

Abstract
The management of massive rotator cuff tears remains a challenge for physicians, with failure rates being higher when compared with smaller tears. Many surgical treatment options exist including debridement with biceps tenodesis, complete repair, partial repair, repair with augmentation devices, superior capsule reconstruction, tendon transfer, and reverse total shoulder arthroplasty. The purpose of this article is to describe our preferred surgical technique for a complete arthroscopic repair using an extended linked, knotless, double-row construct.
The surgical management of massive rotator cuff tears is challenging to orthopaedic surgeons. The prevalence of massive rotator cuff tears has been reported to be as high as 40% of all rotator cuff tears, and failure rates are higher when compared with smaller tears.1, 2, 3 Many surgical treatment options exist including debridement with biceps tenodesis, complete repair, partial repair, repair with patch augmentation, superior capsule reconstruction, tendon transfer, and reverse total shoulder arthroplasty. However, concerns regarding longevity of arthroplasty implants and morbidity associated with tendon transfers lend these treatment options to be less desirable in younger and more active patients.
Advances in arthroscopic equipment and surgical technique have allowed for many massive rotator cuff tears to be anatomically repaired arthroscopically in a similar fashion to smaller tears. This is important because accurate restoration of the anatomic footprint may favor healing because of favorable biomechanical conditions.4 Furthermore, the use of knotless repair constructs may help improve healing potential because the lack of medial knots may improve vascular inflow and the use of a wider suture material helps distribute the compressive forces over a larger surface area of the repaired cuff tendon, thereby preventing suture cut-through.5 Additional benefits include decreased operative time6 and elimination of potential postoperative knot impingement within the subacromial space.7 The purpose of this report is to describe an arthroscopic knotless technique using an extended linked, double-row construct for the repair of massive rotator cuff tears (Video 1, Table 1).
Table 1.
Summary of Surgical Steps
| Surgical Steps | Risks | Pearls |
|---|---|---|
| Diagnostic arthroscopy | Missing of concomitant lesions | Performing a thorough and standardized examination allows for identification of concomitant injuries. |
| Mobilization of rotator cuff | Insufficient release leading to the false assessment of a tear as “irreparable” | A reasonable though not overly aggressive release should be performed. |
| Overly aggressive release leading to traction damage to the suprascapular nerve and compromised blood supply | If complete footprint coverage cannot be achieved, alternative techniques such as patch augmentation should be performed. | |
| Medial-row anchor insertions | Dog-ear formation | The surgeon should start with the anterior and posterior anchors and work from outside in. |
| Suture passage through rotator cuff tendons | Later type 2 rotator cuff repair failure | The sutures should be passed 2-3 mm lateral to the musculotendinous junction. The surgeon can achieve appropriate bursal- and articular-sided tension by using a grasper to reduce the tendon and then taking differential bites through each leaflet when delaminations are present. |
| Lateral-row anchor insertions and tendon fixation | Insufficient room | Planning for anchors should be performed by marking with a radiofrequency device. |
| Soft bone | The bone quality should be assessed with a punch. If the bone is really soft, a 5.5-mm BioComposite SwiveLock should be used. | |
| Dog-ear formation | The surgeon should start with the anterior and posterior anchors and work from outside in. | |
| Postoperative rehabilitation | Postoperative stiffness | The patient should perform early passive range of motion for 3-4 wk. The patient should progress to full passive motion and start active and active-assisted motion at 6 wk postoperatively. |
Surgical Technique
Surgery is performed with the patient under general anesthesia with an additional interscalene block. The patient is placed in the beach-chair position with a pneumatic arm holder (Tenet T-Max Beach Chair and Spider arm positioner; Smith & Nephew, Memphis, TN), and the index shoulder is prepared and draped in a sterile fashion. A standard posterior viewing portal is established, and all intra-articular surfaces are visualized (560 H Camera System; Smith & Nephew). An anterior working portal is made through the rotator interval. An extensive glenohumeral debridement and subacromial bursectomy are routinely performed (Fig 1). If loose bodies are encountered, they are removed. An acromioplasty with release of the coracoacromial ligament is performed if a type III acromion or impingement lesion is identified.
