

Abstract
Two studies examined racial identity (RI) as a protective factor against substance use cognitions among African American young adults who either envisioned or experienced racial discrimination. In Study 1, participants envisioned a discrimination or nondiscrimination scenario, and then their willingness to use drugs and an indirect measure of substance use were assessed. Discrimination was associated with higher levels of use cognitions among participants with low levels of RI. In Study 2, participants were excluded or included in an online game (Cyberball) by White peers and then engaged in an RI-affirmation or control writing task. Participants attributed this exclusion to racial discrimination. Excluded participants who did not affirm their RI reported the highest levels of substance use cognitions, especially if they had engaged in higher levels of previous substance use. These findings highlight the importance of RI among Black young adults and the impact of discrimination on health behaviors.
Keywords: discrimination, racial identity, substance use, affirmation, health
African Americans report experiencing more discrimination than do other minority groups (e.g., Landrine, Klonoff, Corral, Fernandez, & Roesch, 2006). These stressful experiences have been linked to worse physical health (e.g., higher blood pressure) and mental health (e.g., symptoms of depression and distress) as well as more negative health behaviors, including substance use (for reviews, see Pascoe & Smart Richman, 2009; D. R. Williams & Mohammed, 2009). For example, studies have found correlations between reports of discrimination among Blacks and reports of alcohol, tobacco, and drug use (e.g., Borrell et al., 2007; Landrine et al., 2006; Martin, Tuch, & Roman, 2003). Gibbons and colleagues found evidence of a prospective link between perceived discrimination and self-reported substance use 2 and 5 years later among Black adolescents and their parents (Gibbons et al., 2007; Gibbons, Gerrard, Cleveland, Wills, & Brody, 2004). A recent experimental study has also supported this relation among Black young adults. Gibbons and colleagues (2010) demonstrated that imagining a discriminatory (vs. nondiscriminatory) experience was associated with higher levels of willingness to use substances among those who had used substances in the past. Feelings of anger mediated this relation, and reports of supportive parenting buffered the negative effects of discrimination on drug willingness.
Young adulthood is an important time to examine discrimination among Blacks, as they are more likely to experience racial discrimination following high school (Greene, Way, & Pahl, 2006). This is also a time when the “racial crossover effect” becomes evident, as rates of drug use and abuse, which tend to be lower among Black adolescents, begin to exceed those of Whites in young adulthood (e.g., Watt, 2008). In addition, clinic admissions, drug-related mortality, and other negative consequences of use increase for Blacks during this time (French, Finkbiner, & Duhamel, 2002; Vega & Gil, 1998). It has been suggested that racial discrimination is an important factor that contributes to this disparity (Thomas, Price, & Lybrand, in press). Therefore, it is important to understand individual difference factors that are malleable and may buffer the negative impact of discrimination on health cognitions. One such factor is racial identity (RI).
RI and Discrimination
Ethnic/racial identity refers to an aspect of self-concept and social identity that derives from individuals’ knowledge of their ethnic or racial group membership and the significance and meaning they attach to that group membership (Phinney, 1992; Tajfel, 1981). RI is associated with lower psychological stress, distress, and well-being (Sellers, Caldwell, Schmeelk-Cone, & Zimmerman, 2003; Sellers, Copeland-Linder, Martin, & Lewis, 2006). Self-identification as a group member, a sense of belonging, pride in one’s group, and involvement in the activities of the group are all key aspects of RI (Phinney, 1990). Because of their unique minority status, RI is a central aspect of self-concept for young African Americans and may have important implications for their health, especially in the context of racial discrimination (e.g., Greene et al., 2006; D. R. Williams, Spencer, & Jackson, 1999).
Some researchers have suggested that RI is a buffer against the negative effects of discrimination on psychological and physiological health (Cross, 1991; Phinney, 1996; Sellers, Smith, Shelton, Rowley, & Chavous, 1998). For example, discrimination is positively related to physical health problems for Blacks with low levels of RI, but as the level of RI increases, this adverse relation decreases (D. R. Williams et al., 1999). RI is also protective among Blacks against the effects of racial discrimination on perceived stress, depression, psychological well-being, increases in problem behavior, and involvement with deviant friends (e.g., Greene et al., 2006; Sellers et al., 2003; Wong, Eccles, & Sameroff, 2003). According to the rejection-identification model (Branscombe, Schmitt, & Harvey, 1999), perceived discrimination represents rejection by the majority group and is associated with RI enhancement, which, in turn, buffers the negative effects of discrimination on psychological well-being. However, some researchers have not found that RI protects against perceived discrimination (Brondolo, ver Halen, Pencille, Beatty, & Contrada, 2009). Recent reviews have stated that experimental research is needed to address this inconsistency and, specifically, to determine if RI is protective and to assess the effects of RI and racial salience when the discriminatory event takes place (Brondolo et al., 2009; Pascoe & Smart Richman, 2009). That was the goal of the current studies.
RI and Substance Use
Minority youth who have high levels of RI appear to be able to resist or delay substance use initiation and have more negative attitudes toward substance use and higher perceived drug risk than do youths who have low levels of RI (Belgrave, Brome, & Hampton, 2000; Brook & Pahl, 2005; Wallace & Fisher, 2007). For example, Black university students with higher RI are less likely to drink alcohol and use marijuana than those with lower RI (Pugh & Bry, 2007). In addition, RI is associated with more negative substance-related attitudes, greater perceived parental anger if their child uses substances, and less reported substance use (Holley, Kulis, Marsiglia, & Keith, 2006). Consistent with these findings, culturally based prevention programs that include enhancement of RI are effective at preventing or delaying substance use. An example is the Strong African American Families Program (SAAF), which includes the promotion of RI among Black adolescents and has been found to delay the initiation of substance use (Brody et al., 2004; Gerrard et al., 2006).
Although researchers have speculated that RI may have the same buffering effect against discrimination for substance use as it does for psychological health (e.g., Cross, 1991; Phinney, 1996), only one study we are aware of has examined this. Using a cross-sectional design, Chae and colleagues (2008) found that among Asian Americans reporting high levels of discrimination experiences, the probability of current smoking was lower if they also reported high RI. However, no research has examined the causal nature of the impact of discrimination and RI on substance use vulnerability among Blacks. For the present studies, experimental methods were used to examine whether RI is a buffer against pro–substance use cognitions when Black young adults imagine a discrimination-based scenario (Study 1). We also examined whether RI affirmation is protective against substance use vulnerability after Black young adults are socially excluded by Whites (Study 2).
Measuring Substance Use Cognitions
Willingness
The majority of studies examining substance use cognitions have employed only explicit measures of intentions or expectations to use, which can be susceptible to self-presentation (Stacy, 1997). The current studies follow a recent trend toward looking at both explicit and indirect measures. Our explicit measure is taken from previous research on substance use vulnerability and guided by the prototype/willingness model (Gerrard, Gibbons, Houlihan, Stock, & Pomery, 2008; Gibbons, Gerrard, & Lane, 2003). This model is a modified dual-process model focusing on the cognitions that mediate the effects of environmental factors on substance use. A central tenet of the model is a belief that not all health behaviors are planned or intentional, especially when those behaviors involve health risk among adolescents and young adults (cf. Reyna & Farley, 2006). Instead, many risky behaviors are reactions to risk-conducive social situations (Gibbons et al., 2003). These reactions are captured in a proximal antecedent to risk behavior that was used in the current studies: behavioral willingness. Willingness is defined as an openness to risk opportunity—what one would be willing to do when encountering a risk-conducive situation. Previous research has demonstrated that discrimination experiences are associated with higher levels of willingness and that willingness is a strong predictor of future substance use behavior (e.g., Gibbons et al., 2004; Gibbons et al., 2010).
Direct versus indirect
We followed the example of other researchers (e.g., Stacy, 1997; Thush et al., 2007) by also assessing substance use cognitions indirectly. These cognitive measures predict additional variance in substance use behavior and capture cognitions not always found using more explicit methods (e.g., Krank, Schoenfeld, & Frigon, 2010). The indirect method we employed was to have participants imagine and then describe a hypothetical situation (a party). Their responses were coded for mentions of substance use (Krank et al., 2010, used similar methods).
Experiment 1
Overview
The first study involved new analyses of data from a sub-sample of participants in Study 2 of Gibbons et al. (2010). This study found that willingness to use drugs was significantly increased when participants envisioned a racial discrimination (vs. nondiscrimination) scenario, but only if they were substance users. The study did not examine RI as a protective factor, however, and it did not examine the impact of envisioned discrimination on the scenario-based risk cognitions. Only participants who reported past drug use were included in Study 1. Thus, Study 1 focused on self-reported RI as an important protective factor against two independent risk cognitions (willingness and scenario-based risk) among participants at greatest risk for using substances to deal with discriminatory experiences. We predicted an interaction such that when imagining a discriminatory experience (compared to a nonstress or nondiscriminatory stress experience), individuals with lower RI would have higher levels of risk cognitions. All analyses controlled for gender, self-concept, and supportive parenting.
Method
Participants: The Family and Community Health Study (FACHS)
Potential participants were members of the panel in FACHS, which is an ongoing study examining the impact of environmental factors on the mental and physical health of African American families. Community coordinators and school liaisons compiled lists of all families in their area that included a fifth grade African American child. Potential families, chosen randomly from the lists, received an introductory letter followed by a recruitment phone call. A total of 889 families, 467 in Iowa and 422 in Georgia, were recruited for participation in FACHS. Each family had a “target” child between the ages of 10 and 12 at Wave 1; 779 remained in the panel at Wave 2 (M age = 12.5, 54% female). Measures of RI at Wave 2 were used in the current study. The target and his or her primary caregiver (85% were the biological mothers) were interviewed separately. Two interviews were conducted in participants’ homes or nearby locations by Black interviewers and included a computer-assisted personal interview. The primary caregivers received $100 and the target $70 for their participation. For further description of the FACHS sample and recruitment, see Brody et al. (2001), Gerrard, Gibbons, Stock, Vande Lune, and Cleveland (2005), and Simons et al. (2002).
Participants: Experimental study
From the list of Iowa FACHS targets, we randomly chose 90 who had reported drug use in previous waves of FACHS and 85 who reported no use. These 175 young adults received letters inviting them to participate in the lab study; 139 participated.1 However, the RI measure was available only for those who participated in Wave 2 of FACHS (T1; n = 116). Of the 116 who participated in T1 and the lab study (T2), 55% (n = 64) reported drug use in the past 6 months. Thus, the final sample consisted of 64 Black young adults (42 females, M = 18 years of age).
Procedure
Participants were told that the purpose of the study was to examine African Americans’ health attitudes and behaviors and reactions to stressful and successful experiences. Responses were entered on a computer. Participants were randomly assigned to one of three conditions involving imagining being in a work-related situation. The no-stress experience involved trying to find an address while working as a delivery person without any time pressure. The stress-only condition involved falling behind at work and getting a negative evaluation from the boss. In the discrimination condition, participants imagined that their boss and coworkers had discriminated against them because of their race. Participants were asked to envision themselves in the scenario, describe how they would deal with the situation, indicate if they had ever experienced a similar situation, and then report how stressful they thought that situation would be. Willingness to use drugs was then assessed. Before the party scenario, two filler items were included: (a) willingness to help others and (b) describing a future goal.2 Finally, for the scenario-based (indirect) risk measure, participants were asked to imagine they were at a party to celebrate a promotion. They were asked who would be at their party and then answered two open-ended questions: “What are you [your guests] doing at the party?” These responses were coded for mentions of substance use. Participants were paid $105 for their time and transportation costs.
Measures
Racial identification (T1)
RI was assessed using seven items from the Affirmation/Belonging subscale and the Behavior subscale of the Multigroup Ethnic Identity Measure (Phinney, 1992; e.g., “You have a strong attachment toward your ethnic group” and “You feel good about your ethnic background”; 1 = strongly disagree to 4 = strongly agree; α = .74).
Willingness (T2)
Willingness to use drugs was measured with three items worded as in previous studies (e.g., Gibbons et al., 2004). The section began with a description of a hypothetical scenario: “Suppose you were at a friend’s apartment and there were some drugs there that you could have if you wanted.” This statement was followed by two light and one heavier use questions (e.g., “How willing would you be to … try some of the drugs? … use enough to get high? … buy some to use later?”; 1 = not at all to 7 = very; α = .85).
Scenario substance use risk (T2)
The indirect measure of use cognitions was assessed by coding the open-ended responses to the party scenario described above. A point was added if the participant mentioned alcohol or drug use by either themselves or guests. Thus, responses could range from 0 to 4. Agreement between two independent coders (blind to condition) was high: intraclass correlation = .99.
Control Variables
Supportive parenting (T1)
Responses from the adolescents and parents were combined to create the parenting measure. Adolescents completed a nine-item measure of perceived parental warmth (e.g., “How often during the past 12 months did (parent) tell you she loves you?”) plus two communication items. Parents completed a six-item measure of consistent discipline. Parents and adolescents both responded to seven questions about the parents’ inductive reasoning and their use of problem solving (all scales from 1 = never to 4 = always; combined α = .85; Gibbons et al., 2010).
Self-concept (T1)
Adolescents rated themselves on the following adjectives: popular, smart, cool, and good-looking (1 = not at all to 4 = very; α = .64).
Perceived stress (T2)
After imagining the scenario, participants were asked how stressful that situation would be for them (1 = not at all to 4 = very).
Drug use (T2)
Participants were asked how often they had used marijuana, crack or cocaine, and other illegal drugs in the past 6 months (3 items averaged; 1 = not at all to 4 = a lot).
Results
Descriptive statistics, correlations, and ANOVAs
Table 1 presents the means, SDs, and zero-order correlations for all variables. The vast majority (95%) of participants reported using marijuana; 16% reported using one other illegal drug. Substance use in the party scenario was mentioned by 60% of the participants, with 40% reporting use of more than one substance. When asked if an event similar to the one in the scenario had ever happened to them, 43% in the discrimination condition said yes, 47% in the stress condition said yes, and 50% in the nonstress condition said yes.
Table 1.
Means, Standard Deviations, and Correlations for Indices in Study 1
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1 T1 racial identity | — | |||||||
| 2 T2 substance willingness | −.26* | — | ||||||
| 3 T2 scenario substance use | −.08 | .19 | — | |||||
| 4 T1 supportive parenting | .16 | −.11 | −.06 | — | ||||
| 5 T1 self-concept | .04 | .05 | −.05 | .06 | — | |||
| 6 T2 perceived stress | .09 | .17 | .20 | −.17 | .06 | — | ||
| 7 T2 drug use | −.16 | .50** | .23† | −.18 | −.05 | .10 | — | |
| 8 gender | −.08 | −.23† | −.33* | −.09 | −.09 | .04 | −.22† | — |
| M | 3.47 | 2.49 | 0.95 | 3.02 | 3.22 | 2.68 | 1.66 | — |
| SD | 0.51 | 1.35 | 1.10 | 0.48 | 0.47 | 0.92 | 0.35 | — |
| Range | 1–4 | 1–7 | 0–4 | 1–4 | 1–4 | 1–4 | 1.3–3 | — |
N = 64. For gender, 0 = male, 1 = female. All other variables coded such that high scores indicate more of the construct.
p ≤ .10.
p ≤ .05.
p ≤ .01.
