

Abstract
Suprapubic catheter placement has associated complications such as bowel injury, bladder injury, or bleeding. This case describes the management of an elderly patient who had suprapubic catheter placement complicated by small bowel obstruction. The catheter had continued production of urine. Further patient treatment required abdominal exploration and bowel resection.
Keywords: General urology, Suprapubic catheter, Bowel obstruction
Introduction
The placement of a suprapubic catheter allows for percutaneous drainage of the bladder and bypass of the urethra. A key to proper insertion is expertise in the field and anatomical knowledge. Standard insertion is made superior to the pubic bone to allow proper drainage of urine. This procedure comes with several complications including recurrent urinary tract infections, bowel injury, bowel obstruction, bleeding, or injury to the bladder.
Case presentation
An 84-year-old female living at a nursing home presented to the emergency department from an outside facility with complaints of increasing dull abdominal pain for the past twenty-four hours. The pain has progressively worsened and is diffuse in nature. Four days prior to presentation, she had a suprapubic catheter placed at an outside facility and was discharged back to the nursing home without complication. On presentation, she was hypotensive but responded well to a two-liter fluid bolus. Physical examination revealed a distended abdomen with tenderness and peritoneal signs throughout the abdomen. Guarding and rigidity were noted upon palpation. Her white blood cell count was 12.8 thou/uL. She had acute kidney injury with creatinine of 3.79 mg/dL. Computed tomography of the abdomen and pelvis indicated a high grade small bowel obstruction with bowel inflammation (Fig. 1). She was admitted to the intensive care unit for resuscitation prior to operation. The patient went to the operating room for an exploratory laparotomy.
Figure 1.
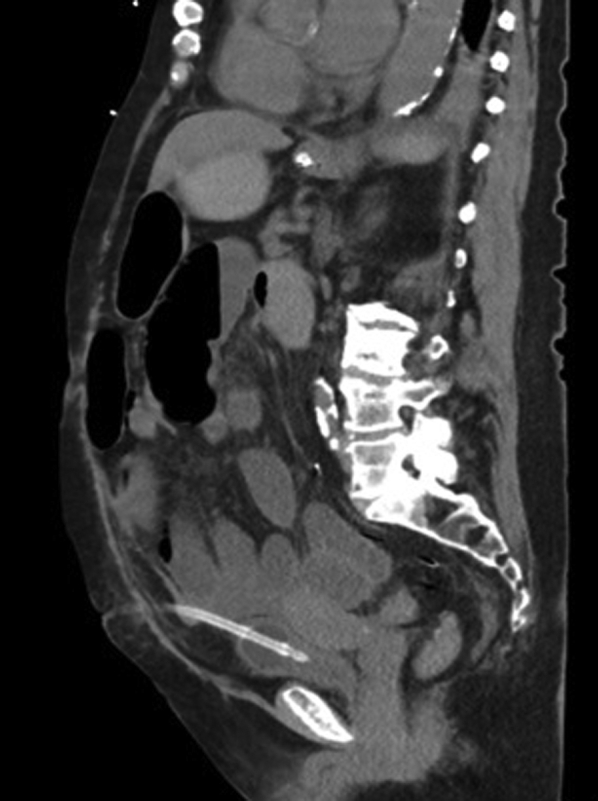
Computed tomography scan depicting small bowel obstruction with air fluid levels.
Laparotomy revealed the suprapubic catheter through the middle of the distal ileum (Fig. 2). The catheter proceeded through the distal ileum to the appropriate position in the dome of the bladder. The involved portion of small bowel was resected back to healthy margins and a hand sewn end-to-end anastomosis was performed. She progressed through the hospitalization without any complications. She tolerated a regular diet with assistance and was discharged back to the nursing facility.
Figure 2.

Intraoperative image of suprapubic catheter through distal ileum.
Discussion
Suprapubic catheter related small bowel injury or obstruction is an uncommon complication of a common urologic procedure. Keen observation and patient evaluation are essential to making the diagnosis post-procedure. These patients often present to a medical facility days to weeks after initial suprapubic catheter placement. Typically they have an obstructive picture with a history of progressively worsening abdominal pain with distention, nausea and vomiting, and obstipation. Timely diagnosis with clinical exam, imaging, and general surgery evaluation are critical to patient recovery.
The most serious rare complications associated with suprapubic catheters are bowel perforation and obstruction.1 In a related case of obstruction, a suprapubic catheter was noted to transfix a loop of pelvic small bowel before entering the bladder.2 Other more common complications of suprapubic catheter placement are hematuria and urinary tract infections.3 Bowel perforation is an infrequent occurrence and is more likely to happen during routine changes of suprapubic catheters. In some instances, the perforation has been noted to occur months after initial catheter placement warranting the need for careful follow-up.4 Laparotomy and repair of the perforation is the standard of care for patients presenting with bowel perforation.5 If treated early, patients typically do quite well.
Conclusion
Suprapubic catheterization must be performed in a careful manner. The operating physician must understand the potential complications associated with catheter placement with timely diagnosis and treatment.
Conflicts of interest
No conflicts of interest.
Acknowledgment
“Research reported in this publication was supported by the NIGMS of the National Institutes of Health under award number U54GM104942. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.”
References
- 1.Adeyemo B., Makovitch S., Foo D. A peculiar complication of suprapubic catheterization: Recurrent ureteral obstruction and hydronephrosis. J Spinal Cord Med. 2013;36(2):166–169. doi: 10.1179/2045772312Y.0000000080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gallagher K.M., Good D.W., Brush J.P. Small bowel injury after suprapubic catheter insertion presenting 3 years after initial insertion. BMJ Case Rep. 2013;2013 doi: 10.1136/bcr-2013-201436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mongiu A.K., Helfand B.T., Kielb S.J. Small bowel perforation during suprapubic tube exchange. Can J Urol. 2009;16(1):4519–4521. [PubMed] [Google Scholar]
- 4.Ahmed S.J., Mehta A., Rimington P. Delayed bowel perforation following suprapubic catheter insertion. BMC Urol. 2004;4(1):16. doi: 10.1186/1471-2490-4-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Witham M.D., Martindale A.D. Occult transfixation of the sigmoid colon by suprapubic catheter. Age Ageing. 2002;31(5):407–408. doi: 10.1093/ageing/31.5.407. [DOI] [PubMed] [Google Scholar]