Fig 1.

Arthroscopic view through the anterolateral portal in a left shoulder in the modified beach-chair position. An extensive glenohumeral debridement with lysis of adhesions around the rotator cuff tendon is performed to mobilize the tendon.
Attention is then turned to assessment and repair of the massive posterosuperior rotator cuff tear (Fig 2, Fig 3, Fig 4).8 A complete rupture of the supraspinatus, infraspinatus, and teres minor tendons is noted in the case shown in this report. The rotator cuff tear margins are assessed for mobility with a grasper. If necessary, intra- and extra-articular releases are performed to allow for greater mobilization of the tendons. The footprint on the greater tuberosity is debrided to a bleeding surface with an arthroscopic shaver (Synergy Resection Shaver Console and APS II Handpiece; Arthrex, Naples, FL) to optimize tendon-to-bone healing.
Fig 2.
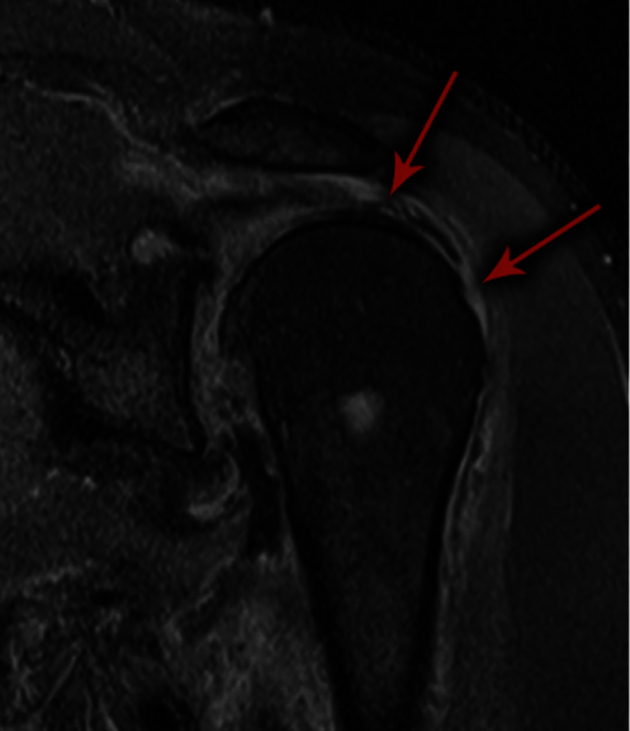
Preoperative magnetic resonance imaging (coronal, T2) in a left shoulder showing a massive posterosuperior rotator cuff tear (arrows).
Fig 3.
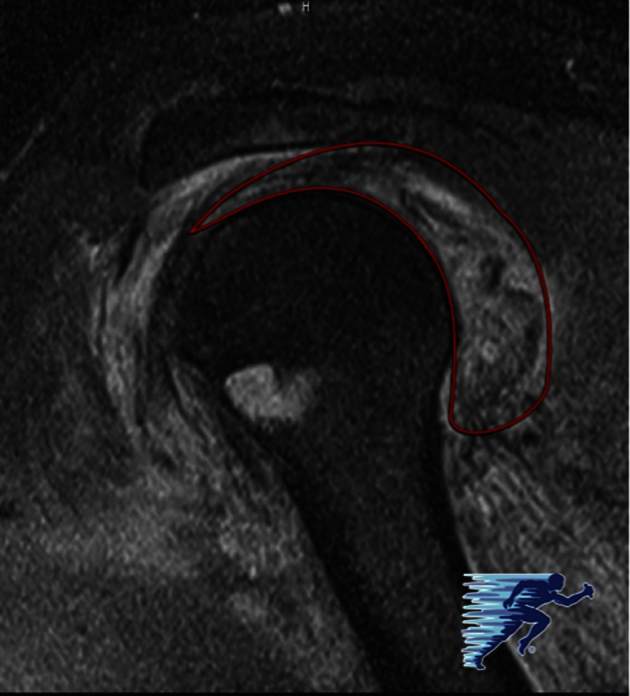
Preoperative magnetic resonance imaging (sagittal, T2) in a left shoulder showing a massive posterosuperior rotator cuff tear (red border).
