

Abstract
Study Objectives:
To examine the longitudinal relationship between sleep problems and development of antisocial behavior from adolescence through young adulthood, and to investigate whether family functioning moderates the association being examined. Potential sex differences were also explored.
Methods:
A total of 2,491 adolescents participated in a prospective study spanning 2009 through 2014 in northern Taiwan. Measures included sleep problems, family functioning (parental support, family interaction, and family conflict), antisocial behavior, and other individual characteristics (sex, age, parental education, family economic stress, depressive symptoms, and stressful life events). Random coefficient growth models were used to test study hypotheses.
Results:
Sleep problems were significantly and positively associated with antisocial behavior (B = 0.088 and 0.038 for males and females, respectively).
Sex differences further emerged in the moderating effects of family functioning. Among males, those with high family interaction had a weaker association between sleep problems and antisocial behavior; among females, the examined association was weaker in those with high parental support. For both sexes, the association between sleep problems and antisocial behavior was stronger for those with high family conflict.
Conclusions:
Our findings highlight the robust link between sleep problems and adolescent antisocial behavior over time. We also show for the first time that the association depends on family functioning. Prevention methods and treatment of sleep problems in youths that incorporate family functioning may yield significant benefits for decreasing antisocial behavior. Sex-specific intervention and prevention approaches should also be considered.
Citation:
Chang LY, Wu CC, Lin LN, Yen LL, Chang HY. The effects of sleep problems on the trajectory of antisocial behavior from adolescence through early adulthood in Taiwan: family functioning as a moderator. SLEEP 2016;39(7):1441–1449.
Keywords: sleep problems, antisocial behavior, family functioning, adolescence
Significance.
The results of the present study shed new lights on the associations among sleep problems, family functioning, and antisocial behavior through a developmental lens. We demonstrated for the first time that the negative effects of sleep problems on antisocial behavior could be lessened by targeting family functioning for intervention. The current findings also highlight the need for sex-specific strategies for antisocial behavior intervention and prevention programs. While the present study provided evidence that the association between sleep problems and antisocial behavior is modifiable, little is known about the specific mechanisms through which sleep problems may affect antisocial behavior or vice versa. More research is needed to understand the nature of the association between sleep problems and antisocial behavior.
INTRODUCTION
Sleep in adolescents has received increasing public health attention because it has an important role in the development of psychological and behavioral functioning.1,2 Nevertheless, sleep problems in adolescents are still prevalent and have continued to grow in recent years.3 Epidemiological studies have shown that the prevalence of sleep problems in children and adolescents ranges between 8% and 40%.4–6 Sleep disorders such as excessive daytime sleepiness, insomnia, sleep-disordered breathing, and restless legs syndrome are also frequently observed among children and adolescents.7,8
Research has found that sleep problems during childhood and adolescence constitute a risk factor for psychopathological symptoms later in life.9,10 For example, a longitudinal study reported that greater levels of sleep impairment was significantly associated with more severe manic and depressive symptoms over a 2-year period.11 Sleep problems in childhood were also found to predict increases in later anxiety disorder and oppositional defiant disorder, as well as elevated risks of externalizing problems.12,13 However, many questions still remain regarding the relationship between sleep problems and antisocial behaviors in the adolescent population. Notably, most previous studies were constrained by a relatively small sample size, a cross-sectional study design, a selected sample population of toddlers or young children, and a reliance on data that encompass only a limited time span in the developmental process.
Different underlying mechanisms have been proposed to explain the predictive links between sleep and antisocial behavior.14 One hypothesis emphasizes the role of the prefrontal cortex (PFC) in the relationship between sleep problems and rule-breaking behaviors. The PFC is associated with the ability to anticipate, delay, and initiate behavioral responses based on cognitive and social contexts, and evidence suggests that sleep problems may reduce PFC functioning,15 resulting in the loss of inhibition that characterizes context-inappropriate responses.16 Uncontrolled, rule-breaking behaviors may consequently follow. Some evidence also suggests that sleep loss elevates stress hormone levels in the brain, which in turn interferes with attention management and behavioral regulation.17
Certain individuals may be more susceptible to the effects of sleep problems.14 Evidence has shown that children with high temperamental resistance to control are more vulnerable to the negative effects of sleep problems on externalizing behaviors than those with moderate or low temperamental resistance to control.18 In addition, stronger associations between sleep disruptions and externalizing behaviors were observed for African Americans and lower socioeconomic status children in comparison with European Americans and children with higher socioeconomic status.19 These findings imply that the relationship between sleep problems and antisocial behavior may vary by certain characteristics. Research has also called for a closer examination of the issue of moderators in the longitudinal relationships between sleep and behavioral problems.9 However, no study has yet examined the potential moderating role of family functioning in the relationship between sleep problems and antisocial behavior despite the evidence that it may act as a stressor or an ameliorator and therefore interact with an adolescent's sleep.10,20
The possible synergistic effects of sleep problems and family characteristics on antisocial behavior are supported by the ecological model of youth development21,22 and the perspectives of the resilience model.23,24 The ecological model posits that characteristics of different contexts, such as families, schools, and neighborhoods in which adolescents reside, may collectively influence their development, including sleep. The resilience model proposes that the existence of protective factors may reduce the extent to which risk factors influence outcomes. Additionally, other risks could enhance the negative effects of risk factors on outcomes. Family functioning such as parental support, family interaction, and family conflict are potential moderators in the relationship between sleep problems and antisocial behavior. Research has demonstrated that adolescents with more parental support report better sleep outcomes compared with those who have less parental support.25 Benoit et al. found that secure maternal attachment was negatively associated with children's sleep problems.26 Further, poor parent-child relations have been linked to sleep problems in a sample of 2,004 elementary school children.27 Consequently, improving family interactions could help reduce sleep problems.28 Conversely, family conflict was found to be positively associated with sleep problems.29,30 Specifically, Gregory et al. found that more family conflict during childhood predicted later insomnia symptoms at age 18.30 Similarly, exposure to marital conflict predicted a reduced amount of sleep, poorer sleep quality, increased sleep fragmentation, and a higher level of subjective sleepiness31; such relationships were more robust for African American children and those from lower socioeconomic status homes.32 By using structural equation modeling, El-Sheikh et al. further revealed that marital conflict first increased emotional insecurity, which in turn predicted increased sleep problems.33 Considering the effects of family characteristics in the association between sleep problems and antisocial behavior is essential, especially for adolescents in Taiwan. Under the influence of Confucianism, the role of family plays an important part of daily life in Taiwan. In fact, the majority of the “five relationships” (i.e., sovereign and subject, father and son, husband and wife, elder and younger siblings, and friend and friend) defined by Confucius to provide a basis for the norms of interpersonal behavior are family relations, thus clearly showing the importance of family in Taiwanese culture.34
Research regarding sex differences in the relationships between sleep and behavioral problems shows inconsistent results. In 763 French adolescents, poor sleep was related to illicit drug use in boys but not in girls.20 However, a stronger association between sleep problems and substance use was found in girls than in boys in a study of 13,381 US adolescents.35 Other longitudinal studies19,36 have reported no significant sex difference in the sleep-child development link. Because there is a dearth of studies regarding sex differences, in addition to the inconsistent results across research, it is important to ascertain whether the effects of sleep problems on antisocial behavior vary by sex.