An ANOVA performed on RI and past use revealed no significant condition effects, indicating no randomization problems (ps > .15). An ANCOVA (controlling for gender, past use, RI, self-concept, and parenting) performed on perceived stress revealed a main effect of Condition: F(2,63) = 6.53, p = .003. As expected, the mean in the Discrimination condition (M = 3.23) was significantly higher than that in either the Control condition (M = 2.20, p = .002) or the Stress condition (M = 2.59, p < .05); and the Stress condition was higher than the Control (p = .05). Because we were interested in the effects of discrimination (and RI), and not stress, all subsequent analyses controlled for this measure.
RI as a protective factor
Hierarchical multiple regression analyses were used to examine the hypothesized RI × Condition interactions on drug willingness and scenario-based risk. RI was centered for all interactions. Two orthogonal contrasts were created for the condition variable. Because it was hypothesized that the discrimination condition would differ from both the stress and control conditions (Gibbons et al., 2010), the first contrast compared the discrimination condition with the stress and control condition (Contrast D-SC; −2, 1, 1). The second contrast compared the stress condition with the control condition (Contrast S-C; 0, 1, −1; West, Aiken, & Krull, 1996).
Willingness
A significant main effect was found for past drug use: Those who reported past use reported higher willingness (β = .42, p < .001). The main effect for RI was marginal (β = −.24, p < .06), as participants with higher levels of RI tended to report lower willingness. Parenting, self-concept, perceived stress, and gender were all nonsignificant. The S-C contrast and S-C contrast × RI interaction were also not significant (ps > .4), indicating that the stress and control conditions did not differ. The predicted main effect of the D-SC contrast was significant (β = −.32, p < .04), as those in the discrimination condition reported higher levels of willingness than those in the control and stress conditions. The anticipated D-SC × RI interaction was significant (β = −.34, p < .01; see Figure 1).3 Simple slopes revealed that among participants in the discrimination condition, lower RI (mean RI levels +1/−1 SD) was associated with higher levels of willingness (β = −.43, p < .04). Among participants in the nondiscrimination conditions, however, the relationship was nonsignificant (p > .7).
Figure 1.

Willingness to use drugs as a function of condition (discrimination vs. nondiscrimination) and racial identity (RI) level (±1 SD) among past drug users (Study 1)
Scenario-based risk
Reports of substance use were not significantly correlated with willingness (r = .19, p > .1). However, because it was measured first, we controlled for willingness in the following regressions. A significant main effect for gender indicated that males reported higher levels of risk (β = −.29, p < .03). None of the other control variables was a significant predictor of scenario-based risk. The S-C contrast was not significant (p > .2), indicating that, once again, the stress and control conditions did not differ. The predicted main effect was found for the D-SC contrast: Participants in the discrimination condition were more likely to report substance use at the party (β = −.33, p < .02). A D-SC × RI interaction revealed the same pattern found with willingness: Participants in the discrimination condition who had lower RI levels reported the highest levels of scenario-based risk (β = .34, p < .04; see Figure 2). Among participants in the discrimination condition, RI was associated with lower levels of risk (β = .43, p < .04). Among participants in the nondiscrimination conditions, however, the relationship was nonsignificant (p > .4).
Figure 2.

Scenario-based substance use risk as a function of condition (discrimination vs. nondiscrimination) and racial identity (RI) level (±1 SD) among past drug users (Study 1)
Discussion
Results from this study add to those in Gibbons et al. (2010) by providing evidence that RI can serve as a buffer against the negative impact of discrimination on drug use vulnerability among drug users. Black young adult users who envisioned themselves in a racial discrimination scenario were more likely to report willingness to use drugs and higher levels of substance use cognitions on a more indirect (spontaneous) measure than those who did not imagine a discrimination experience. Importantly, these findings were moderated by RI, such that those with lower RI were more likely to think about drug use when faced with discrimination. Thus, our findings indicate that individual differences in RI can help explain within-group variability among Black young adults in reactions to discrimination.
The first study used a lab-based discrimination scenario to demonstrate the protective effects of RI on substance use vulnerability among Black young adults and showed these effects on both an explicit and an indirect measure of substance vulnerability. However, although discrimination was manipulated, participants did not face a discriminatory experience, and RI was not manipulated. This raises additional important questions that Study 2 was designed to answer: (a) Can the results be replicated when Black young adults experience (vs. imagine) race-based discrimination? and (b) Can the protective effects of RI be demonstrated experimentally, via a RI manipulation? In short, to understand the quality of RI as a protective factor, it is important to manipulate RI salience.
Experiment 2
Discrimination, Social Exclusion, and Cyberball
A common form of discrimination that is often faced by minorities is being socially excluded (Smart Richman & Leary, 2009; K. D. Williams & Carter-Sowell, 2009). An effective way of manipulating social exclusion is via Cyberball, which is a computer ball-tossing game in which participants are excluded or included by other “players” (in actuality, there are no players and the tosses are preprogrammed; K. D. Williams, Cheung, & Choi, 2000). Research employing Cyberball has revealed that social exclusion is associated with lower levels of perceived belonging (K. D. Williams & Carter-Sowell, 2009), especially when participants are excluded by members of an out-group (K. D. Williams et al., 2000). Using Cyberball, Wirth and Williams (2009) found that participants who were excluded by “players” of a different gender were more likely to attribute this exclusion to gender-based discrimination and reported more negative moods than did those who did not have group status (i.e., gender) made salient (by showing the players’ gender). A recent study also demonstrated that Cyberball is an effective way to examine racial discrimination effects (Goodwin, Williams, & Carter-Sowell, 2010). In this study, Black and White participants were excluded by members of their own or the other race. Blacks attributed their exclusion (by Blacks and Whites) to racism, and this attribution impeded psychological recovery time, particularly when the other players were White. Previous research, using a different exclusion paradigm, found that when Black students were rejected by a White confederate, this rejection was attributed to prejudicial attitudes when the confederate knew they were Black (Crocker, Voelkl, Testa, & Major, 1991). However, previous studies have not examined the effects of exclusion, including racial exclusion, on substance-related cognitions.
RI Affirmation
RI tends to be relatively stable for young adults, but its salience can be influenced by the social situation (Yip, 2007). For example, Shelton and Sellers (2000) found that racial centrality scores were higher among Black young adults who watched a video in which a Black male was attacked by a White male while in a room with three White confederates, compared to those in a room with Black confederates or those who watched a video of a White male being assaulted by another White male. In addition, interventions that include an Africentric approach (e.g., an Africentric education course) have found RI levels to be higher among adolescents in the intervention versus control group (Belgrave, Reed, Plybon, & Corneille, 2004; Cherry et al., 1998), demonstrating that RI is mutable.
One way to examine the impact of RI salience is through the process of affirmation (writing about an important value or life domain). Self-affirmation has been shown to decrease negative reactions to psychological threats to the self (or one’s social/racial group) and protect self-worth (Sherman & Cohen, 2006). For example, it has been shown to reduce the negative effects of stereotype threat on the math performance of female college students (Steele, Spencer, & Aronson, 2002). One prominent aspect of the self for minorities that is connected to positive feelings of self-worth is racial group membership (Phinney, Cantu, & Kurtz, 1997). Given that self-affirmation is associated with more positive feelings about the self in situations involving threat (see Sherman & Cohen, 2006, for a review), we reasoned that these effects should generalize to RI affirmation in situations that include self-threats based on race. Therefore, Study 2 examined whether self-affirmation involving RI can mitigate the negative effects of discrimination on substance use vulnerability. We hypothesized that social exclusion of Blacks by Whites would be attributed to racial discrimination and associated with greater substance use vulnerability among those who do not affirm their RI.
Method
Participants
Participants were recruited through advertisements around the Washington, D.C., metro area. They were told we were examining the relations among RI, health, emotions, and the social environment. Out of approximately 230 responses to the ads, 206 young adults (114 females; M age = 21.5, SD = 1.9) met the criteria for participation (African American, ages 18 to 25). A total of 4 participants were excluded because of high levels of suspicion, 2 did not follow directions, and 1 was unable to complete the study. Of the remaining 199 participants, 22% reported no substance use behaviors in the past 6 months. Because of previous research findings that manipulated discrimination predicts risk cognitions only among substance users (Gibbons et al., 2010), Study 2 focused on the 155 young adults (91 females) who had used substances.
Procedure
Basic demographic questions, RI, and substance use (alcohol and drugs) over the past 6 months were assessed by phone (T1). In the lab (T2), participants were told they would first play an online ball-tossing game. The game was a modified version of Cyberball (similar to Goodwin et al., 2010). Participants were led to believe that the other “players” were three White same-sex 18- to 25-year-olds and were randomly assigned to the exclusion or inclusion conditions. In the exclusion condition (n = 75), participants received the ball three times and then were excluded for the rest of the game. In the inclusion condition (n = 80), the participant and each “player” received the ball 25% of the time. The game lasted approximately 3 minutes. Following the game, mood and manipulation checks were assessed.
Participants were then randomly assigned to either the RI affirmation condition (n = 77) or the control condition (n = 78). RI affirmation participants were asked to “… think about what it means to you to be an African American. For example, how is being connected to other members of your racial group important to who you are, how you feel about yourself, and your values?” Participants in the control condition wrote about what they did over the past 24 hours (cf. Sherman & Cohen, 2006). The writing task was followed by measures of willingness to use alcohol and drugs and then the same scenario-based risk measure used in Study 1. Manipulation check items and a self-esteem scale were also included postmanipulation. Finally, participants were debriefed and paid $40 for their time.
Measures
Previous use (T1)
Participants were asked how often they had drunk a lot or used marijuana, crack or cocaine, and other illegal drugs in the past 6 months (1 = never to 7 = more than 8 times; α = .69).
Manipulation checks (T2)
Following the Cyberball game, participants were asked how much they felt they belonged to the group (1 = not at all, 7 = very much) and how included they were (1 = totally excluded, 7 = totally included). These two items comprised the belonging manipulation check (α = .89). To examine if the Cyberball manipulation resulted in feelings of perceived discrimination, participants were asked, “To what extent do you feel your inclusion or exclusion was due to your race” (1 = not at all, 7 = very much), and a more direct item at the end of the study asked, “To what extent do you feel you were being discriminated against based on your race?” (1 = not at all, 7 = very much; α = .77). Participants were also asked to what extent they believed their inclusion/exclusion was the result of their gender, age (1 = not at all, 7 = very much), or other reasons (open ended).
Willingness (T2)
The drug scenario was the same one used in Study 1. The alcohol scenario began, “Suppose that you are at a party. After several drinks, you begin to feel that you may have had enough… .” This statement was followed by one lighter and one heavier use question (e.g., “How willing would you be to stay and … have a few more drinks? … continue to drink more than a few drinks?”), each accompanied by a 7-point scale from not at all to very (e.g., Gibbons et al., 2004). These four items were combined (α = .82).
Scenario substance use risk (T2)
Scenario-based substance use risk was measured the same way as in Study 1. Agreement between two independent coders (blind to condition) was high: intraclass correlation = .98.
Control variables
All analyses controlled for gender. In addition, self-reported RI (T1) was used as a control variable. Five items from Phinney’s (1992) affirmation and belonging scales (Study 1) were modified slightly. Instead of using the term ethnic, the items referred to Black or racial identity (1 = strongly disagree to 7 = strongly agree; a = .79). Self-esteem (T2) was assessed by averaging five items from the Rosenberg Self-Esteem Scale (Rosenberg, 1965; α = .67).
Results
Descriptive statistics, correlations, and ANCOVAs
Table 2 presents the means, SDs, and zero-order correlations (by Exclusion condition) for all variables. Most of the participants (75%) reported drinking a lot; 50% reported using marijuana; 14% reported using at least one other illegal drug. An Exclusion (no/yes) by RI Affirmation (no/yes) ANOVA performed on past use revealed no significant condition or interaction effects, indicating there were no randomization problems (all ps > .13).
Table 2.
Means, Standard Deviations, and Correlations for Indices in Study 2
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 Gender | — | |||||||||
| 2 RI affirmation | .04 | — | ||||||||
| 3 Exclusion | .02 | .00 | — | |||||||
| 4 Belonging | −.11 | −.05 | −.67*** | — | ||||||
| 5 Perceived discrimination | .09 | −.01 | .54*** | −.62*** | — | |||||
| 6 Substance use | −.09 | .07 | −.12 | −.00 | −.05 | — | ||||
| 7 RI | .00 | .04 | −.01 | .05 | .02 | .01 | — | |||
| 8 Substance willingness | −.04 | −.12 | .14 | −.08 | .09 | .59*** | −.10 | — | ||
| 9 Scenario substance use | −.01 | −.05 | .07 | −.04 | .02 | .37** | −.04 | .40*** | — | |
| 10 Self-esteem | .01 | .07 | −.06 | .15* | −.05 | −.09 | .17* | −.08 | −.05 | — |
| M | — | — | — | 3.4 | 3.26 | 2.61 | 5.50 | 2.41 | 1.40 | 5.57 |
| SD | — | — | — | 1.5 | 1.63 | 1.37 | 1.03 | 1.33 | 1.04 | 1.27 |
| Range | — | — | — | 1–7 | 1–7 | 1–7 | 2–7 | 1–7 | 0–4 | 1–7 |
N = 155. For racial identity (RI) affirmation, 0 = no, 1 = yes. For exclusion, 0 = included, 1 = excluded. All other variables coded such that high scores indicate more of the construct.
p ≤ .05.
p ≤ .01.
p ≤ .001.
An Exclusion by Affirmation general linear model ANCOVA on belonging (controlling for gender, self-esteem, and RI) revealed a main effect for Exclusion, as excluded participants reported lower levels of belonging, F(1, 154) = 146.67, p < .001. The Exclusion by Affirmation interaction was also significant, F(1, 154) = 6.50, p = .01; the lowest levels of belonging were reported by the nonaffirmed, excluded participants. An Exclusion main effect was also found for perceived discrimination: Excluded participants reported much higher levels of perceived discrimination than included participants, F(1, 154) = 55.54, p < .001. Moreover, all but two of the excluded participants reported the reason was their race (i.e., they had higher means on the question about race versus gender, age, or other reasons).4 Finally, the Exclusion by Affirmation interaction on perceived discrimination was nonsignificant (p > .5).
RI, racial exclusion, and past use: Willingness
Hierarchical multiple regression analyses were used to examine the effects of Affirmation and Exclusion on substance willingness. For all interactions, the continuous variables were centered. Main effects were found for past use and exclusion: Users and excluded participants reported higher levels of willingness (βs = .59 and .17, ps < .01). An Exclusion × Affirmation interaction revealed a similar pattern to Study 1 in that the nonaffirmed, excluded group reported the highest levels of willingness (β = −.28, p < .01).5 In addition, a significant Use × Exclusion interaction revealed that excluded participants reporting higher levels of previous use, reported the highest levels of willingness (β = −.25, p < .03). The two-way interactions were qualified by the anticipated Use × Affirmation × Exclusion interaction (β = −.26, p < .01): High users in the Exclusion, non-RI affirmation condition reported the highest willingness, whereas the lowest levels were reported by low users in the included condition with RI affirmation.6 No other significant effects were found.
To further examine the three-way interaction, the Use × Affirmation interactions were examined separately for the included versus excluded participants. Among the included participants, past use was a significant predictor of willingness (β = .54, p < .001); however, the Use by Affirmation interaction was not significant (p = .38). For the excluded participants, significant Use and Affirmation condition main effects (βs = .39, −.27, ps ≤ .01) revealed that higher levels of use and not engaging in the RI affirmation writing task were associated with higher levels of willingness. In addition, a significant Use by Affirmation interaction (β = −.43, p < .01; see Figure 3) revealed that the highest levels of willingness were among high users who did not engage in RI affirmation. Simple slopes revealed that among the high users (+1 SD), RI Affirmation was associated with lower willingness (β = −.45, p = .02). Among the low users (−1 SD), however, the relationship was nonsignificant (p > .8).
Figure 3.
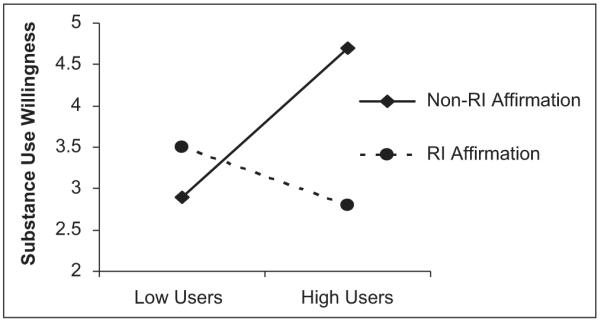
Willingness to use substances as a function of level of use (±1 SD) and racial identity (RI) affirmation (no vs. yes) among the excluded (discriminated) participants (Study 2)
Because being excluded was associated with perceptions of discrimination, an internal analysis that substituted participants’ self-reports of discrimination for exclusion condition was also conducted. When the Exclusion condition was replaced in the regression with perceived discrimination as a predictor, the Affirmation × Perceived Discrimination and the three-way interaction remained significant (βs = −.25, p < .04; −.78, p < .001) and revealed the same patterns as above: High users who reported the highest levels of perceived discrimination and did not affirm their RI reported the highest levels of willingness.
RI, racial exclusion, and past use: Scenario substance use risk
Self or other substance use in the party scenario was mentioned by 84% of the participants. This measure was correlated with willingness but not redundant (r = .40, p < .001). As in Study 1, because willingness was measured first, it was included as a control variable. Participants who reported high levels of past use also reported higher scenario risk (β = .31, p < .01). The Exclusion × Affirmation interaction (β = −.29, p = .02) revealed the highest risk was reported by those without RI affirmation in the excluded condition, whereas participants in the affirmed, excluded condition reported the lowest. A significant Use × Exclusion interaction (β = .40; p < .04) indicated that participants with higher levels of past use, in the exclusion condition, reported the highest levels of risk. The interaction was qualified by the Use × Affirmation × Exclusion interaction (β = −.52, p < .02), revealing that high users in the Exclusion, non-RI affirmation condition reported the highest risk, whereas the lowest levels were reported by low users in the included, RI Affirmation condition.
Further examination of the three-way interaction revealed that the Use × Affirmation interaction was significant for excluded participants (β = −.43, p < .02; see Figure 4) but not included participants (p = .28). Among the excluded participants, higher levels of past use and being in the nonaffirmed condition were significant predictors of risk (βs = .61, −.22, ps < .03, respectively), but these main effects were not significant among the included participants. As with willingness, RI Affirmation was associated with lower risk among high users (β = −.58, p < .01), but not among low users (p > .3). Finally, when the Exclusion condition was replaced in the regression with perceived discrimination, the Affirmation × Perceived Discrimination interaction and the three-way interaction with use were significant (βs = −.32, −.54, ps < .04) and revealed the same patterns: The highest levels of risk were reported by high users who did not affirm and who reported higher levels of perceived discrimination.
Figure 4.

Scenario-based substance use risk as a function of level of use (±1 SD) and racial identity (RI) affirmation (yes vs. no) among the excluded (discriminated) participants (Study 2)
Discussion
Study 2 demonstrated that Cyberball is an effective way to examine the impact of racial discrimination on risk cognitions in a lab-based setting. The vast majority of the Black young adults who were excluded attributed this discrimination to their race and, as in Study 1, were more likely to report substance use vulnerability, especially if they did not engage in RI affirmation. Also, consistent with previous research, we found that attributing exclusion to prejudice does have negative effects and that RI can buffer these effects (Branscombe et al., 1999; Schmitt & Branscombe, 2002). Finally, the effects of RI Affirmation and Exclusion were the same when the exclusion condition was replaced with perceptions of discrimination, indicating that the attributions of discrimination are important and it is not just being excluded that has a negative effect.
There was evidence that experimentally affirming RI can counteract the effect of racial discrimination on substance use vulnerability. More specifically, results indicated that RI salience is malleable, interacts with the situation, and, in turn, has an impact on subsequent risk cognitions. In other words, not only is dispositional RI protective (Study 1), but having Black young adults affirm the importance of their racial group after experiencing discrimination is also protective, even when controlling for self-reported RI and self-esteem. Thus, this study supports a basic tenet of self-affirmation theory: Affirming an important value can protect against perceived threat (Sherman & Cohen, 2006), a process that may enhance positive thoughts in dealing with experiences of discrimination.
Expanding on conceptual models in social psychology on rejection, we demonstrated that social exclusion (via Cyberball) is associated with negative physical health (substance use) cognitions. It is likely that our participants perceived their exclusion to be unfair as there was no explicit reason for it, and perceived unfairness because of rejection is associated with anger and antisocial responses (Smart Richman & Leary, 2009). However, RI affirmation may help reduce anger and restore feelings of support, which reduces the likelihood of negative health outcomes.7
General Discussion
Social scientists have found evidence among Blacks of a relation between perceived racial discrimination and health risk behaviors (Pascoe & Smart Richman, 2009; D. R. Williams & Mohammed, 2009). In addition, some studies have found RI to be protective against the negative effects of discrimination on mental and, in some instances, physical health (Branscombe et al., 1999; Sellers et al., 2003; D. R. Williams et al., 1999). These current studies provide experimental evidence that RI is protective against substance use risk among Black young adults following a discrimination experience. The pattern of results was consistent: Discrimination, whether manipulated via imagining a discrimination scenario or via social exclusion during an interactive game, was associated with higher levels of substance use risk cognitions. However, RI, both self-reported and affirmed, was protective against this relation among substance users. Moreover, the results demonstrated these protective effects on two distinct measures of substance vulnerability.
RI as a Protective Factor
RI and substance use
Our findings are consistent with research on the general protective influence of RI on substance use attitudes and problem behaviors (Belgrave et al., 2000; Brook, Balka, Brook, Win, & Gursen, 1998; Pugh & Bry, 2007) and with research indicating that as RI increases, perceived discrimination has less of an impact on African Americans’ well-being (Greene et al., 2006; Wong et al., 2003). Although our studies did not examine mediators of the relation between RI and risk cognitions, we believe there are several possible reasons why RI buffers against substance vulnerability, including the positive association between RI and positive feelings about the self as a minority (Phinney et al., 1997; Sellers et al., 2003). RI is also associated with endorsement of Black cultural norms, which emphasize bonds with one’s family and racial group and, in turn, enhance feelings of belonging and social support (Boyd-Franklin, 2003; Phinney, 1990). Black cultural norms are associated with a set of substance use beliefs that protect Black children from early use (Johnson & Johnson, 1999). In addition, it may be the case that Blacks, especially when RI is salient, are motivated to debunk stereotypes of Blacks as users while embracing a positive identification (Pugh & Bry, 2007). In short, Black young adults whose level of RI is high or made salient appear to be less negatively affected by racial discrimination.
RI affirmation
To enhance RI salience, the Black young adults in Study 2 engaged in a racial-identity affirmation task. The majority of previous studies in self-affirmation theory have had participants choose a value to rank or write on a domain unrelated to the one being threatened (Sherman & Cohen, 2006). Our results demonstrate that affirmations based within the same (vs. different) domain that is being threatened can be protective in some situations. In addition, we found that having all participants affirm the same value can be effective against self-threats that cannot be changed (e.g., race) and against the negative effects of exclusion by other racial groups.