Fig 4.
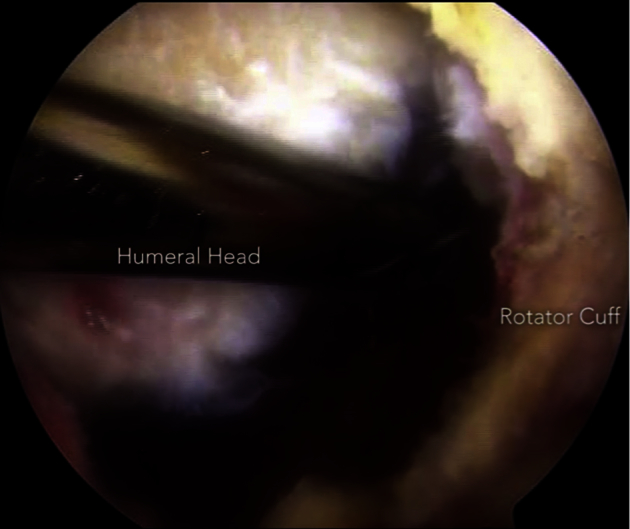
Arthroscopic view from the posterolateral portal in a left shoulder in the modified beach-chair position. A massive tear of the rotator cuff is visualized.
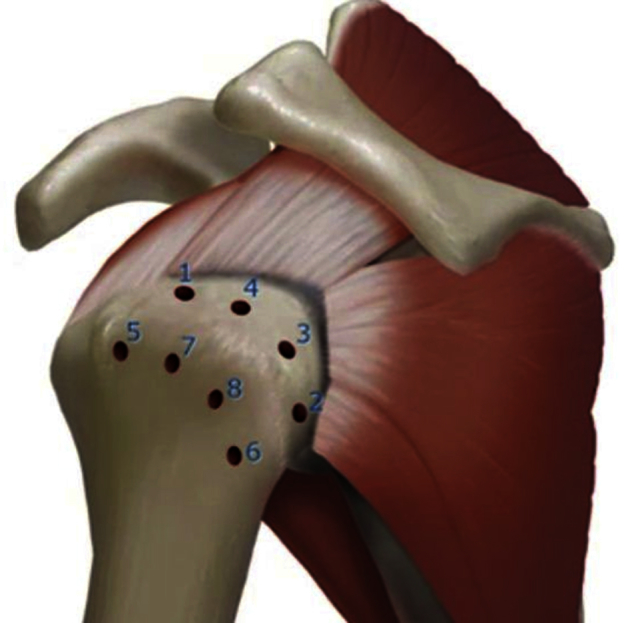
The insertion spots for the medial row of anchors are determined (Fig 5). Correct anchor placement is of particular relevance in repairs of massive rotator cuff tears, especially with double-row repairs. The risk of anchors punching out of the shoulder and fractures of bone bridges between anchors increases with the increasing number of anchors. It is therefore crucial to determine the insertion sites for the anchors before inserting them. We use a radiofrequency device to mark the spots where anchors are supposed to be inserted. We recommend keeping a bone bridge of at least 15 mm between anchors in the anteroposterior mediolateral direction.
Fig 5.
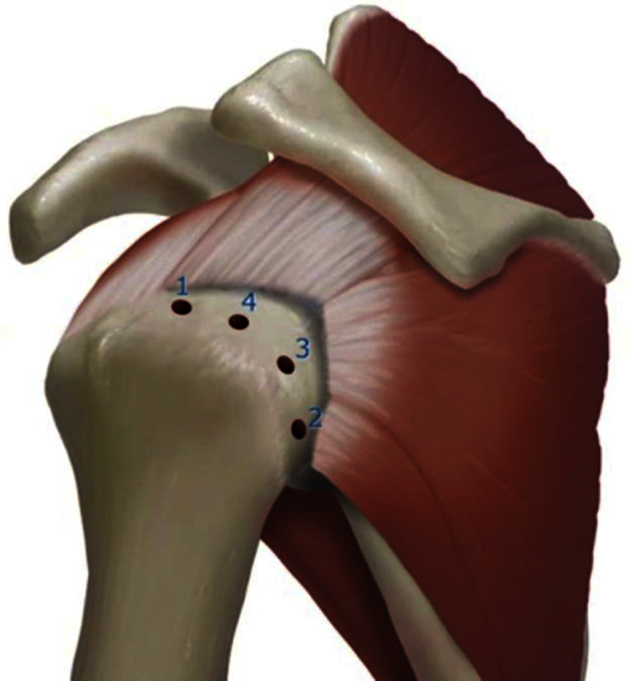
Preferred placement and order of insertion of the medial-row anchors in a left shoulder. We prefer to work from outside in to try to avoid dog ears. Figure provided by the medical illustration department of Arthrex.
Bone sockets are prepared with an arthroscopic punch. Four 4.75-mm vented BioComposite SwiveLock suture anchors (Arthrex), each loaded with No. 2 FiberTape (Arthrex), are placed medially in the rotator cuff footprint 1 to 2 mm lateral to the articular cartilage margin of the humeral head (Fig 6). The initial anchor is placed anteriorly, and the second anchor is placed posteriorly (Fig 7). Working from outside in helps avoid the formation of dog ears.
Fig 6.
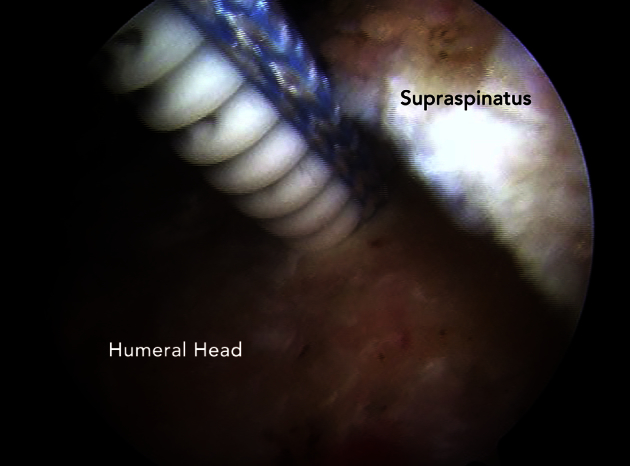
Arthroscopic view through the posterolateral portal in a left shoulder. The 4.75-mm BioComposite SwiveLock anchor loaded with FiberTape is placed 1 to 2 mm adjacent to the articular cartilage margin of the humeral head.
Fig 7.
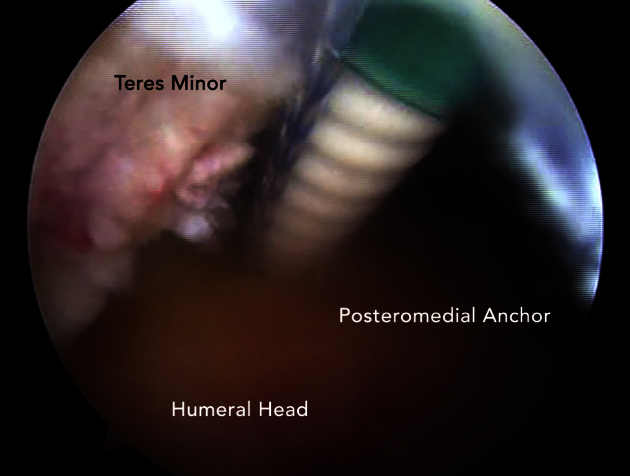
Arthroscopic view through the anterolateral portal in a left shoulder showing placement of the posteromedial suture anchor.
The tendons are pulled with a grasper from the lateral portal, and each limb of the suture tape is passed through the tendon approximately 2 to 3 mm lateral to the musculotendinous junction by use of a suture lasso (QuickPass SutureLasso; Arthrex) (Fig 8). Every effort should be made to incorporate delaminations of the rotator cuff tendon into the repair, with differential bites of tissue as needed to equalize tension across articular and bursal layers. These steps are repeated until each suture tape has been passed through the rotator cuff tendon. At this point, the medial row with the four anchors is visualized.
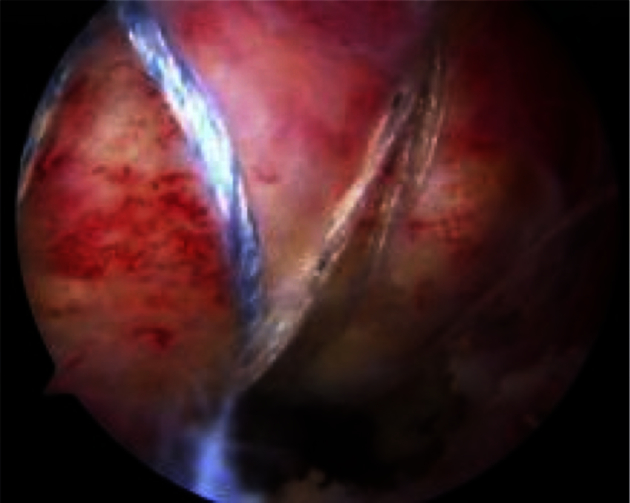
Fig 8.
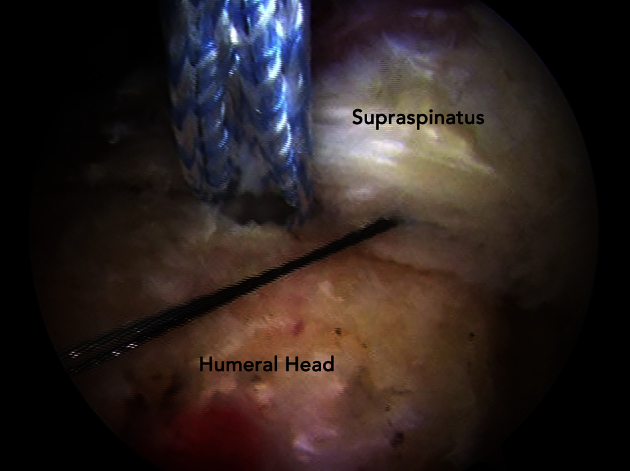
Arthroscopic view through the posterolateral portal in a left shoulder. The rotator cuff tendon is grasped, and a suture lasso is used to shuttle the FiberTape sutures back through the tendon. It is important to pass the sutures lateral to the musculotendinous junction to avoid damage.
The FiberTapes (Arthrex) are then loaded sequentially onto each of the four anchors as they are inserted into the lateral row of the repair. In a similar fashion to the medial row, a bone punch is used to prepare the bone sockets for the lateral-row anchors (Fig 9). The lateral anchors should be placed 5 to 10 mm lateral to the edge of the greater tuberosity and approximately 15 to 20 mm from the medial row of anchors. The limbs of the suture tapes are tensioned through the eyelet of the SwiveLock anchor, and the rotator cuff is compressed down onto the footprint by the extended linked SpeedBridge repair technique (Arthrex). The posterior and anterior anchors are placed first and then the middle anchors (Fig 10). This acts to tension the tissues and the suture tapes more evenly. The complete repair construct with eight anchors is visualized (Fig 11, Fig 12), showing a low-profile complete closure of the rotator cuff around the humeral head.
Fig 9.
Placement and order of insertion of all suture anchor locations (medial and lateral row) in a left shoulder. Figure provided by the medical illustration department of Arthrex.
Fig 10.