The current study builds on the existing literature by examining the longitudinal relationship between sleep problems and development of antisocial behavior from adolescence through young adulthood. Moreover, we investigated whether family functioning moderated the effects of sleep problems on outcomes. We hypothesized that the negative effects of sleep problems on antisocial behavior would be buffered by parental support and family interaction but are exacerbated by family conflict. Finally, we explored whether the effects of sleep problems and the moderating effects of family characteristics on antisocial behavior vary by sex. We had no specific hypothesis regarding sex differences in the effects of sleep problems on antisocial behavior, given the inconsistent findings across studies.
METHODS
Data and Sample
The study data came from the Child and Adolescent Behaviors in Long-term Evolution (CABLE) project,37 a multi-wave longitudinal study of health and risk behaviors in children and adolescents. Nine elementary schools from an urban area (Taipei City) and 9 from a rural area (Hsingchu County) in northern Taiwan were selected. The 1st and 4th grade students in each school were sampled to be followed annually. There were 14 waves of data collection at 1-year intervals from 2001 to 2014. Informed consent was obtained from either a child's parent or a guardian at baseline. The CABLE study was approved by the Internal Review Board of the National Health Research Institutes (approval code: EC9009003). The current study used data from the final 6 waves (waves 9–14), which were the only waves to include measurements of sleep problems. Response rates ranged between 67.11% and 84.69% during waves 9–14. The study sample included participants who were 14–16 years old in 2009 and 19–21 years old in 2014, and it excluded those who had missing data on age across all waves (n = 228) and those who completed only one wave of data collection (n = 138). The final sample had 2,491 participants. Of those in the analysis sample, 58.61% participated in all 6 waves, and 19.03%, 10.84%, 6.38%, and 5.14% participated only in 5, 4, 3, and 2 waves, respectively. There was no significant difference regarding covariates, family functioning, or antisocial behavior between participants included in the analysis sample and those who were excluded. Approximately half of the sample was male (50.58%), and the most frequently reported parental education level was senior high school (50.94% and 60.80% for father and mother, respectively). In 2009, only 13.58% of the participants came from a single-parent household, and 37.27% indicated that their family economic stress was low.
Measures
Sleep Problems
Adolescents were asked, “how often have you had the following sleep problems in the past month?” Six sleep problems were listed: “having trouble sleeping,” “having sleep disruption,” “waking in the middle of the night or early morning,” “being unable to breathe comfortably,” “having excessive daytime sleepiness,” and “taking medicine to help sleep.” All responses were on a 5-point scale ranging from 1 for “never” to 5 for “every day.” An overall sleep problems score was computed by averaging the 6 items, with higher scores indicating more sleep problems. Cronbach α was 0.65 in 2009.
Antisocial Behavior
Nine items were used to assess antisocial behavior in each wave. Participants were asked “During the past month, how often have you done the following things (to others)?” The 9 items were “cursed,” “fought,” “hit,” “purposely destroyed public property,” “stolen,” “used weapon or object to attack,” “used force to get money or things,” “destroyed things when angry,” and “cheated on school tests.” The response categories ranged from never (1) to every day (4). The nine items were averaged to reflect participants' involvement in antisocial behaviors. Higher scores indicated higher levels of antisocial behaviors. Cronbach α was 0.78 in 2009.
Family Functioning
Parental support was measured at each wave and included six items about whether each parent “encourages me when I face hardships,” “tells me when I do a good job on things,” “comforts me when I am upset,” “takes care of me when I am not feeling well,” “pays attention to me when I am talking,” and “proactively cares about my school life.” Response categories ranged from never (1) to every time (4). Items were averaged, with higher scores indicating more parental support. Cron-bach α was 0.90 in 2009. Family interaction was measured by 4 items in each wave asking participants how often they did the following with parents in the past week: “chatted,” “ate together,” “did activities,” and “hung out.” Response categories ranged from never (1) to every day (4). Items were averaged, with higher scores reflecting more family interaction. Cron-bach α was 0.80 in 2009. Family conflict was measured only at wave 9 and consisted of 5 items asking participants whether in the past month they “argued with siblings,” “hit siblings,” “argued with parents or other adults at home,” and whether their father and mother “argued” or “hit” each other. Items were rated on a 4-point scale from never (1) to every day (4) and were averaged to create a family conflict score. Higher scores indicated more family conflict. Cronbach α was 0.57 in 2009.
Control Variables
Participants reported biological sex and current age for each wave of data collection. Father's education and mother's education were measured by participants' report of the highest level of education attained by parents across waves, ranging from junior high school or less (0) to college or more (2). Family structure indicated whether the participants reported living in a single-parent household in each wave of data collection. Family economic stress was measured by an item asking participants' perceptions about their family economy. The response categories ranged from good (1) to bad (3). Depressive symptoms were measured based on the Center for Epidemio-logical Studies Depression Scale for Children (CES-DC) and included 7 items (e.g., “had a loss of appetite,” “felt sad, cried for no reason,” “got upset over nothing”). Items were measured on a 3-point scale and were averaged to create a depressive symptoms score, with a higher score indicating more depressive symptoms. Cronbach α was 0.79 in 2009. Stressful life events were measured in 2009 and 2010, and consisted of 14 items (e.g., “broken romantic relationship,” “serious illness,” “house moving”). Response categories (1 = yes and 0 = no) were first summed to a total score and then averaged across 2 years to reflect a mean score of stressful life events. Higher scores indicated more stressful life events.
Data Analysis
Missing data were handled through multiple imputation using SAS PROC MI and PROC MIANALYZE.38 Ten sets of missing values were imputed using multiple-chain Markov Chain Monte Carlo methods. Random growth curve models conducted using Proc Mixed in SAS Version 9.338 was used to test study hypotheses. We first determined the optimal unconditional growth curve model of antisocial behavior by using age as the primary metric of time to estimate the average trajectory of antisocial behavior from ages 14 to 21. For both sexes, the best-fitting unconditional model of antisocial behavior was a linear model with an autoregressive error structure and included two random effects (individual random intercept and individual random slope). To adjust for non-normality in the distribution of the outcome, the repeated measures for antisocial behavior were log-transformed. Study hypotheses were then tested by estimating a series of conditional growth curve models. All time-varying variables (family structure, family economic stress, depressive symptoms, sleep problems, parental support, and family interaction) were person-mean centered and time invariant variables (parental education, stressful life events, and family conflict) were grand-mean centered before modeling.39 Next, we examined the relationships between sleep problems and antisocial behavior trajectories by estimating a model that included sleep problems, family functioning, and individual covariates. To test hypotheses about moderators, we added various sets of interaction terms between sleep problems and each family functioning measure to the model and determined the joint significance of their contribution using multivariate Wald tests (α = 0.05). Post hoc analyses were used to probe the nature of significant interactions. Finally, models were stratified by sex to examine potential sex differences.
RESULTS
Descriptive Analyses
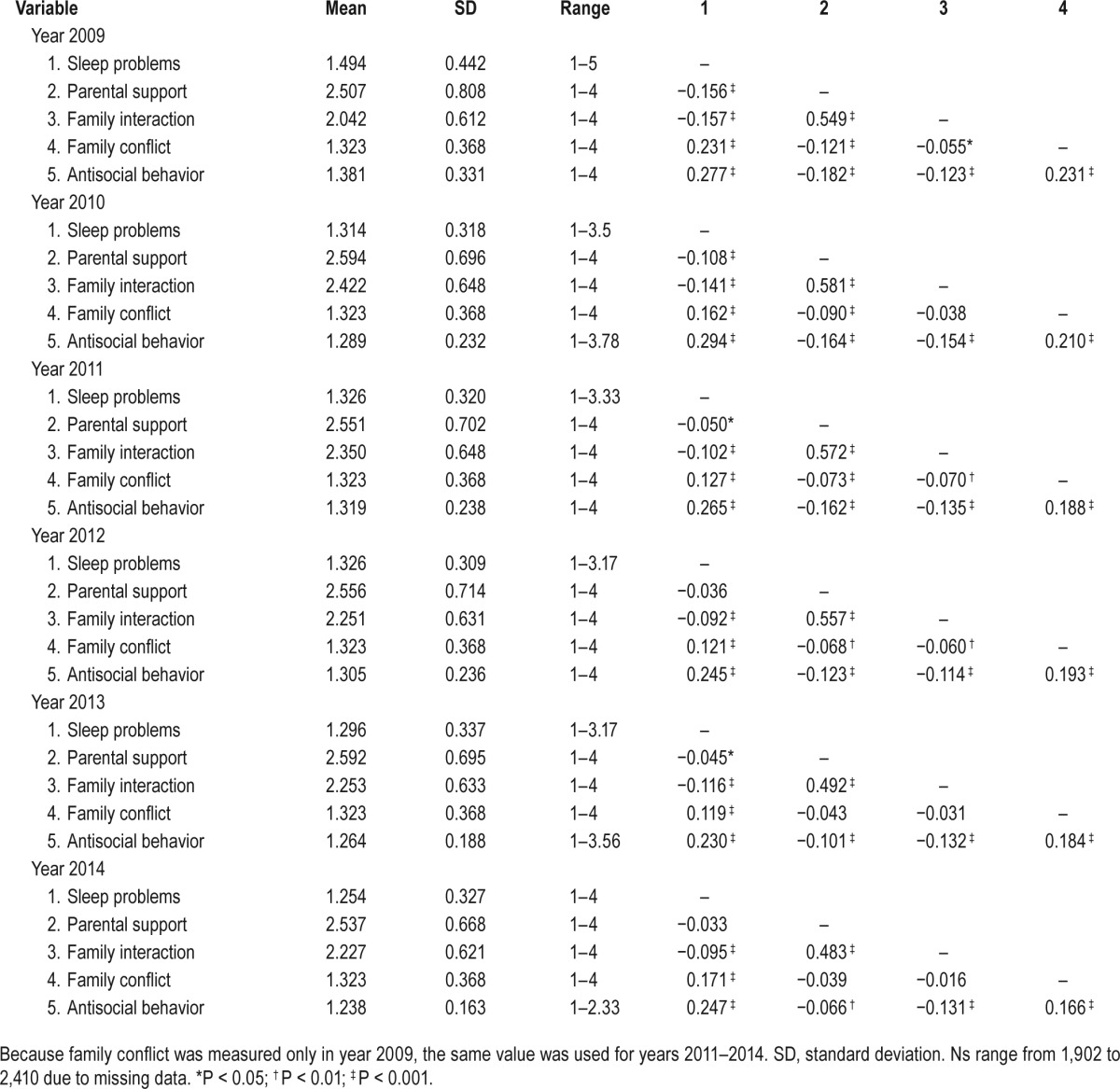
Table 1 presents the descriptive statistics and Spearman correlations for sleep problems, family functioning, and antisocial behaviors from 2009 to 2014. The correlations showed that sleep problems were positively and significantly associated with antisocial behavior across years. In addition, higher levels of parental support and higher levels of family interaction were significantly associated with lower levels of antisocial behavior. Conversely, higher levels of family conflict were found to be correlated with higher levels of antisocial behavior.
Table 1.
Descriptive statistics and correlations for sleep problems, moderators, and antisocial behaviors.
Relationships between Sleep Problems and Antisocial Behavior
The results of the model assessing the effects of sleep problems on antisocial behavior trajectory after controlling for family functioning and individual covariates are presented in Table 2 (Model 1). Sleep problems were significantly and positively related to levels of antisocial behavior with stronger effects observed in males than in females (B = 0.088 and 0.038 for males and females, respectively). The effects of sleep problems on antisocial behavior were also found to vary over time (sleep problems × age: B = −0.014 and −0.007 for males and females, respectively). Specifically, adolescents with high levels of sleep problems had higher initial levels of antisocial behaviors and a faster rate of decrease in antisocial behavior over time than those with low levels of sleep problems (Figure 1). However, additional analyses show that after controlling for covariates, the mean scores of antisocial behavior remained significantly higher in adolescents with more sleep problems than in those with less sleep problems by age 20 and age 18 for males and females, respectively.
Table 2.
Family functioning measures as moderators of the association between sleep problems and antisocial behavior from ages 14 through 21.
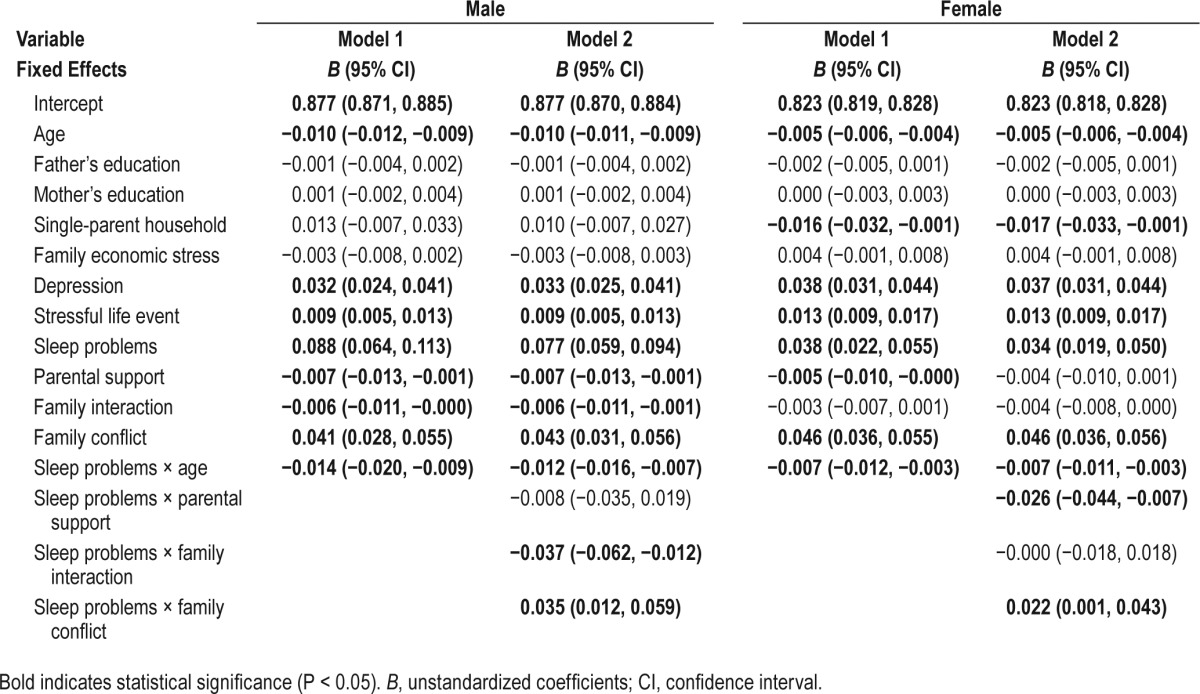
Figure 1.
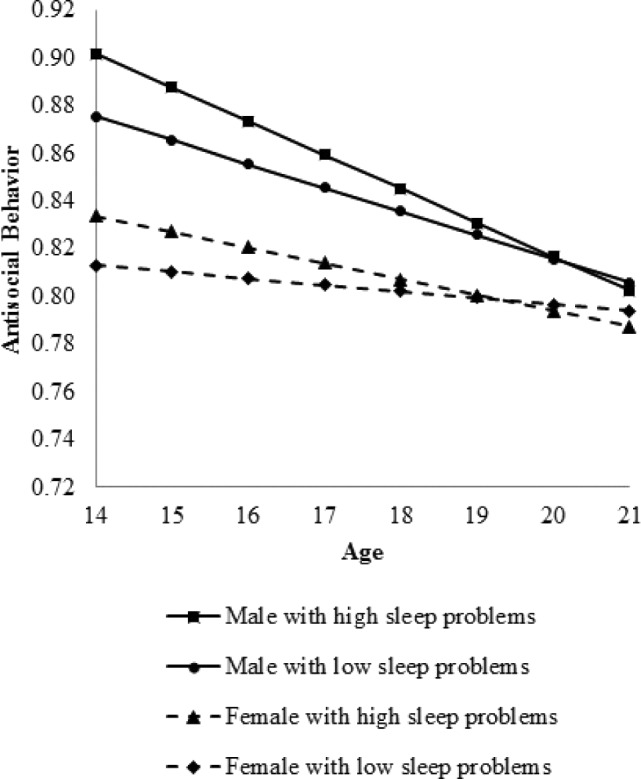
The effects of sleep problems on the trajectory of antisocial behavior from ages 14 to 21 years by sex.
Family Functioning as a Moderator
Supporting our study hypotheses, parental support, family interaction, and family conflict were found to moderate the association between sleep problems and the trajectory of antisocial behavior (Model 2 in Table 2). However, varying moderation patterns emerged for males and females. For males, the negative effects of sleep problems on antisocial behavior were buffered by family interaction. Specifically, the negative effects of sleep problems were less in male adolescents with high levels of family interaction than in those with low levels of family interaction (B = 0.061 and 0.092, respectively; Figure 2A). For females, the negative effects of sleep problems on antisocial behavior were buffered by parental support. As shown in Figure 3A, the negative effects of sleep problems on antisocial behavior were less for female adolescents with high levels of parental support than for those with low levels of parental support (B = 0.024 and 0.045, respectively). For both male and female adolescents, family conflict exacerbated the negative effects of sleep problems on antisocial behavior such that stronger effects were observed in adolescents with high levels of family conflict compared with those with low levels of family conflict (Males: B = 0.088 and 0.062, respectively, Figure 2B; Females: B = 0.043 and 0.027, respectively, Figure 3B).
Figure 2.

The moderating effects of parental interaction and family conflict in the association between sleep problems and antisocial behavior in male adolescents.
Figure 3.

The moderating effects of parental support and family conflict in the association between sleep problems and antisocial behavior in female adolescents.
DISCUSSION
This study addressed gaps in the literature by longitudinally examining the effects of sleep problems and the moderating effects of family functioning on antisocial behaviors trajectory from adolescence to young adulthood. The results confirm that adolescents with sleep problems are more likely to develop antisocial behavior. Our findings are the first to show that the negative effects of sleep problems on antisocial behavior are moderated by family functioning. Significant sex differences were also observed in the main effect of sleep problems and in the buffering effect of family functioning on the trajectory of antisocial behavior.
Sleep problems appear to be a robust risk factor for antisocial behavior. This result corresponds to previous findings relating sleep to various adolescent risk behaviors.36,40 We further demonstrated that the effects of sleep problems on antisocial behavior vary by time. Although higher levels of sleep problems were associated with higher levels of antisocial behavior in early and middle adolescence, the effects diminished over time. By late adolescence, sleep problems were no longer predictive of individual differences in levels of antisocial behavior. This phenomenon suggests that sleep problems alone may not be sufficient to explain persistence of antisocial behavior throughout a lifetime. Moffitt's theory41 described a number of different forces (e.g., genetic factors, social and structural aspects of the environment) that, together with sleep problems, may contribute to the development of antisocial behavior. Accordingly, our results indicate the need to consider the influences of time and multiple risk factors in examining the effects of sleep problems on antisocial behavior.
The findings that sleep problems had a less pronounced effect on antisocial behavior for adolescents in families with more support and interaction are consistent with the perspective of the protective model of resilience.23 Specifically, parental support and family interaction operated as protective factors that reduced the negative effects of sleep problems on antisocial behavior. Although sleep problems may alter stress hormone levels and PFC functioning and lead to inappropriate behaviors, interpersonal relationships that involve support and interaction can enhance the ability of adolescents to cope and respond,42 which can decrease the risk of exhibiting antisocial behavior promoted by sleep problems. Adolescents with high levels of parental support and family interaction may also have ingrained prosocial values that help reduce antisocial behavior when they lose their inhibitions and are prone to inappropriate responses because of sleep problems. The current findings also agree with the views of the socioecological framework suggesting that factors from different domains of life may combine to influence adolescent development. Although there is currently no other study examining the moderating effects of parental support and family interaction in the relationship between sleep problems and antisocial behavior, the potential buffering effects of family functioning have been reported for other adolescent behaviors.43
Our findings that family conflict enhanced the negative effects of sleep problems on antisocial behavior also are in accordance with the view of the resilience model,24 in which family conflict is seen as a vulnerable reactive factor that heightens the disadvantages associated with increasing levels of risks. That is, the risk of antisocial behavior associated with sleep problems is higher for adolescents with more family conflicts than for those with less family conflicts. Deep sleep requires a relative cessation of awareness and responsiveness to the external environment; however, family conflict contributes to increased vigilance, which requires a heightened sensitivity to the external environment, and may exacerbate sleep problems.10 Similar findings were also reported by Lemola and colleagues,44 but their study suffers from the limitations of small sample size and cross-sectional study design. Therefore, our study contributes to the current understanding of family conflict as a moderator in the longitudinal associations between sleep problems and antisocial behavior.
In terms of sex differences, we found that the negative effects of sleep problems on antisocial behavior were stronger for males than for females. Such variation could be explained by the sex differences in sleep. Compared to girls, boys generally have more sleep problems,45,46 and these sex differences may affect how sleep problems impact the antisocial behavior of boys differently from girls. Further, we found different buffering effects of family support and family interaction for males and females. Specifically, family support buffered the negative effects of sleep problems on antisocial behavior for girls, but not for boys. Research on social support during adolescence has shown that girls perceived more support from their parents than boys did.47 Our data also showed significantly higher levels of parental support reported by girls than by boys. A developmental study further demonstrated that from middle to late adolescence, parental support significantly increased for girls but stabilized for boys.48 Perhaps the different levels and patterns of parental support received by girls and boys contributed to the sex differences in the moderation effects of parental support. We also found significant buffering effects of family interaction for boys only. Research has suggested that the effects of family interaction depend on the communication and process involved in the interaction.49 Given the sex differences in communication during family interaction,50 varying protective effects of family interaction on antisocial behavior may be observed for boys and girls. Because of the lack of research that has explored sex differences in the joint effects of sleep problems and protective family functioning on behavioral outcomes, more studies are needed to understand why and how family support and interaction differentially protect males and females from the negative effects of sleep problems on antisocial behavior.
Some limitations of our study should be noted. First, our measures of sleep problems were based solely on self-report of adolescents. The self-reported measures of both sleep problems and antisocial behavior may also produce common method variance and increase or decrease the association being examined. The use of objective data in addition to subjective data may better reflect the sleep problems that adolescents experience. Another limitation of using self-reported data is that antisocial behavior might be underestimated in the current study due to social desirability biases. However, because the CABLE project has been conducted over a decade, we believe that the trusting relationship built between participants and study staff during this period might help participants to respond truthfully. To encourage honest reporting, students were also assured that their answers were confidential and would not be disclosed to parents, teachers, or other authorities. In addition, the measurements of our study variables were adopted from various existing scales to increase their applicability to adolescents in Taiwan; therefore, validity data were not available and internal consistency was not very high. Furthermore, unlike other time-varying measures of family functioning in the current study, family conflict was treated as a time-invariant variable in our model because it was not assessed at other waves. Our results involving family conflict must be interpreted with caution because the levels of family conflict may change over time. Finally, this study cannot infer causality. Therefore, an opposite association between sleep problems and antisocial behavior may exist such that antisocial behavior may be associated with academic failure51 or peer rejection52 and thus affect sleep quality, suggesting the need for more research examining the nature of the association between sleep problems and antisocial behavior.
Nonetheless, our study has several strengths. The longitudinal nature of the data structure allowed us to examine the relationships between sleep problems and antisocial behavior over time, which increases the current understanding of the effects of sleep problems through a developmental viewpoint. Another unique aspect of our study is the examination of the potential role of family functioning in moderating the association between sleep problems and the trajectory of antisocial behavior. To the best of our knowledge, no other study has tested whether the effects of sleep problems on adolescent risk behaviors vary based on family functioning. In addition, we used multiple imputation procedures to replace missing values to minimize the effects of attrition, and we noted that 88% of adolescents completed at least four of the six surveys. Finally, several important individual covariates that might confound the relationship being examined were taken into account in the model.
In conclusion, our findings highlight the detrimental effects of sleep problems on adolescent antisocial behavior over time. The magnitude of the effects, however, depends on adolescent sex, age, and family functioning. Therefore, prevention and treatment of sleep problems in children and adolescents may yield significant benefits of decreasing antisocial behavior by considering the effects of the studied moderators. The differential effects of sleep problems on antisocial behavior in adolescents also deserve continued attention in future research.
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.
ACKNOWLEDGMENTS
The authors thank the Child and Adolescent Behaviors in Long-term Evolution project (HP-090-SG-03), funded by National Health Research Institutes and Health Promotion Administration, Ministry of Health and Welfare, for providing data for this study. Part of this study was also supported by the Ministry of Science and Technology (MOST 105-3011-F-400-001).
REFERENCES
- 1.Shochat T, Cohen-Zion M, Tzischinsky O. Functional consequences of inadequate sleep in adolescents: a systematic review. Sleep Med Rev. 2014;18:75–87. doi: 10.1016/j.smrv.2013.03.005. [DOI] [PubMed] [Google Scholar]
- 2.Lo JC, Ong JL, Leong RL, Gooley JJ, Chee MW. Cognitive performance, sleepiness, and mood in partially sleep deprived adolescents: the need for sleep study. Sleep. 2016;39:687–98. doi: 10.5665/sleep.5552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Luntamo T, Sourander A, Santalahti P, Aromaa M, Helenius H. Prevalence changes of pain, sleep problems and fatigue among 8-year-old children: years 1989, 1999, and 2005. J Pediatr Psychol. 2012;37:307–18. doi: 10.1093/jpepsy/jsr091. [DOI] [PubMed] [Google Scholar]
- 4.Byars KC, Yolton K, Rausch J, Lanphear B, Beebe DW. Prevalence, patterns, and persistence of sleep problems in the first 3 years of life. Pediatrics. 2012;129:e276–84. doi: 10.1542/peds.2011-0372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fricke-Oerkermann L, Pluck J, Schredl M, et al. Prevalence and course of sleep problems in childhood. Sleep. 2007;30:1371–7. doi: 10.1093/sleep/30.10.1371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Roberts RE, Roberts CR, Xing Y. Restricted sleep among adolescents: prevalence, incidence, persistence, and associated factors. Behav Sleep Med. 2011;9:18–30. doi: 10.1080/15402002.2011.533991. [DOI] [PubMed] [Google Scholar]
- 7.Petrov ME, Lichstein KL, Baldwin CM. Prevalence of sleep disorders by sex and ethnicity among older adolescents and emerging adults: relations to daytime functioning, working memory and mental health. J Adolesc. 2014;37:587–97. doi: 10.1016/j.adolescence.2014.04.007. [DOI] [PubMed] [Google Scholar]
- 8.Calhoun SL, Vgontzas AN, Fernandez-Mendoza J, et al. Prevalence and risk factors of excessive daytime sleepiness in a community sample of young children: the role of obesity, asthma, anxiety/ depression, and sleep. Sleep. 2011;34:503–7. doi: 10.1093/sleep/34.4.503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sadeh A, Tikotzky L, Kahn M. Sleep in infancy and childhood: implications for emotional and behavioral difficulties in adolescence and beyond. Curr Opin Psychiatry. 2014;27:453–9. doi: 10.1097/YCO.0000000000000109. [DOI] [PubMed] [Google Scholar]
- 10.Gregory AM, Sadeh A. Annual research review: sleep problems in childhood psychiatric disorders - a review of the latest science. J Child Psychol Psychiatry. 2016;57:296–317. doi: 10.1111/jcpp.12469. [DOI] [PubMed] [Google Scholar]
- 11.Lunsford-Avery JR, Judd CM, Axelson DA, Miklowitz DJ. Sleep impairment, mood symptoms, and psychosocial functioning in adolescent bipolar disorder. Psychiatry Res. 2012;200:265–71. doi: 10.1016/j.psychres.2012.07.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shanahan L, Copeland WE, Angold A, Bondy CL, Costello EJ. Sleep problems predict and are predicted by generalized anxiety/depression and oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2014;53:550–8. doi: 10.1016/j.jaac.2013.12.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sivertsen B, Harvey AG, Reichborn-Kjennerud T, Torgersen L, Ystrom E, Hysing M. Later emotional and behavioral problems associated with sleep problems in toddlers: a longitudinal study. JAMA Pediatr. 2015;169:575–82. doi: 10.1001/jamapediatrics.2015.0187. [DOI] [PubMed] [Google Scholar]
- 14.Kamphuis J, Meerlo P, Koolhaas JM, Lancel M. Poor sleep as a potential causal factor in aggression and violence. Sleep Med. 2012;13:327–34. doi: 10.1016/j.sleep.2011.12.006. [DOI] [PubMed] [Google Scholar]
- 15.Dahl RE. The regulation of sleep and arousal: development and psychopathology. Dev Psychopathol. 1996;8:3–27. [Google Scholar]
- 16.Horne JA. Human sleep, sleep loss and behaviour. Implications for the prefrontal cortex and psychiatric disorder. Br J Psychiatry. 1993;162:413–9. doi: 10.1192/bjp.162.3.413. [DOI] [PubMed] [Google Scholar]
- 17.Weissbluth M. Sleep-loss stress and temperamental difficultness: psychobiological processes and practical considerations. In: Kohnstamm GA, Bates JE, Rothbart MK, editors. Temperament in childhood. Oxford, England: John Wiley; 1989. pp. 357–75. [Google Scholar]
- 18.Goodnight JA, Bates JE, Staples AD, Pettit GS, Dodge KA. Temperamental resistance to control increases the association between sleep problems and externalizing behavior development. J Fam Psychol. 2007;21:39–48. doi: 10.1037/0893-3200.21.1.39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.El-Sheikh M, Kelly RJ, Buckhalt JA, Benjamin Hinnant J. Children's sleep and adjustment over time: the role of socioeconomic context. Child Dev. 2010;81:870–83. doi: 10.1111/j.1467-8624.2010.01439.x. [DOI] [PubMed] [Google Scholar]
- 20.Vignau J, Bailly D, Duhamel A, Vervaecke P, Beuscart R, Collinet C. Epidemiologic study of sleep quality and troubles in French secondary school adolescents. J Adolesc Health. 1997;21:343–50. doi: 10.1016/S1054-139X(97)00109-2. [DOI] [PubMed] [Google Scholar]
- 21.Bronfenbrenner U. Ecological systems theory. Annu Child Dev. 1989;6:187–249. [Google Scholar]
- 22.Grandner MA, Hale L, Moore M, Patel NP. Mortality associated with short sleep duration: the evidence, the possible mechanisms, and the future. Sleep Med Rev. 2010;14:191–203. doi: 10.1016/j.smrv.2009.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fergus S, Zimmerman MA. Adolescent resilience: a framework for understanding healthy development in the face of risk. Annu Rev Public Health. 2005;26:399–419. doi: 10.1146/annurev.publhealth.26.021304.144357. [DOI] [PubMed] [Google Scholar]
- 24.Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71:543–62. doi: 10.1111/1467-8624.00164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Brand S, Hatzinger M, Beck J, Holsboer-Trachsler E. Perceived parenting styles, personality traits and sleep patterns in adolescents. J Adolesc. 2009;32:1189–207. doi: 10.1016/j.adolescence.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 26.Benoit D, Zeanah CH, Boucher C, Minde KK. Sleep disorders in early childhood: association with insecure maternal attachment. J Am Acad Child Adolesc Psychiatry. 1992;31:86–93. doi: 10.1097/00004583-199201000-00013. [DOI] [PubMed] [Google Scholar]
- 27.Liu X, Sun Z, Uchiyama M, Shibui K, Kim K, Okawa M. Prevalence and correlates of sleep problems in Chinese schoolchildren. Sleep. 2000;23:1053–62. [PubMed] [Google Scholar]
- 28.Framer EM, Sanders SH. The effects of family contingency contracting on disturbed sleeping behaviors in a male adolescent. J Behav Ther Exp Psychiatry. 1980;11:235–7. [Google Scholar]
- 29.Smaldone A, Honig JC, Byrne MW. Sleepless in America: inadequate sleep and relationships to health and well-being of our nation's children. Pediatrics. 2007;119:S29–37. doi: 10.1542/peds.2006-2089F. [DOI] [PubMed] [Google Scholar]
- 30.Gregory AM, Caspi A, Moffitt TE, Poulton R. Family conflict in childhood: a predictor of later insomnia. Sleep. 2006;29:1063–7. doi: 10.1093/sleep/29.8.1063. [DOI] [PubMed] [Google Scholar]
- 31.El-Sheikh M, Buckhalt JA, Mize J, Acebo C. Marital conflict and disruption of children's sleep. Child Dev. 2006;77:31–43. doi: 10.1111/j.1467-8624.2006.00854.x. [DOI] [PubMed] [Google Scholar]
- 32.Kelly RJ, El-Sheikh M. Marital conflict and children's sleep: reciprocal relations and socioeconomic effects. J Fam Psychol. 2011;25:412–22. doi: 10.1037/a0023789. [DOI] [PubMed] [Google Scholar]
- 33.El-Sheikh M, Buckhalt JA, Mark Cummings E, Keller P. Sleep disruptions and emotional insecurity are pathways of risk for children. J Child Psychol Psychiatry. 2007;48:88–96. doi: 10.1111/j.1469-7610.2006.01604.x. [DOI] [PubMed] [Google Scholar]
- 34.Fan Y. A classification of Chinese culture. Cross Cult Manag. 2000;7:3–10. [Google Scholar]
- 35.Johnson EO, Breslau N. Sleep problems and substance use in adolescence. Drug Alcohol Depend. 2001;64:1–7. doi: 10.1016/s0376-8716(00)00222-2. [DOI] [PubMed] [Google Scholar]
- 36.Wong MM, Brower KJ, Zucker RA. Childhood sleep problems, early onset of substance use and behavioral problems in adolescence. Sleep Med. 2009;10:787–96. doi: 10.1016/j.sleep.2008.06.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yen LL, Chen L, Lee SH, Hsiao C, Pan LY. Child and adolescent behaviour in long-term evolution (CABLE): a school-based health lifestyle study. Promot Educ. 2002;(Suppl 1):33–40. doi: 10.1177/10253823020090010115. [DOI] [PubMed] [Google Scholar]
- 38.SAS Institute. Cary, NC: SAS Institute Inc.; 2011. SAS Software, Version 9.3. [Google Scholar]
- 39.Raudenbush SW, Bryk AS. 2nd ed. Thousand Oaks, CA: Sage; 2002. Hierarchical linear models: applications and data analysis methods. [Google Scholar]
- 40.Pieters S, Burk WJ, Van der Vorst H, Dahl RE, Wiers RW, Engels RC. Prospective relationships between sleep problems and substance use, internalizing and externalizing problems. J Youth Adolesc. 2015;44:379–88. doi: 10.1007/s10964-014-0213-9. [DOI] [PubMed] [Google Scholar]
- 41.Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev. 1993;100:674–701. [PubMed] [Google Scholar]
- 42.Cohen S, McKay G. Social support, stress, and the buffering hypothesis: a theoretical analysis. In: Baum A, Taylor SE, Singer JE, editors. Handbook of psychology and health. Hillsdale, NJ: Lawrence Erlbaum; 1984. pp. 253–67. [Google Scholar]
- 43.El-Sheikh M, Buckhalt JA. Parental problem drinking and children's adjustment: attachment and family functioning as moderators and mediators of risk. J Fam Psychol. 2003;17:510–20. doi: 10.1037/0893-3200.17.4.510. [DOI] [PubMed] [Google Scholar]
- 44.Lemola S, Schwarz B, Siffert A. Interparental conflict and early adolescents' aggression: is irregular sleep a vulnerability factor? J Adolesc. 2012;35:97–105. doi: 10.1016/j.adolescence.2011.06.001. [DOI] [PubMed] [Google Scholar]
- 45.Buckhalt JA, El-Sheikh M, Keller P. Children's sleep and cognitive functioning: race and socioeconomic status as moderators of effects. Child Dev. 2007;78:213–31. doi: 10.1111/j.1467-8624.2007.00993.x. [DOI] [PubMed] [Google Scholar]
- 46.Sadeh A, Raviv A, Gruber R. Sleep patterns and sleep disruptions in school-age children. Dev Psychol. 2000;36:291–301. doi: 10.1037//0012-1649.36.3.291. [DOI] [PubMed] [Google Scholar]
- 47.Meeus W. Psychosocial problems and social support in adolescence. In: Nestmann F, Hurrelmann K, editors. Social networks and social support in childhood and adolescence. Berlin: de Gruyter; 1994. [Google Scholar]
- 48.De Goede IH, Branje SJ, Meeus WH. Developmental changes in adolescents' perceptions of relationships with their parents. J Youth Adolesc. 2009;38:75–88. doi: 10.1007/s10964-008-9286-7. [DOI] [PubMed] [Google Scholar]
- 49.Noller P, Callan VJ. Adolescents' perceptions of the nature of their communication with parents. J Youth Adolesc. 1990;19:349–62. doi: 10.1007/BF01537077. [DOI] [PubMed] [Google Scholar]
- 50.Fitzpatrick MA, Marshall LJ, Leutwiler TJ, Krcmar M. The effect of family communication environments on children's social behavior during middle childhood. Commun Res. 1996;23:379–406. [Google Scholar]
- 51.Ma HK. The relation of academic achievement, family and classroom social environment, and peer interactions to prosocial and antisocial behavior of Chinese children. Psychologia. 2003;46:163–73. [Google Scholar]
- 52.van Lier PA, Vitaro F, Wanner B, Vuijk P, Crijnen AA. Gender differences in developmental links among antisocial behavior, friends' antisocial behavior, and peer rejection in childhood: results from two cultures. Child Dev. 2005;76:841–55. doi: 10.1111/j.1467-8624.2005.00881.x. [DOI] [PubMed] [Google Scholar]