RI and Discrimination
The results have implications for research on RI, social exclusion, and discrimination and suggest a number of future studies. First, there is some debate in the literature about the direction of the relation between discrimination and RI. Experiencing discrimination has been shown to lead to greater affiliation with one’s ethnic group (Branscombe et al., 1999; Sellers et al., 2003). However, some have suggested that a high level of RI may also lead to a tendency to perceive more discrimination (Hall & Carter, 2006; Sellers et al., 2006). In addition, researchers have suggested that discrimination may have a more negative impact among those who report their group is more central to their identity (e.g., Major, Quinton, & Schmader, 2003). This was not the case in the current studies. These discrepancies may reflect study design and differences in measures of RI. For example, research suggests that RI only enhances sensitivity to perceptions of discrimination in attributionally ambiguous situations (Major et al., 2003). Our studies examined RI in situations where experiences of discrimination were not ambiguous and where participants were discriminated against by a group versus one person.
RI constructs
There is some evidence that feelings of belonging and connections to one’s racial group may be more likely than other RI measures, such as racial centrality, to act as a buffer (e.g., Burrow & Ong, 2010; Greene et al., 2006). Phinney’s measure of affirmation and belonging has been shown to be a reliable measure of in-group identification and to buffer the impact of discrimination on well-being (e.g., Branscombe et al., 1999). However, some researchers view RI as a multidimensional construct (Phinney, 1996; Sellers et al., 2003). We are currently using the Multidimensional Inventory of Black Identity to examine if some dimensions of RI are more protective against risky health behaviors than others (Sellers et al., 1998).
We have also found that among Black adolescents, RI is more protective against substance use in integrated environments, where perceived discrimination is higher. Future research should examine whether young adults with low RI and those in more integrated environments are at higher risk when they are more assimilated into the mainstream and/or when they experience greater levels of discrimination. It is also important to identify the potential of RI to moderate the relations among risk factors and risk cognitions, either through buffering against psychological or social risks or by enhancing promotive factors, such as academic orientation (Brook et al., 1998). Additional research that combines lab and longitudinal studies is needed to more fully examine the relation among different forms of racial discrimination, different components of RI, and health outcomes among Blacks and other minority groups.
Cyberball
Work by Williams and colleagues has shown that exclusion by one’s in-group can also produce psychological distress and perceptions of discrimination (Goodwin et al., 2010; K. D. Williams & Carter-Sowell, 2009). However, research has also shown that Blacks are more likely to attribute (written) rejection by Whites (vs. Blacks) to discrimination (Mendes, Major, McCoy, & Blascovich, 2008). Our current research suggests that same-race exclusion is associated with distress and substance-related cognitions, but at a lower level compared to exclusion by another race. It is not known, however, if same-race exclusion would also be moderated by RI. Additional studies should also assess reflexive needs (immediate feelings of distress or pain; Goodwin et al., 2010) as potential mediators of the link between racial exclusion and risk cognitions.
Intervention Implications
The current results illustrate the potential importance of ethnic-based approaches to minority substance use prevention. Promoting RI might reduce risk factors for drug use and enhance the effects of protective factors (Brook et al., 1998). Substance prevention programs, such as SAAF, which encourage Black adolescents to be proud of their race, in part, because Black adolescents use substances less, can increase negative attitudes toward use and also decrease willingness and use (Brody et al., 2004; Gerrard et al., 2006). In addition, preventive interventions aimed at helping Black parents prepare their children for difficulties they may face because of discrimination, while enhancing RI may help buffer the negative impact of discrimination on health (Brody et al., 2004; Fischer & Shaw, 1999).
Although the impact of exclusion on psychological well-being is fairly well established (Smart Richman & Leary, 2009), our findings suggest that social exclusion can also have potentially negative effects on the physical well-being of young adults. The findings that RI affirmation is protective against these negative effects implies that enhancing and discussing group-based identification can help reduce the pain and potential negative health consequences because of rejection from the majority (Brondolo et al., 2009; Schmitt & Branscombe, 2002). Finally, our results imply that having everyone affirm the same value may be an effective, and potentially more feasible and realistic strategy, to use in future prevention and intervention efforts among those who share a common value or the same group identity.
Limitations
There are limitations to the current studies that should be acknowledged. First, discriminatory experiences outside the lab may produce different reactions than they did in Study 2. Thus, it is unclear how strong the protective effects of RI would be in these situations. In addition, in Study 1, no significant differences in willingness were found between the nonstress and stress conditions. Thus, we do not know how a more stressful scenario would compare to the stress of a discrimination scenario. Finally, our data do not allow us to conclude if RI affirmation was protective via increasing levels of RI, making RI salient, or enhancing positive feelings about the self and one’s racial group. Future research should examine the process by which RI is protective when experiencing discrimination.
Conclusion
Results across two studies provide experimental evidence that racial discrimination can have an important impact on the substance use vulnerability of Black young adult substance users. In addition, these results demonstrate that both self-reported and affirmed RI can be protective against explicit and more indirect measures of substance use cognitions, after experiencing racial discrimination. This is important for several reasons, including the fact that Blacks appear to suffer more negative consequences of substance use than do adults of other races, and these negative consequences may have a long-term impact on their health (e.g., French et al., 2002). Finally, these findings have implications for future interventions and demonstrate the importance of examining the interaction of individual and social factors.
Acknowledgments
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: This research was supported by National Institute of Drug Abuse Grants DA018871-05 and DA021898.
Notes
It was not possible to determine if all 175 received the recruitment letter as this was a very mobile population.
There were no main effects or interactions on willingness to help others.
The two-way interactions were also significant when the discrimination condition was compared to just the control or just the stress condition. When the nonusers are included in the regressions, there is a significant previous Drug Use × RI × D-SC interaction on willingness to use drugs (β = −.31, p < .02) and on the scenario-based risk measure (β = −.26, p < .04). The D-SC × RI interactions were not significant for nonusers (ps > .40).
Results do not change when these 2 participants are excluded.
We also included measures of sadness, happiness, and anger. A significant exclusion effect was found only on anger. An Exclusion × RI affirmation interaction (p < .03) revealed the highest level of anger was reported by those without RI affirmation in the excluded condition; moreover, the exclusion main effect on anger was significant only among the nonaffirmed participants (p = .002). For this group, anger mediated the relation between exclusion and willingness (Sobel t = 2.10, p < .05; cf. Gibbons et al., 2010). These results are interesting but beyond the scope of this article.
When the nonusers were included in the regressions, the three-way interaction remained significant on willingness (β = −.26, p < .01) and on the scenario-based risk measure (β = −.49, p < .04).