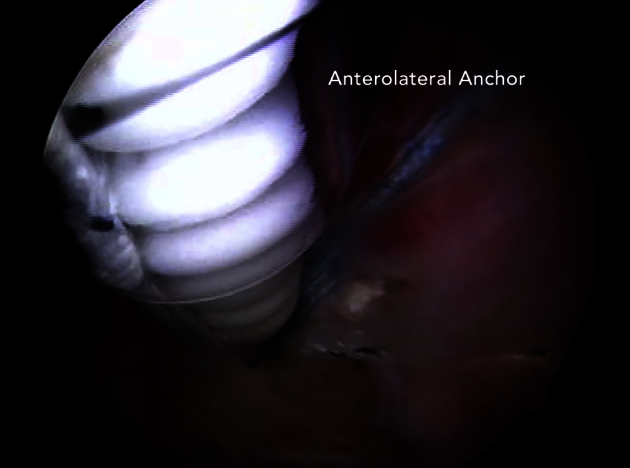
Arthroscopic view through the posterolateral portal in a left shoulder. The FiberTapes are tensioned through the eyelet of the SwiveLock anchors. This compresses the rotator cuff down to the footprint. The anterolateral anchor is placed first in the lateral row, followed by the posterolateral anchor. Working from outside in helps avoid the formation of dog ears.
Fig 11.
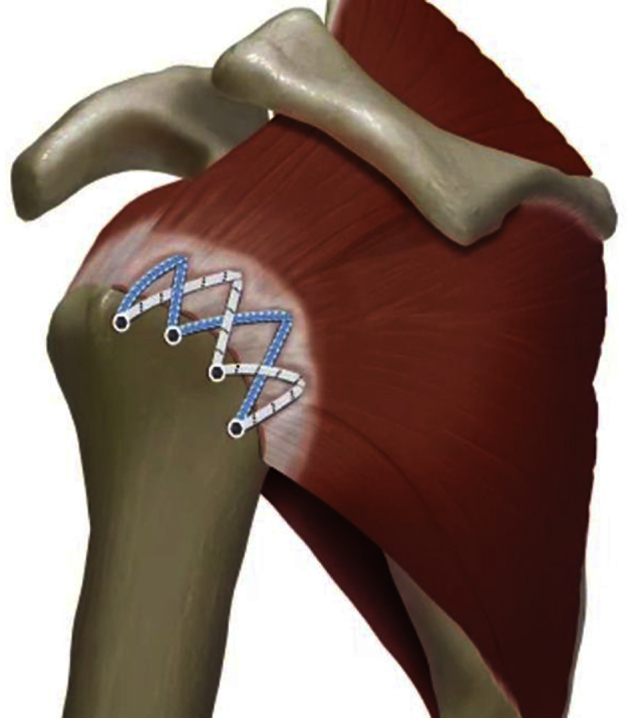
Completed extended linked, double-row rotator cuff repair construct in a left shoulder. Figure provided by the medical illustration department of Arthrex.
Fig 12.
Arthroscopic view from the anterolateral portal in a left shoulder that is positioned in the modified beach-chair position. The final low-profile, extended linked, double-row repair construct is visualized.
If pathology of the long head of the biceps tendon is identified, it undergoes tenotomy for a tenodesis. Our preferred technique is a subpectoral biceps tenodesis using a small incision in the axillary fold. The tendon is fixed in a 7- or 8-mm unicortical socket with a PEEK (polyether ether ketone) tenodesis screw (Arthrex).9 The wounds are then copiously irrigated and meticulously closed in layers. Steri-Strips (3M, St Paul, MN) and dry sterile dressings are applied.
Our preferred postoperative rehabilitation protocol consists of early passive range of motion for 3 to 4 weeks.10 Limitations of motion of 30° of external rotation, 90° of abduction, and 120° of forward flexion are used when the tissue quality or repair security is compromised. The patient then progresses to full passive motion and starts active and active-assisted motion approximately 6 weeks postoperatively. A full return to activities including sports is typically achieved after 4 to 6 months.
