

SUMMARY
Objectives
The present study conducted demographic analysis of blast injuries, with the authors aiming to guide the determination of groups and regions at risk, helping hospitals take preventive measures and providing information for accurate triage, rapid intervention, multidisciplinary approach, and lowering workforce losses.
Methods
This study retrospectively examined the demographic properties of civilians who presented to the Emergency Department of Dicle University after being injured in explosions of various origins between January 2005 and September 2013 in the Southeastern Anatolia Region of Turkey.
Results
Of the study population, 85.50% were male and 14.50% were female. The explosive responsible for injury was a mine in 20.51% of the cases, a bomb in 29.06%, a squib in 14.53%, dynamite in 7.69%, and some other explosive in the remaining 28.31%. Of those injured, 35.90% were students, 21.36% were farmers, 11.10% were shepherds or drivers, and 31.62% were from other occupational groups.
Conclusions
In conclusion, injuries resulting from explosions are associated with higher morbidity and mortality rates, making it necessary to increase the number of trauma centers and emergency action teams in that region, as well as demining the region and educating the native population about explosives.
Key words: Amputation, blast injury, explosives
Introduction
Southeastern Anatolia Region is one of seven geographical regions in Turkey. It is the smallest, but most densely populated region. Syria and Iraq border to the south and Iran to the east. This region has the highest terrorism and smuggling rates in Turkey and its borders with neighboring countries have not been cleared of land mines. Hence, blast injuries due to explosions are common. Among civilians, explosions are encountered mostly due to terrorist activities. Although bombs are used during war, they may also rarely cause multiple blast injuries in peacetime as well. Nevertheless, substances with explosive properties other than bombs are also encountered in daily life, albeit rarely.[1] These include propane cylinders, automobile LPG systems, oil barrels, lighters, or even everyday tools that are seemingly harmless, such as pressure cookers, fireworks, squibs, vehicle power supplies, and electric panels.[2] In places where terrorist activities take place, explosives are used and when terrorist activities scale up, use of explosives shows a parallel increase.3, 4
Mines are laid during wars or for security reasons during peacetime and have enormous explosive power. They potentially remain underground or on soil for years after wars because land mines are not regularly mapped.3, 4 Land mines reduce the use of farmland,[5] delay infrastructure and government investments, and prevent the inflow of foreign capital due to the fear and threat experienced in these regions. It is reported that the cost of clearing mines is a hundred times their production cost6, 7 and that treatment costs for a mine victim are more than a thousand times their production cost. Unfortunately, thousands of new land mines are laid each year, most of which will never be cleared.[6] Fertile lands and historical places also suffer from land mines, harming agriculture and tourism. In our country, no clinical scoring or triage technique is widely used for occupational accidents, blast injuries due to domestic appliances, or certain explosives used for terrorist activities. Moreover, injury and mortality rates remain high due to lack of regulatory restrictions. This study aimed to guide the determination of groups and regions at risk, helping hospitals take preventive measures and providing information for accurate triage, rapid intervention, multidisciplinary approach, and lowering workforce losses by conducting demographic analysis of blast injuries.
Materials and Methods
This study retrospectively examined the demographic properties of 117 civilians who presented to the Emergency Department of Dicle University, Faculty of Medicine, after being injured in explosions of various origins between January 2005 and September 2013 in the Southeastern Anatolia Region of the Republic of Turkey. This article is a cross-sectional observational study. All patients were examined, resuscitated in compliance with ATLS (Advanced Trauma Life Support), and treated per available protocols for diagnosis and treatment in the emergency department.
Inclusion criteria
-
1-
Injuries to civilians with materials meeting the criteria set for explosives
-
2-
Injuries caused by explosions occurring in peacetime
-
3-
Injuries with hospital records which were accessible from the Dicle University Faculty of Medicine, