a laboratory setting using artificial groundwater to verify the claims set by each company against various hydrogeological conditions found in Bangladesh (Johnston, Hanchett et al. 2010, Ahmed and Ahmed 2014). A considerable number of more realistic field studies have been conducted in Bangladesh to demonstrate that these, or similar systems, remove As from actual groundwater for at least some time (Cheng, van Geen et al. 2004, Hussam and Munir 2007, Jones-Hughes, Peters et al. 2013, Neumann, Kaegi et al. 2013). To our knowledge, however, only one such study paired the deployment of an As-removal system with the systematic monitoring of a biomarker to evaluate its effectiveness directly, instead of relying on the As content of the water and claims by the household that the system was systematically used (Milton, Smith et al. 2007). Although several lab-approved arsenic removal water filters exist, there is a paucity of research on their prolonged use in the field.
Faced with the challenge of reducing As exposure in a micronutrient supplementation trial intended to lower blood As concentrations (Peters, Hall et al. 2015), several hundred households in Araihazar, Bangladesh, were provided with one of the approved As-removal systems and encouraged to use them for 6 months. This intervention provided a unique opportunity to monitor the effectiveness of such a system because both untreated and treated water As, as well as urinary As, were monitored over the duration of the intervention and, for a subset of participants, measured again 12 months later.
2. Methods
2.1 The Folate and Creatine Trial (FACT)
The setting for the deployment of household filters was provided by FACT, a double-blind, placebo-controlled, randomized trial conducted in Araihazar, Bangladesh. Details on the study have been described elsewhere (Peters, Hall et al. 2015). Briefly, FACT examined how folate and creatine supplementation influence blood As levels over six-months. Between December 2009 and May 2011, the study recruited 622 otherwise healthy adults. For inclusion criteria, The FACT study recruited members of the Health Effects of Arsenic Longitudinal Study (HEALS) cohort (Ahsan, Chen et al. 2006) who had been consuming water As (wAs) >50 μg/L, exceeding the Bangladeshi standard for As, for at least one year before the study began. The study excluded pregnant women, individuals taking nutritional supplements, individuals with protein in their urine, and individuals with known renal disease, diabetes, or gastrointestinal or other health problems. Ethical approval was obtained from the Institutional Review Board of Columbia Presbyterian Medical Center and the Bangladesh Medical Research Council. Informed consent was obtained from all participants.
All FACT participants (both those who received nutritional supplementation and those in the control group) received a free READ-F (Brota International, Inc.) point-of-use arsenic-removal unit when the trial began (Figure 1). The filter was selected over two other household-level filters based on our analysis of treated water from systems deployed by UNICEF in Shahrasti upazila in 2007. The READ-F units are also portable and easy to use. Field staff showed participants how the filter worked, by simply pouring untreated well water in the top of the filter tank and collecting treated water from the tap (figure 1a), and instructed participants to use filter-treated water for all cooking and drinking throughout the duration of the six-month trial.
Figure 1. Filter deployment area.
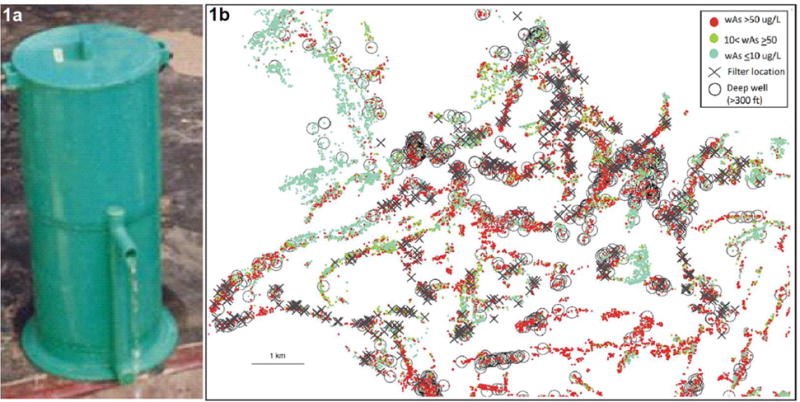
1a. The READ-F arsenic removal unit. Photo from: http://www.dphe.gov.bd/index.php%3Foption%3Dcom_content%26view%3Darticle%26id%3D96%26Itemid%3D104 1b. Map of Araihazar, Bangladesh. Colored dots show tubewells tracked and tested by Columbia University using the ITS Econo-Quick kit (van Geen et al., 2014). The color indicates the well’s water As level. The diagonal crosses show where the filters were deployed. The larger circles show the location of low-As deep wells to which participants could switch. In most cases deep wells are community wells.
Field staff worked in pairs, one interviewer and one physician, to recruit and follow study participants through face-to-face home visits at week 0 (baseline), 1, 6, 12, 13, 18, and 24. Urine samples were collected at each of these visits. Field staff verified the filter was adequately lowering As throughout the six-month intervention by testing filter-treated wAs levels using the Hach EZ kit at each home visit. If measurement indicated filter failure (wAs>10), or if participants cited filter failure, filters were repaired or replaced by the field staff. After the six-month nutritional intervention ended, participants were allowed to keep the filter, however, maintenance was no longer provided by field staff.
Beginning in December 2012, during routine HEALS cohort follow-up home visits, field staff returned to FACT participants and collected new water and urine samples. During this interval, the filters were no longer monitored and participants were not reminded to use the filter. Using a structured questionnaire, field staff asked participants about their experience with the filter and other mitigation options.
2.2 Arsenic levels in well-water (untreated)
Each tubewell used by a member of the HEALS cohort since 2000 is marked with a small numbered ID tag and a placard indicating its status with respect to As. The placard is often removed or lost over time but the small ID tag typically remains. The corresponding wAs level for each tubewell ID is tracked through a database. Figure 1b shows the spatial distribution of all tubewells and their corresponding As levels tested and tracked through the database. At enrollment, participants’ wAs level was identified through their reported tubewell ID and was used to enroll participants on the basis of their As content. For any participants indicating that they used an untested tubewell, the new well was tested in the field using the Hach EZ kit (Hach Company, Loveland, CO). The inclusion criterion was met if the test result indicated a water As concentration >50 μg/L. The Bangladesh Arsenic Mitigation and Water Supply Project has used the Hach EZ kit to test millions of wells. Prior studies evaluating the accuracy of this kit found it to be fairly accurate, correctly identifying the status of tested wells 88% of the time, provided the reaction time is increased from 20 to 40 min (van Geen, Cheng et al. 2005).
All well-water samples at the time of recruitment were collected and sent to Lamont-Doherty Earth Observatory (LDEO) of Columbia University in New York for confirmatory analysis. Water As levels were measured using a previously published method (Cheng, Zheng et al. 2004, van Geen, Cheng et al.). The detection limit of this method is on the order of 0.1 μg/L and the precision ~5%. Of the 622 participants enrolled in the study, 435 participants were recruited from wells with known wAs concentrations and 187 participants were recruited from wells with a previously unknown wAs concentration.
2.3 Arsenic levels in filter-treated water
Throughout the trial arsenic levels in filter-treated water was tested at week 1, 6, 12, 13, 18, and 24 using the Hach EZ kit and a 40 min reaction time. In addition, we collected a random subset of filtered water samples at baseline, week 12, and week 24 for confirmatory laboratory analysis.
2.4 Arsenic removal technology (READ-F)
The READ-F point-of-use arsenic-removal unit is locally manufactured and distributed by Brota Services International, Bangladesh. One unit costs approximately $70; however, study participants did not have to pay for their filter. At each visit, field staff measured filter-treated wAs levels. If measurement indicated filter failure, or if participants cited filter failure, filters were repaired or replaced free-of-charge by Brota International. READ-F filters use resin-embedded hydrous cerium oxide as the adsorptive agent. Under the Bangladesh testing program, READ-F filters were shown to be effective for at least two years when raw water contained dissolved iron levels <10 mg/L, phosphate concentrations <4 mg/L, and pH <7.5.
2.5 Total urinary arsenic
Eight spot urine samples were collected from each participant over time, seven times over the course of the nutritional trial and once more a year after the trial ended. Urinary As metabolites were speciated using HPLC separation of arsenobetaine, arsenocholine, AsIII, AsV, MMAIII+V and DMAIII+V followed by detection using ICP-MS-DRC1(Reuter, Davidowski et al. 2003). Total urinary As is calculated as the sum of AsIII, AsV, MMAIII+V and DMAIII+V..
2.6 Statistical analyses
We calculated summary statistics to describe characteristics of the sampled population. Urinary As variables were natural-log transformed to meet normality assumptions. We substituted samples with levels below the detection limit with the detection limit value (0.1 μg/L). We used paired t-tests to examine the mean difference at each time point and determined the percent change in mean uAs over time compared to baseline using the formula. We used one-way repeated measures ANOVA to examine both between- and within- subject effects and Kurskal-Wallis when data did not meet assumptions. All statistical tests were two-sided with a significance level of 0.05. All analyses were conducted in SAS (version 9.4, Cary, NC).