Discussion
Arthroscopic rotator cuff repair techniques have evolved over the past 3 decades to reach their current state. The advances in technique, surgical skill, and arthroscopic equipment allow for many massive rotator cuff tears to be repaired arthroscopically. The described technique provides orthopaedic surgeons an additional arthroscopic treatment option for massive rotator cuff tears.
There has been great debate regarding the use of single-row versus double-row repair constructs. Double-row rotator cuff repairs have been shown to have superior biomechanical properties on the basis of increased load to failure, as well as better restoration of the tendon footprint.11 Denard et al.12 noted that a double-row repair was 4.89 times more likely to result in a good or excellent University of California, Los Angeles score. A recent meta-analysis of Level I randomized clinical studies conducted by Millett et al.13 found a significantly higher retear rate in rotator cuff repairs performed with a single row compared with double-row repairs. However, no differences were noted in postoperative clinical outcome scores at a mean of less than 2 years. The aforementioned technique has the biomechanical advantages of a double-row repair whereas the interconnectivity and self-reinforcement of the construct allow for shear stresses to be converted into compressive forces, which reinforce the repair.6 The vented anchors also allow access to bone marrow contents to enhance the healing environment.
The role of platelet-rich plasma (PRP) to enhance healing is not fully understood. A recent meta-analysis conducted by Warth et al.14 analyzed the effects of PRP on the clinical and structural outcomes after arthroscopic repair of full-thickness rotator cuff tears. They did not note any statistically significant differences in overall gain in outcome scores or retear rates between treatment groups. However, when they analyzed tears greater than 3 cm in the anterior-posterior direction, retear rates were significantly lower when PRP was used. Further studies are needed to help elucidate the benefits of PRP in rotator cuff repair.
Repair of massive rotator cuff tears can be challenging. The described technique shows an extended linked, knotless, double-row construct, facilitating the complete arthroscopic repair of a massive, posterosuperior three-tendon tear.
Footnotes
The authors report the following potential conflict of interest or source of funding: J.A.G., M.P., and P.J.M. receive support from Steadman Philippon Research Institute. Corporate sponsorship for Steadman Philippon Research Institute is received from Ossur, Smith & Nephew Endoscopy, Siemens Medical Solutions, and Arthrex. P.J.M. also receives support from Arthrex, Myos, GameReady, and VuMedi.
Supplementary Data
Our preferred surgical technique for repair of massive rotator cuff tears using an extended linked, double-row construct. The patient is placed in the modified beach-chair position. A diagnostic arthroscopy is performed, and concomitant pathologies are addressed. The rotator cuff tear is assessed. The greater tuberosity footprint is debrided. The insertion spots of the medial row are determined, and holes are created with an arthroscopic punch. The anchors are inserted and sutures passed through the tendon. The lateral row is then established and repair completed.
