

A 21-year-old patient who was fell during a ball game presented with pain, tenderness, and swelling of the base of his right thumb. Clinical examination revealed a deformity and restricted joint motion. Anteroposterior (AP) wrist and thumb X-ray is shown in the Figure 1. [see page 86 for diagnosis]
Figure 1.
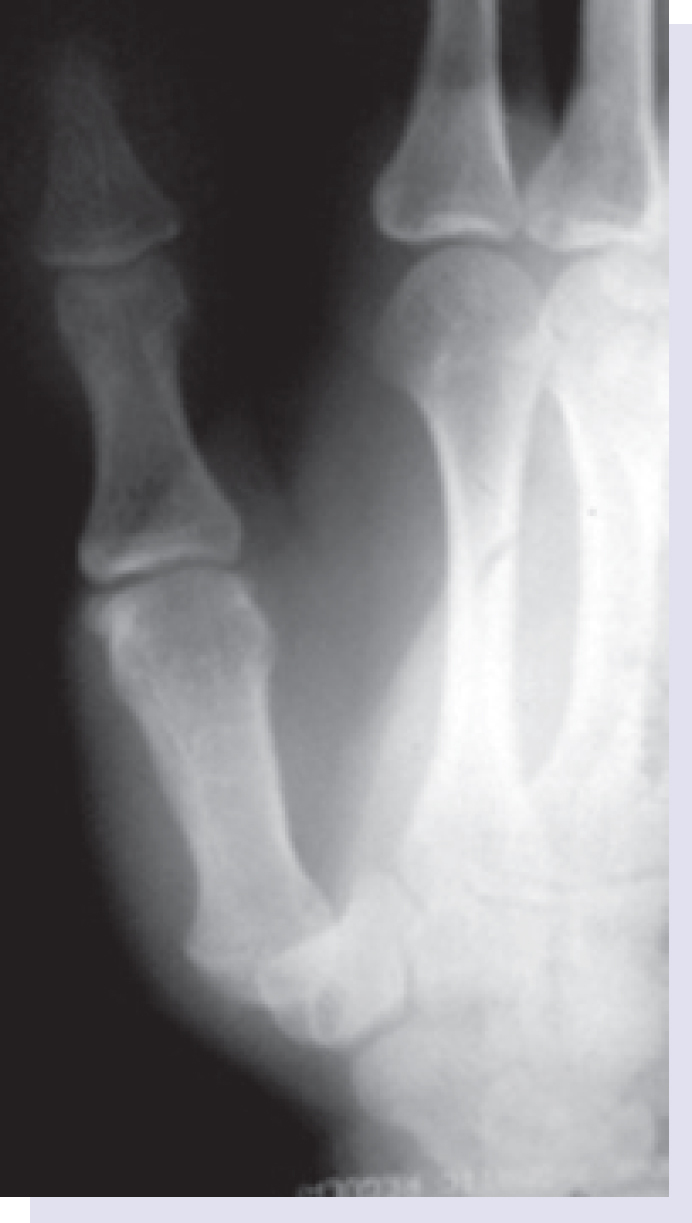
Anteroposterior and oblique radiographs of the right hand.
DIAGNOSIS: Carpometacarpal (CMC) Joint Dislocation.
Anteroposterior (AP) wrist and thumb x-ray revealed a dislocation of the CMC joint (Figure 1). No bone fracture signs were identified. The patient was treated with open reduction, pinning and capsuloraphy, and a short thumb spica cast was applied (Figure 2a, b). At 4–month follow-up, radiographic examination revealed normal joint anatomy without any signs of subluxation or early osteoarthritis.
Dislocation of the thumb carpometacarpal (CMC) joint is a rare injury in the hand. This injury is usually the result of an axial transmitted force through a partially flexed thumb.[1] The patient complained of swelling and tenderness over the CMC joint. Mechanisms of injury including sudden, strong impacts, fall from tall heights, motor vehicle accidents, and fighting must attract attention for this injury.
Dislocation of the CMC joint of the thumb is a rare injury and may be associated with other injuries such as carpal bone fractures.[2] Joint capsule and ligaments, including intermetacarpal, anterior oblique, dorsoradial, and posterior oblique ligaments, play a significant role in stabilization.[1] Joint capsule and/or ligaments are frequently damaged during dislocation.[3]
Routine AP and oblique x-ray radiographs are sufficient to evaluate the CMC joint. Computed tomography may be used in the diagnosis of complex injuries and preoperative planning.
Treatment aims to accomplish reduction and stability, with the goals of reducing pain, maintaining joint motion, and preserving strength and function. Treatment options include closed reduction and casting, open or closed reduction with pinning and reconstruction of dorsal ligament and capsulorrhaphy.[4] Inadequate treatment may induce recurrent instability, joint degeneration, and chronic pain and reduce functional capability of the joint.[5]
Figure 2.

(a) Intraoperative photograph of the dorsalateral aspect of carpometacarpal joint shows the thumb CMC joint percutaneous pinning, capsule damage and capsuloraphy. (b) Postoperative anteroposterior radiograph of carpometacarpal joint shows thumb CMC joint reduction and percutaneous pinning.
Footnotes
Published online: February 17, 2015
References
- 1.Strauch RJ, Behrman MJ, Rosenwasser MP. Acute dislocation of the carpometacarpal joint of the thumb: an anatomic and cadaver study. J Hand Surg Am. 1994;19:93–98. doi: 10.1016/0363-5023(94)90229-1. CrossRef. [DOI] [PubMed] [Google Scholar]
- 2.Tolat AR, Jones MW. Carpometacarpal dislocation of the thumb associated with fracture of the trapezium. Injury. 1990;21:411–412. doi: 10.1016/0020-1383(90)90136-i. CrossRef. [DOI] [PubMed] [Google Scholar]
- 3.Fotiadis E, Svarnas T, Lyrtzis C, Papadopoulos A, Akritopoulos P, Chalidis B. Isolated thumb carpometacarpal joint dislocation: a case report and review of the literature. J Orthop Surg Res. 2010;5:16. doi: 10.1186/1749-799X-5-16. CrossRef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sohail A, Kevin DP. Carpometacarpal dislocations of the fingers. Operative Techniques in Sports Medicine. 1996;4:257–267. CrossRef. [Google Scholar]
- 5.Simonian PT, Trumble TE. Traumatic dislocation of the thumb carpometacarpal joint: early ligamentous reconstruction versus closed reduction and pinning. J Hand Surg Am. 1996;21:802–806. doi: 10.1016/S0363-5023(96)80195-X. CrossRef. [DOI] [PubMed] [Google Scholar]