3. Results
Of the 622 participants enrolled in FACT, 595 were surveyed at a HEALS cohort follow-up visit one year later, yielding a 96% revisit response rate. Of the 27 participants who were lost, 6 refused, 2 were not available for interview, 6 moved, and 3 died. Half of the participants were male. The age of participants ranged from 24–55 years old and BMI ranged from 13.8–31.9 kg/m2. Just over a quarter of the participants reported a history of smoking and almost half of the population owned land (a sociodemographic proxy variable) (Table 1).
Table 1.
Study population characteristics
| Variable | Mean ±SD or n (%) | Min | Max |
|---|---|---|---|
| Water As (μg/L) | 130 ±119 | 0.10 | 1182 |
| Male | 311 (50%) | ||
| Age (years) | 38 ±8 | 24 | 55 |
| BMI (kg/m2) | 19.9 ±3 | 13.8 | 31.9 |
| Education (years) | 3.5 ±3 | 0 | 16 |
| Ever smoker | 168 (27%) | ||
| Ever betel nut user | 152 (24%) | ||
| Own land | 292 (47%) | ||
| Own TV | 276 (44%) |
3.1 Well-water and urinary arsenic at baseline
At baseline, the median untreated well-water As level was 103 μg/L and ranged from <1 to 1182 μg/L. Fifty-four out of 622 participants turned out to be using a well with water As levels <50 μg/L, mostly because of discrepancies between the field kit and laboratory measurements near the threshold. Results were similar regardless of excluding participants with low well-water As levels, and thus all participants were included. Figure 2 illustrates the relationship between untreated water As levels and urinary As concentrations at baseline. There was considerable scatter between untreated water As levels and urinary As levels at baseline (Figure 2a), but levels were also positively correlated (Spearman correlation=0.41, p<0.0001). There was also a wider range in urinary As level with increasing water As levels (Figure 2b).
Figure 2. Relationship between well-water and urinary arsenic levels at baseline.
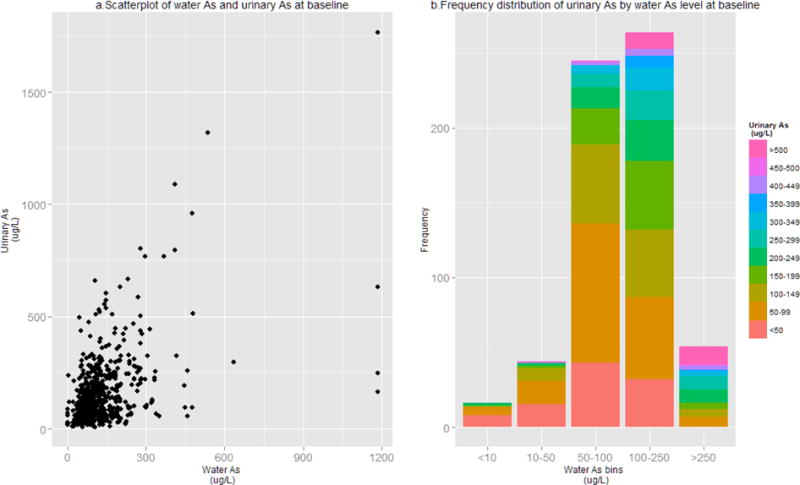
2a. Scatterplot of untreated well-water and urinary As levels at baseline (n=622). 2b. Frequency distribution of urinary As level at baseline categorized by corresponding untreated well-water level.
3.2 Arsenic removal from well-water
Initially, all READ-F systems effectively removed As from drinking water at levels below the WHO guideline of 10 μg/L. About 50 filters reportedly did not function during the trial, either because of clogging or because As in the treated water was too high and were replaced by Brota International. Arsenic levels in treated water were field tested using the HACH EZ kit throughout the trial. In addition, filter treated water samples were repeatedly collected from the final 215 participants’ filter systems at baseline, week 12 and week 24 for laboratory analysis. Out of this confirmatory subset, As levels in treated water analyzed in the laboratory were mostly below 10 μg/L during the six-month nutritional trial (Table 2). Among the 31 systems tested 12 months after the nutritional intervention ended, 5 filters failed to reduce wAs<10 μg/L and As levels in treated water were above 50 μg/L in two of these filters (Figure 3).
Table 2.