See Note 5.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Belgrave FZ, Brome DR, Hampton C. The contribution of Africentric values and racial identity to the prediction of drug knowledge, attitudes, and use among African American youth. Journal of Black Psychology. 2000;26:386–401. [Google Scholar]
- Belgrave FZ, Reed MC, Plybon LE, Corneille M. The impact of a culturally enhanced drug prevention program on drug and alcohol refusal efficacy among urban African American girls. Journal of Drug Education. 2004;34:267–279. doi: 10.2190/H40Y-D098-GCFA-EL74. [DOI] [PubMed] [Google Scholar]
- Borrell LN, Jacobs DR, Williams DR, Pletcher MJ, Houston TK, Kiefe CI. Self-reported racial discrimination and substance use in the Coronary Artery Risk Development in Adults study. American Journal of Epidemiology. 2007;166:1068–1079. doi: 10.1093/aje/kwm180. [DOI] [PubMed] [Google Scholar]
- Boyd-Franklin N. Black families in therapy: An African-American experience. 2nd ed Guilford; New York, NY: 2003. [Google Scholar]
- Branscombe NR, Schmitt MT, Harvey RD. Perceiving pervasive discrimination among African-Americans: Implications for group identification and well-being. Journal of Personality and Social Psychology. 1999;77:135–149. [Google Scholar]
- Brody GH, Ge X, Conger R, Gibbons FX, Murry VM, Gerrard M, Simons RL. The influence of neighborhood disadvantage, collective socialization, and parenting on African American children’s affiliation with deviant peers. Child Development. 2001;72:1231–1246. doi: 10.1111/1467-8624.00344. [DOI] [PubMed] [Google Scholar]
- Brody GH, Murry VM, Gerrard M, Gibbons FX, Molgaard V, McNair L, Newbaum-Carlan E. The Strong African Americans Families Program: Translating research into prevention programming. Child Development. 2004;75:900–917. doi: 10.1111/j.1467-8624.2004.00713.x. [DOI] [PubMed] [Google Scholar]
- Brondolo E, ver Halen NB, Pencille M, Beatty D, Contrada RJ. Coping with racism: A selective review of the literature and a theoretical and methodological critique. Journal of Behavioral Medicine. 2009;32:64–88. doi: 10.1007/s10865-008-9193-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brook JS, Balka EB, Brook DW, Win PE, Gursen MD. Drug use among African Americans: Ethnic identity as a protective factor. Psychological Reports. 1998;83:1427–1446. doi: 10.2466/pr0.1998.83.3f.1427. [DOI] [PubMed] [Google Scholar]
- Brook J, Pahl K. The protective role of ethnic and racial identity and aspects of an Africentric orientation against drug use among African American young adults. Journal of Genetic Psychology. 2005;166:329–345. doi: 10.3200/GNTP.166.3.329-345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burrow AL, Ong AD. Racial identity as a moderator of daily exposure and reactivity to racial discrimination. Self and Identity. 2010;9:383–402. [Google Scholar]
- Chae DH, Takeuchi DT, Barbeau EM, Bennet GG, Lindsey J, Krieger N. Unfair treatment, racial/ethnic discrimination, ethnic identification and smoking among Asian Americans in the National Latino and Asian American Study. American Journal of Public Health. 2008;98:485–529. doi: 10.2105/AJPH.2006.102012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cherry VR, Belgrave FZ, Jones W, Kennon DK, Gray FS, Phillips F. NTU: An Africentric approach to substance abuse prevention among African American youth. Journal of Primary Prevention. 1998;18:319–339. [Google Scholar]
- Crocker J, Voelkl K, Testa M, Major B. Social stigma: The affective consequences of attributional ambiguity. Journal of Personality and Social Psychology. 1991;60:218–228. doi: 10.1037//0022-3514.64.1.60. [DOI] [PubMed] [Google Scholar]
- Cross WE., Jr. Shades of black: Diversity in African-American identity. Temple University Press; Philadelphia, PA: 1991. [Google Scholar]
- Fischer AR, Shaw CM. African Americans’ mental health and perceptions of racist discrimination: The moderating effects of racial socialization experiences and self-esteem. Journal of Counseling Psychology. 1999;46:395–407. [Google Scholar]
- French K, Finkbiner R, Duhamel L. Patterns of substance use among minority youth and adults in the United States: An overview and synthesis of national survey findings. Caliber; Fairfax, VA: 2002. [Google Scholar]
- Gerrard M, Gibbons FX, Brody GH, Murry VM, Cleveland MJ, Wills TA. A theory-based dual focus alcohol intervention for pre-adolescents: The Strong African American Families Program. Psychology of Addictive Behavior. 2006;20:185–195. doi: 10.1037/0893-164X.20.2.185. [DOI] [PubMed] [Google Scholar]
- Gerrard M, Gibbons FX, Houlihan AE, Stock ML, Pomery EA. A dual-process approach to health risk decision making: The prototype willingness model. Developmental Review. 2008;28:29–61. [Google Scholar]
- Gerrard M, Gibbons FX, Stock ML, Vande Lune LS, Cleveland MJ. Images of smokers and willingness to smoke among African American pre-adolescents: An application of the prototype/willingness model of adolescent health risk behavior to smoking initiation. Pediatric Psychology. 2005;30:305–318. doi: 10.1093/jpepsy/jsi026. [DOI] [PubMed] [Google Scholar]
- Gibbons FX, Etcheverry PE, Stock ML, Gerrard M, Weng C, O’Hara R. Exploring the link between racial discrimination and substance use: What mediates and what buffers? Journal of Personality and Social Psychology. 2010;99:785–801. doi: 10.1037/a0019880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibbons FX, Gerrard M, Cleveland M, Wills TA, Brody GH. Perceived discrimination and substance use in African American parents and their children: A panel study. Journal of Personality and Social Psychology. 2004;86:517–529. doi: 10.1037/0022-3514.86.4.517. [DOI] [PubMed] [Google Scholar]
- Gibbons FX, Gerrard M, Lane DJ. A social reaction model of adolescent health risk. In: Suls JM, Wallston K, editors. Social psychological foundations of health and illness. Blackwell; Oxford, UK: 2003. pp. 107–136. [Google Scholar]
- Gibbons FX, Yeh H, Gerrard M, Cleveland MJ, Cutrona C, Simons RL, Brody GH. Early experience with discrimination and conduct disorder as predictors of subsequent drug use: A critical period analysis. Drug and Alcohol Dependence. 2007;88:27–37. doi: 10.1016/j.drugalcdep.2006.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goodwin SA, Williams KD, Carter-Sowell AR. The psychological sting of stigma: The costs of attributing ostracism to racism. Journal of Experimental Social Psychology. 2010;46:612–618. [Google Scholar]
- Greene ML, Way N, Pahl K. Trajectories of perceived adult and peer discrimination among Black, Latino, and Asian American adolescents: Patterns and psychological correlates. Developmental Psychology. 2006;42:218–238. doi: 10.1037/0012-1649.42.2.218. [DOI] [PubMed] [Google Scholar]
- Hall SP, Carter RT. The relationship between racial identity, ethnic identity, and perceptions of racial discrimination in an Afro-Caribbean descent sample. Journal of Black Psychology. 2006;32:155–175. [Google Scholar]
- Holley LC, Kulis S, Marsiglia FF, Keith VM. Ethnicity versus ethnic identity: What predicts substance use norms and behaviors? Journal of Social Work Practice in the Addictions. 2006;6:53–79. [Google Scholar]
- Johnson BJ, Johnson HL. Cultural and familial influences that maintain the negative meaning of alcohol. Journal of Studies on Alcohol. 1999;13:79–83. doi: 10.15288/jsas.1999.s13.79. [DOI] [PubMed] [Google Scholar]
- Krank MD, Schoenfeld T, Frigon AP. Self-coded indirect memory associations and alcohol and marijuana use in college students. Behavior Research Methods. 2010;42:733–738. doi: 10.3758/BRM.42.3.733. [DOI] [PubMed] [Google Scholar]
- Landrine H, Klonoff EA, Corral I, Fernandez S, Roesch S. Conceptualizing and measuring ethnic discrimination in health research. Journal of Behavioral Medicine. 2006;29:79–94. doi: 10.1007/s10865-005-9029-0. [DOI] [PubMed] [Google Scholar]