References
- 1.Bedi A., Dines J., Warren R.F., Dines D.M. Massive tears of the rotator cuff. J Bone Joint Surg Am. 2010;92:1894–1908. doi: 10.2106/JBJS.I.01531. [DOI] [PubMed] [Google Scholar]
- 2.Greenspoon J.A., Petri M., Warth R.J., Millett P.J. Massive rotator cuff tears: Pathomechanics, current treatment options, and clinical outcomes. J Shoulder Elbow Surg. 2015;24:1493–1505. doi: 10.1016/j.jse.2015.04.005. [DOI] [PubMed] [Google Scholar]
- 3.Galatz L.M., Ball C.M., Teefey S.A., Middleton W.D., Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86:219–224. doi: 10.2106/00004623-200402000-00002. [DOI] [PubMed] [Google Scholar]
- 4.Park M.C., ElAttrache N.S., Tibone J.E., Ahmad C.S., Jun B.L., Lee T.Q. The effect of abduction and rotation on footprint contact for single-row, double-row, and modified double-row rotator cuff repair techniques. Am J Sports Med. 2009;37:1599–1608. doi: 10.1177/0363546509332506. [DOI] [PubMed] [Google Scholar]
- 5.Vaishnav S., Millett P.J. Arthroscopic rotator cuff repair: Scientific rationale, surgical technique, and early clinical and functional results of a knotless self-reinforcing double-row rotator cuff repair. J Shoulder Elbow Surg. 2011;19:83–90. doi: 10.1016/j.jse.2009.12.012. [DOI] [PubMed] [Google Scholar]
- 6.Burkhart S.S., Adams C.R., Schoolfield J.D. A biomechanical comparison of 2 techniques of footprint reconstruction for rotator cuff repair: The SwiveLock-FiberChain construct versus standard double-row repair. Arthroscopy. 2009;25:274–281. doi: 10.1016/j.arthro.2008.09.024. [DOI] [PubMed] [Google Scholar]
- 7.Yamakado K., Katsuo S., Mizuno K., Arakawa H., Hayashi S. Medial-row failure after arthroscopic double-row rotator cuff repair. Arthroscopy. 2010;26:430–435. doi: 10.1016/j.arthro.2009.07.022. [DOI] [PubMed] [Google Scholar]
- 8.Millett P.J., Warth R.J. Posterosuperior rotator cuff tears: Classification, pattern recognition, and treatment. J Am Acad Orthop Surg. 2014;22:521–534. doi: 10.5435/JAAOS-22-08-521. [DOI] [PubMed] [Google Scholar]
- 9.Millett P.J., Sanders B., Gobezie R., Braun S., Warner J.J. Interference screw vs. suture anchor fixation for open subpectoral biceps tenodesis: Does it matter? BMC Musculoskelet Disord. 2008;9:121. doi: 10.1186/1471-2474-9-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Millett P.J., Wilcox R.B., III, O’Holleran J.D., Warner J.J. Rehabilitation of the rotator cuff: An evaluation-based approach. J Am Acad Orthop Surg. 2006;14:599–609. doi: 10.5435/00124635-200610000-00002. [DOI] [PubMed] [Google Scholar]
- 11.Mazzocca A.D., Millett P.J., Guanche C.A., Santangelo S.A., Arciero R.A. Arthroscopic single-row versus double-row suture anchor rotator cuff repair. Am J Sports Med. 2005;33:1861–1868. doi: 10.1177/0363546505279575. [DOI] [PubMed] [Google Scholar]
- 12.Denard P.K., Jiwani A.Z., Lädermann A., Burkhart S.S. Long-term outcome of arthroscopic massive rotator cuff repair: The importance of double row fixation. Arthroscopy. 2012;28:909–915. doi: 10.1016/j.arthro.2011.12.007. [DOI] [PubMed] [Google Scholar]
- 13.Millett P.J., Warth R.J., Dornan G.J., Lee J.T., Spiegl U.J. Clinical and structural outcomes after arthroscopic single-row versus double-row rotator cuff repair: A systematic review and meta-analysis of level I randomized clinical trials. J Shoulder Elbow Surg. 2014;23:586–597. doi: 10.1016/j.jse.2013.10.006. [DOI] [PubMed] [Google Scholar]
- 14.Warth R.J., Dornan G.J., James E.W., Horan M.P., Millett P.J. Clinical and structural outcomes after arthroscopic repair of full-thickness rotator cuff tears with and without platelet-rich product supplementation: A meta-analysis and meta regression. Arthroscopy. 2015;31:306–320. doi: 10.1016/j.arthro.2014.09.007. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Our preferred surgical technique for repair of massive rotator cuff tears using an extended linked, double-row construct. The patient is placed in the modified beach-chair position. A diagnostic arthroscopy is performed, and concomitant pathologies are addressed. The rotator cuff tear is assessed. The greater tuberosity footprint is debrided. The insertion spots of the medial row are determined, and holes are created with an arthroscopic punch. The anchors are inserted and sutures passed through the tendon. The lateral row is then established and repair completed.