Summary statistics for arsenic levels (μg/L) in filtered water analyzed in the laboratory
| Filter-treated wAs |
n | Mean ± SD | Median | Min | Max | Number of failed filters (wAs>10μg/L) |
|---|---|---|---|---|---|---|
| Baseline | 215 | 0.4 ±0.7 | 0.1 | <0.07 | 4.6 | 0 |
| Week 12 | 215 | 1.1 ±1.8 | 0.4 | <0.07 | 15.5 | 2 |
| Week 24 | 215 | 0.4 ±0.7 | 0.1 | <0.07 | 5.9 | 0 |
| Revisit | 31 | 9.8 ±25.2 | 0.9 | <0.07 | 112.4 | 5 |
Figure 3. Filter-treated water arsenic levels over time.
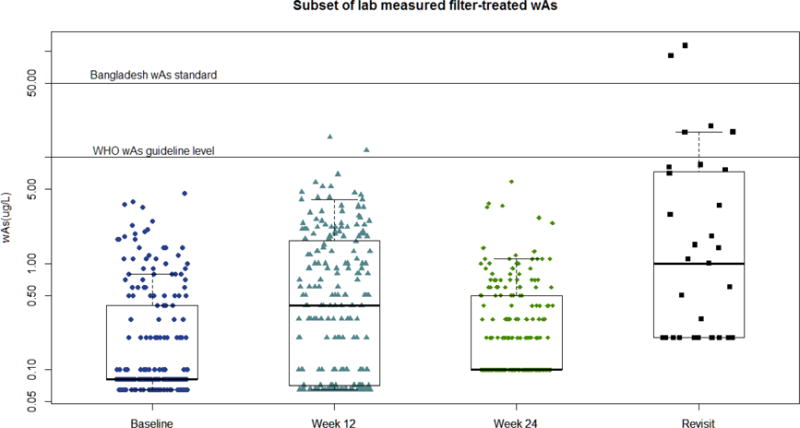
Subset of filter-treated water As levels measured by ICP-MS at baseline, week 12, 24 (n=215) and at a revisit one year after the nutritional trial ended (n=31). Horizontal line at 10 μg/L indicates the WHO guideline level for As. Horizontal line at 50 μg/L indicates Bangladesh’s national As standard.
3.3 Changes in exposure over the first 6 months
Filters were well received during the first weeks of the nutritional trial (Table 3). Median urinary As dropped from 117 μg/L at baseline to 51 μg/L in the first week, on average, a 54% decrease. Although urinary arsenic levels were similar at 1 and 6 weeks, levels were significantly higher at week 6 compared to week 1 (t(609)=4.04, p<0.0001). By week 18, As had increased to within 1% of baseline levels. The range of urinary As was still quite wide throughout the duration of the nutritional trial (Figure 4). Overall, urinary As levels at week 24 were not significantly different from urinary As levels at baseline (t(593)=1.14, p-value=0.2544).
Table 3.
Total urinary arsenic levels and the percent change in urinary arsenic from baseline.
| Time | n | Median | Min | Max | Percent change from baseline urinary As | p-value |
|---|---|---|---|---|---|---|
| Baseline | 622 | 117 | 7 | 1767 | ||
| Week 1 | 618 | 51 | 5 | 790 | −54% | <0.0001 |
| Week 6 | 612 | 62 | 4 | 801 | −46% | <0.0001 |
| Week 12 | 604 | 97 | 6 | 1591 | −15% | <0.0001 |
| Week 13 | 606 | 101 | 5 | 1233 | −14% | 0.0001 |
| Week 18 | 605 | 124 | 4 | 1867 | −1% | 0.6354 |
| Week 24 | 593 | 126 | 6 | 1607 | 5% | 0.2544 |
| Revisit | 595 | 97 | 5 | 1429 | −24% | <0.0001 |
uAs= μg/L, paired t-test versus uAs at baseline
Figure 4. Total urinary arsenic levels over time.
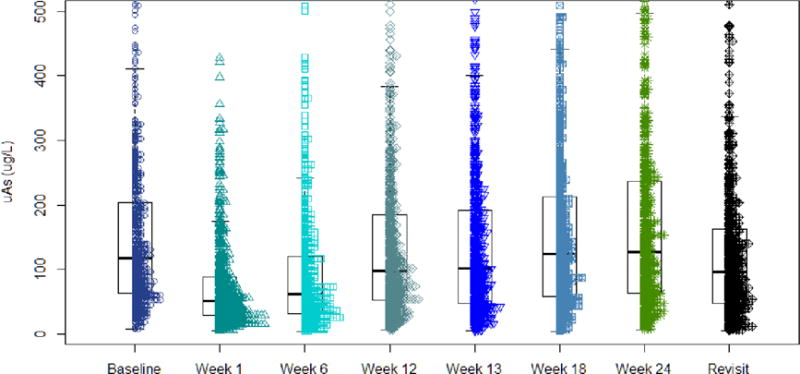
Distribution of total urinary As levels over the first six-months (n=622) and at a revisit one year later (n=595).
3.4 Filter use 12 months after the end of the trial
All participants were revisited by HEALS field staff one year after the nutritional trial ended. Only 31 of the original 622 filters were purportedly still in use. Inconvenience was the most commonly reported reason that participants stopped using their filter (n=378), with comments indicating that the flow-rate of treated water had slowed over time, likely because of insufficient maintenance of the media. Thus, as the flow-rate slowed, filters took more time and became increasingly inconvenient to use.
We compared the effect of post-trial filter use (“yes, always”, “yes, sometimes”, or “no, stopped using filter after trial”) on urinary As levels since the end of the nutritional trial (week 24). There was not a significant difference between filter use groups and uAs (F(2, 564),=0.73, p=0.4844).
Although the number of well-switchers and continued filter-users was small, we explored the potential long-term trends in uAs between those who either switched to a low-arsenic well (n=10) or continued to always use their filter (n=12,) and those who did not take any further exposure mitigation after the nutritional trial ended (n=556). For this analysis we excluded participants who reportedly only “sometimes” used their filters (n=12). Looking at the within-person time trends, all participants had significantly lower uAs levels at revisit than they had at both the beginning and end of the nutritional-trial (Table 4). Self-identified “always” filter-users had somewhat lower uAs levels compared to those who did not take a mitigation action, although this did not achieve statistical significance (Kurskal-Wallis chi-square=3.5644, p-value=0.0590).
Table 4.
Mitigation options and total urinary arsenic levels one year after nutritional trial ended. Mitigation action analysis excludes 17 participants only “sometimes” using their filter.
| Still using filter? | n | Revisit uAs Median (μg/L) | Revisit uAs Range (μg/L) | Revisit vs Baseline | Revisit vs Week 24 | ||
|---|---|---|---|---|---|---|---|
| Percent change in uAs | p-value | Percent change in uAs | p-value | ||||
| Yes, always | 12 | 65 | 19–302 | −40% | 0.0367 | −52% | 0.0092 |
| Yes, sometimes | 17 | 75 | 7–518 | −38% | 0.1181 | −14% | 0.6580 |
| No | 566 | 98 | 5–1429 | −28% | <.0001 | −27% | <.0001 |
| Mitigation action | |||||||
| Switched to low-As well | 10 | 63 | 6–87 | −66% | 0.0151 | −69% | 0.0057 |
| Always uses filter | 12 | 65 | 19–302 | −40% | 0.0367 | −52% | 0.0092 |
| No action | 556 | 102 | 5–1429 | −20% | <.0001 | −25% | <.0001 |
3.5 Well-switching from the end of the FACT trial to the re-visit one year later
Those who reported switching to a nearby low-arsenic well had significantly lower uAs levels compared to those who reported no longer using their filter after the trial ended (Kruskal-Wallis chi-square=6.7018, p-value=0.0096) (Figure 5). Mitigation action did not significantly differ by sex, land-ownership or age (all p-values>0.1).
Figure 5. Self-reported mitigation action one year after nutritional trial ended and corresponding urinary arsenic levels.
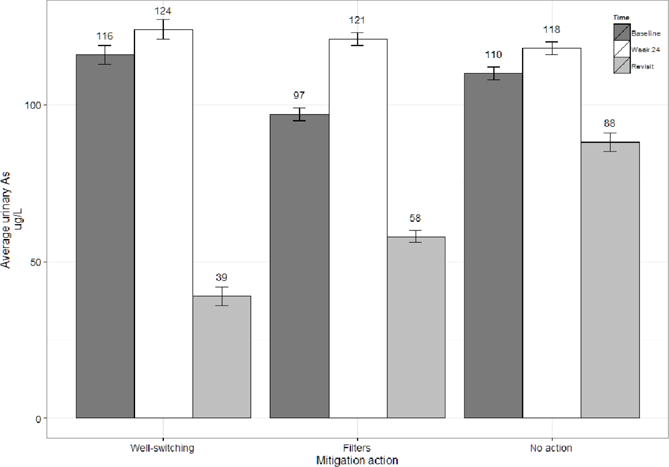
Average urinary As level above bars, week 24 indicates the end of nutritional trial.