- Major B, Quinton WJ, Schmader T. Attributions to discrimination and self-esteem: Impact of group identification and situational ambiguity. Journal of Experimental Social Psychology. 2003;39:220–231. [Google Scholar]
- Martin JK, Tuch SA, Roman P. Problem drinking patterns among African-Americans: The impacts of experiences with discrimination, perceptions of prejudice, and “risky” coping strategies. Journal of Health and Social Behavior. 2003;44:408–425. [PubMed] [Google Scholar]
- Mendes WB, Major B, McCoy S, Blascovich J. How attributional ambiguity shapes physiological and emotional responses to social rejection and acceptance. Journal of Personality and Social Psychology. 2008;94:278–291. doi: 10.1037/0022-3514.94.2.278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pascoe EA, Smart Richman L. Perceived discrimination and health: A meta-analytic review. Psychological Bulletin. 2009;135:531–554. doi: 10.1037/a0016059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Phinney JS. Ethnic identity in adolescents and adults: A review of research. Psychological Bulletin. 1990;108:499–514. doi: 10.1037/0033-2909.108.3.499. [DOI] [PubMed] [Google Scholar]
- Phinney JS. The Multigroup Ethnic Identity Measure: A new scale for use with diverse groups. Journal of Adolescent Research. 1992;7:156–176. [Google Scholar]
- Phinney JS. When we talk about American ethnic groups, what do we mean? American Psychologist. 1996;51:918–927. [Google Scholar]
- Phinney JS, Cantu CL, Kurtz DA. Ethnic and American identity as predictors of self-esteem among African American, Latino, and White adolescents. Journal of Youth and Adolescence. 1997;26:165–185. [Google Scholar]
- Pugh LA, Bry BH. The protective effects of ethnic identity for alcohol and marijuana use among Black young adults. Cultural Diversity and Ethnic Minority Psychology. 2007;13:187–193. doi: 10.1037/1099-9809.13.2.187. [DOI] [PubMed] [Google Scholar]
- Reyna VF, Farley F. Risk and rationality in adolescent decision making: Implications for theory, practice, and public policy. Psychological Science in the Public Interest. 2006;7:1–44. doi: 10.1111/j.1529-1006.2006.00026.x. [DOI] [PubMed] [Google Scholar]
- Rosenberg M. Society and the adolescent self-image. Princeton University Press; Princeton, NJ: 1965. [Google Scholar]
- Schmitt MT, Branscombe NR. The meaning and consequences of perceived discrimination in disadvantaged and privileged social groups. In: Stroebe W, Hewstone M, editors. European review of social psychology. Vol. 12. Wiley; Chichester, UK: 2002. pp. 167–199. [Google Scholar]
- Sellers RM, Caldwell CH, Schmeelk-Cone KH, Zimmerman MA. Racial identity, racial discrimination, perceived stress, and psychological distress among African American young adults. Journal of Health and Social Behavior. 2003;43:302–317. [PubMed] [Google Scholar]
- Sellers RM, Copeland-Linder N, Martin PP, Lewis RL. Racial identity matters: The relationship between racial discrimination and psychological functioning in African American adolescents. Journal of Research on Adolescence. 2006;16:187–216. [Google Scholar]
- Sellers RM, Smith MA, Shelton JN, Rowley SAJ, Chavous TM. Multidimensional model of racial identity: A reconceptualization of African American racial identity. Personality and Social Psychology Review. 1998;2:18–39. doi: 10.1207/s15327957pspr0201_2. [DOI] [PubMed] [Google Scholar]
- Shelton JN, Sellers RM. Situational stability and variability in African American racial identity. Journal of Black Psychology. 2000;26:27–50. [Google Scholar]
- Sherman DK, Cohen GL. The psychology of self-defense: Self-affirmation theory. In: Zanna MP, editor. Advances in experimental social psychology. Vol. 38. Academic Press; San Diego, CA: 2006. pp. 183–242. [Google Scholar]
- Simons RL, Murry V, McLoyd V, Lin K-H, Cutrona CE, Conger RD. Discrimination, crime, ethnic identity, and parenting as correlates of depressive symptoms among African American children: A multilevel analysis. Development & Psychopathology. 2002;14:371–393. doi: 10.1017/s0954579402002109. [DOI] [PubMed] [Google Scholar]
- Smart Richman L, Leary MR. Reactions to discrimination, stigmatization, ostracism, and other forms of interpersonal rejection: A multimotive model. Psychological Review. 2009;116:365–383. doi: 10.1037/a0015250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stacy AW. Memory activation and expectancy as prospective predictors of alcohol and marijuana use. Journal of Abnormal Psychology. 1997;106:61–73. doi: 10.1037//0021-843x.106.1.61. [DOI] [PubMed] [Google Scholar]
- Steele CM, Spencer SJ, Aronson J. Contending with group image: The psychology of stereotype and social identity threat. In: Zanna MP, editor. Advances in experimental social psychology. Vol. 37. Academic Press; San Diego, CA: 2002. pp. 379–440. [Google Scholar]
- Tajfel H. Human groups and social categories: Studies in social psychology. Cambridge University Press; Cambridge, UK: 1981. [Google Scholar]
- Thomas Y, Price L, Lybrand A. Drug use trajectories in minority youth. Springer; New York: (in press) [Google Scholar]
- Thush C, Wiers RW, Ames SL, Grenard JL, Sussman S, Stacy AW. Apples and oranges? Comparing indirect measures of alcohol-related cognition predicting alcohol use in at-risk adolescents. Psychology of Addictive Behaviors. 2007;21:587–591. doi: 10.1037/0893-164X.21.4.587. [DOI] [PubMed] [Google Scholar]
- Vega WA, Gil AG. Drug use and ethnicity in early adolescence. Plenum; New York, NY: 1998. [Google Scholar]
- Wallace SA, Fisher CB. Substance use attitudes among urban Black adolescents: The role of parent, peer, and cultural factors. Journal of Youth and Adolescence. 2007;36:441–451. [Google Scholar]
- Watt TT. The race/ethnic age crossover effect in drug use and heavy drinking. Journal of Ethnicity in Substance Abuse. 2008;71:93–114. doi: 10.1080/15332640802083303. [DOI] [PubMed] [Google Scholar]
- West SG, Aiken LS, Krull JL. Experimental personality designs: Analyzing categorical by continuous variable interactions. Journal of Personality. 1996;64:1–48. doi: 10.1111/j.1467-6494.1996.tb00813.x. [DOI] [PubMed] [Google Scholar]
- Williams DR, Mohammed S. Discrimination and racial disparities in health: Evidence and needed research. Journal of Behavioral Medicine. 2009;32:20–47. doi: 10.1007/s10865-008-9185-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, Spencer M, Jackson JS. Race, stress, and physical health: The role of group identity. In: Contrada RJ, Ashmore RD, editors. Self, social identity, and physical health: Interdisciplinary explorations. Oxford University Press; New York, NY: 1999. pp. 71–100. [Google Scholar]
- Williams KD, Carter-Sowell AR. Marginalization through social ostracism: Effects of being ignored and excluded. In: Butera F, Levine JM, editors. Coping with minority status: Responses to exclusion and inclusion. Cambridge University Press; New York, NY: 2009. pp. 104–122. [Google Scholar]
- Williams KD, Cheung CKT, Choi W. Cyberostracism: Effects of being ignored over the Internet. Journal of Personality and Social Psychology. 2000;79:748–762. doi: 10.1037//0022-3514.79.5.748. [DOI] [PubMed] [Google Scholar]
- Wirth JH, Williams KD. “They don’t like our kind”: Consequences of being ostracized while possessing a group membership. Group Processes & Intergroup Relations. 2009;12:111–127. [Google Scholar]
- Wong CA, Eccles JS, Sameroff A. The influence of ethnic discrimination and ethnic identification on African American adolescents’ school and socioemotional adjustment. Journal of Personality. 2003;71:1197–1232. doi: 10.1111/1467-6494.7106012. [DOI] [PubMed] [Google Scholar]
- Yip T. Everyday experiences of ethnic and racial identity among adolescents and young adults. In: Quintana SM, McKown C, editors. The handbook of race, racism, and the developing child. John Wiley; New York, NY: 2007. pp. 182–202. [Google Scholar]