4. Discussion
The READ-F filters were well received at the onset of the trial. The filters successfully removed As from contaminated water during the nutritional trial and, during the first few weeks, the uAs levels of study participants decreased. Some of the participants indicated that the filters improved the taste and clarity of the water and, when used for cooking, produced rice that remained whiter. These remarks are consistent with the positive evaluations of filters collected by Inauen et al. 2013, although the same study reports that as much of a third of households to whom filters were delivered subsequently denied that they had received a filter and were therefore not interviewed. As Inauen et al. 2013 point out, this may also have been an indication of lack of interest in household filters by a substantial fraction of the population.
The main reason for participants’ perception of improved quality of the treated water is likely due to iron removed by the filters. The high iron content of water in the region (up to 10 mg/L) (Zheng, Stute et al. 2004) and the generation of flocs upon oxidation may lead filters to clog and thus decrease the flow rate of treated water (Ahmed and Ahmed 2014). This may have been a major factor reducing the use of the filters, although other factors may have played a role as well since the uAs data indicate diminished use while maintenance was still provided under the trial.
Declining long-term filter use compliance rates have been previously reported in sand filter studies (Milton, Smith et al. 2007), where self-reported compliance dropped from 80% compliance in the first month to 20% compliance in the 12th month. In a randomized controlled trial of one of the early three-pitcher filter systems, Milton et al. 2007 report that, 12 months after their introduction, uAs concentrations among those who received filters were not significantly different from pre-intervention levels. Unfortunately, our experience with the READ-F filter was no better, even if the READ-F filter is more effective in terms of removing As and conceptually simpler to maintain. Although filter-treated wAs levels remained low throughout the duration of the nutritional trial, uAs rebounded by week 6; indicating fading use, not failing technology. Further qualitative study to understand other dimensions of human behavior related to filter compliance may be useful for future studies which consider the provision of filters.
We examined whether groundwater As levels were unstable over time and if this could influence the slow rise in urinary As levels. Among participants who continued to use their same well one year post-trial, untreated wAs remained within 10% of the baseline concentration for 157 of 188 participants, indicating As levels in groundwater were stable for the duration of the intervention.
A significant strength of this study compared to most technological demonstrations of As removal at the household-level is the direct measurement of urinary As over an extended period of time. One weakness of the study may be that the households were not sufficiently encouraged to perform the most basic maintenance, i.e. regularly washing the sand filter media to remove accumulated iron flocs, themselves (BETV-SAM/DPHE/ITN 2007)., this might have alleviated some of the diminished flow issues and could have prolonged use of the filters. Further, education and encouragement for using and maintaining units have previously been identified as some of the main driving factors behind villager participation and is not unique to this population (Jones-Hughes, Peters et al. 2013).
4.1 Implications for mitigation
Even though the filter selected for this trial was probably the most effective and easy to use on the market, it was soon rejected by the majority of households despite repeated encouragement to use them. In contrast, traditional forms of well-water treatment that do not require any specialized media, only sand and are based on aeration and iron precipitation, have been shown to be effective for reducing As exposure in other countries such as Vietnam (Berg, Luzi et al. 2006). Unfortunately, this approach will often fail in Bangladesh because levels of iron are too low and levels of phosphate are too high (Neumann, Kaegi et al. 2013). This failed attempt to reduce exposure by treatment at the household-level confirms that well-testing and exploiting the spatial variability of As levels in well-water thus redirecting households to a subset of safe wells, in parallel with more installation of deep community wells, are more promising avenues that need to be reinvigorated in Bangladesh (Ahmed, Ahuja et al. 2006, van Geen, Ahmed et al. 2014, van Geen 2015).
5. Conclusions
This analysis sought to evaluate the effectiveness of arsenic removal at the household-level in rural Bangladesh. To our knowledge, this was the largest and longest deployment of filters accompanied by monitoring of urinary arsenic. The results show that READ-F filters can temporarily reduce arsenic exposure for weeks to a few months, but should not be considered as a sustainable arsenic mitigation option over the long term.
Highlights.
Sustainably reducing water As exposure is a major environmental health challenge.
There is limited field evidence on prolonged efficacy of As removal water filters.
We evaluated the effectiveness of household-level As removal filters in Bangladesh.
Filters temporarily reduced urinary As, but only for a few weeks.
Filters should not be considered as a long-term mitigation option.
Acknowledgments
This work was supported by funding from NIH grants R01CA133595, R01ES017875, P42ES010349, P30ES009089, R00ES018890, and D43TW005724.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Diane Levy, Email: dl2015@cumc.columbia.edu.
Mohammad Hasan Shahriar, Email: shahriar@urb-bd.org.
Mohammad Nasir Uddin, Email: nasirbmb@gmail.com.
Abu B. Siddique, Email: suman_siddiq@yahoo.com.
Joseph H. Graziano, Email: jg24@cumc.columbia.edu.
Angela Lomax-Luu, Email: aml2221@cumc.columbia.edu.
Alexander van Geen, Email: avangeen@ldeo.columbia.edu.
Mary V. Gamble, Email: mvg7@cumc.columbia.edu.
References
- Ahmed MF, Ahuja S, Alauddin M, Hug SJ, Lloyd JR, Pfaff A, Pichler T, Saltikov C, Stute M, van Geen A. Ensuring safe drinking water in Bangladesh. Science. 2006;314(5806):1687–6888. doi: 10.1126/science.1133146. [DOI] [PubMed] [Google Scholar]
- Ahmed MFA, Ahmed T. Comprehensive Water Quality and Purification. S. Ahuja. Waltham, Elsevier; 2014. 1.8 - Status of Remediation of Arsenic Contamination of Groundwater in Bangladesh; pp. 104–121. [Google Scholar]
- Ahsan H, Chen Y, Parvez F, Argos M, Hussain AI, Momotaj H, Levy D, van Geen A, Howe G, Graziano J. Health Effects of Arsenic Longitudinal Study (HEALS): Description of a multidisciplinary epidemiologic investigation. J Expo Sci Environ Epidemiol. 2006;16(2):191–205. doi: 10.1038/sj.jea.7500449. [DOI] [PubMed] [Google Scholar]
- BBS/UNICEF. Progotir Pathey: Bangladesh multiple indicator cluster survey 2012–2013. Bangladesh Bureau of Statistics (BBS) and UNICEF; 2015. [Google Scholar]
- Berg M, Luzi S, Trang KPT, Viet PH, Giger W, Stüben D. Arsenic removal from groundwater by household sand filters: comparative field study, model calculations, and health benefits. Environmental Science & Technology. 2006;40(17):5567–5573. doi: 10.1021/es060144z. [DOI] [PubMed] [Google Scholar]
- BETV-SAM/DPHE/ITN. Water Safety Plan for READ-F Arsenic Removal Technology. 2007 Retrieved 4/07/2016, from http://www.buet.ac.bd/itn/publications/sector-documents/wsp-doc/READ-F%20WSP%20Jul%2001_2007%20v1.pdf.
- Chen Y, van Geen A, Graziano JH, Pfaff A, Malgosia M, Parvez F, Hussain AZMI, Slavkovich V, Tariqul I, Ahsan H. Reduction in urinary arsenic levels in response to arsenic mitigation efforts in Araihazar, Bangladesh. Environmental Health Perspectives. 2007;115(6):917–923. doi: 10.1289/ehp.9833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheng Z, van Geen A, Jing C, Meng X, Seddique A, Ahmed KM. Performance of a household-level arsenic removal system during 4-month deployments in Bangladesh. Environmental Science & Technology. 2004;38(12):3442–3448. doi: 10.1021/es0352855. [DOI] [PubMed] [Google Scholar]
- Cheng Z, Zheng Y, Mortlock R, Van Geen A. Rapid multi-element analysis of groundwater by high-resolution inductively coupled plasma mass spectrometry. Anal Bioanal Chem. 2004;379(3):512–518. doi: 10.1007/s00216-004-2618-x. [DOI] [PubMed] [Google Scholar]
- Carlin Danielle J, N MF, Bradham Karen D, Cowden John, Michelle H, Heacock HF, Lee Janice S, Thomas David J, Thompson Claudia, Erik J Tokar, W MP, Birnbaum Linda S, Suk William A. Arsenic and environmental health: State of the science and future research opportunities. Environmental Health Perspectives. 2015 doi: 10.1289/ehp.1510209. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussam A, Munir AK. A simple and effective arsenic filter based on composite iron matrix: Development and deployment studies for groundwater of Bangladesh. Journal of Environmental Science and Health Part A. 2007;42(12):1869–1878. doi: 10.1080/10934520701567122. [DOI] [PubMed] [Google Scholar]
- Inauen J, Hossain MM, Johnston RB, Mosler H-J. Acceptance and use of eight arsenic-safe drinking water options in Bangladesh. PLoS ONE. 2013;8(1):e53640. doi: 10.1371/journal.pone.0053640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston R, Hug SJ, Inauen J, Khan NI, Mosler H-J, Yang H. Enhancing arsenic mitigation in Bangladesh: Findings from institutional, psychological, and technical investigations. Science of the Total Environment. 2014;488:477–483. doi: 10.1016/j.scitotenv.2013.11.143. [DOI] [PubMed] [Google Scholar]
- Johnston RB, Hanchett S, Khan MH. The socio-economics of arsenic removal. Nature Geoscience. 2010;3(1):2–3. [Google Scholar]
- Jones-Hughes T, Peters J, Whear R, Cooper C, Evans H, Depledge M, Pearson M. Are interventions to reduce the impact of arsenic contamination of groundwater on human health in developing countries effective? A systematic review. Environmental Evidence. 2013;2(1):11. [Google Scholar]
- Milton AH, Smith W, Dear K, Ng J, Sim M, Ranmuthugala G, Lokuge K, Caldwell B, Rahman A, Rahman H, Shraim A, Huang D, Shahidullah SM. A Randomised intervention trial to assess two arsenic mitigation options in Bangladesh. Journal of Environmental Science and Health, Part A. 2007;42(12):1897–1908. doi: 10.1080/10934520701567197. [DOI] [PubMed] [Google Scholar]
- Neumann A, Kaegi R, Voegelin A, Hussam A, Munir AK, Hug SJ. Arsenic removal with composite iron matrix filters in Bangladesh: A field and laboratory study. Environmental Science & Technology. 2013;47(9):4544–4554. doi: 10.1021/es305176x. [DOI] [PubMed] [Google Scholar]
- Nixon DE, Mussmann GV, Eckdahl SJ, Moyer TP. Total arsenic in urine: palladium-persulfate vs nickel as a matrix modifier for graphite furnace atomic absorption spectrophotometry. Clin Chem. 1991;37(9):1575–1579. [PubMed] [Google Scholar]
- Peters BA, Hall MN, Liu X, Parvez F, Sanchez TR, van Geen A, Mey JL, Siddique AB, Shahriar H, Uddin MN. Folic acid and creatine as therapeutic approaches to lower blood arsenic: A randomized controlled trial. Environmental Health Perspectives. 2015 doi: 10.1289/ehp.1409396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reuter W, Davidowski L, Neubauer K. Speciation of five arsenic compounds in urine by HPLC/ICP-MS. Franklin, MA: PerkinElmerSCIEX, PerkinElmer Life and Analytical Sciences; 2003. [Google Scholar]
- Singh R, Singh S, Parihar P, Singh VP, Prasad SM. Arsenic contamination, consequences and remediation techniques: A review. Ecotoxicology and Environmental Safety. 2015;112:247–270. doi: 10.1016/j.ecoenv.2014.10.009. [DOI] [PubMed] [Google Scholar]
- Straif K, Benbrahim-Tallaa L, Baan R, Grosse Y, Secretan B, El Ghissassi F, Bouvard V, Guha N, Freeman C, Galichet L. A review of human carcinogens—part C: metals, arsenic, dusts, and fibres. The Lancet Oncology. 2009;10(5):453–454. doi: 10.1016/s1470-2045(09)70134-2. [DOI] [PubMed] [Google Scholar]
- van Geen A, Ahmed EB, Pitcher L, Mey JL, Ahsan H, Graziano JH, Ahmed KM. Comparison of two blanket surveys of arsenic in tubewells conducted 12 years apart in a 25 km2 area of Bangladesh. Science of the Total Environment. 2014;488:484–492. doi: 10.1016/j.scitotenv.2013.12.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Geen A, Cheng Z, Jia Q, Seddique AA, Rahman MW, Rahman MM, Ahmed KM. Monitoring 51 community wells in Araihazar, Bangladesh, for up to 5 years: Implications for arsenic mitigation. Journal of Environmental Science and Health Part A. 2007;42(12):1729–1740. doi: 10.1080/10934520701564236. [DOI] [PubMed] [Google Scholar]
- Van Geen A, Cheng Z, Seddique A, Hoque M, Gelman A, Graziano J, Ahsan H, Parvez F, Ahmed K. Reliability of a commercial kit to test groundwater for arsenic in Bangladesh. Environmental Science & Technology. 2005;39(1):299–303. [PubMed] [Google Scholar]
- Van Geen A, Ahmed KM, Ahmed EB, Choudhurry I, Mozumder MR, Bostick BC, Mailloux BJ. Inequitable allocation of deep community wells for reducing arsenic exposure in Bangladesh. Journal of Water Sanitation and Hygiene for Development. 2015 doi: 10.2166/washdev.2015.115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zheng Y, Stute M, van Geen A, Gavrieli I, Dhar R, Simpson HJ, Schlosser P, Ahmed KM. Redox control of arsenic mobilization in Bangladesh groundwater. Applied Geochemistry. 2004;19(2):201–214. [Google Scholar]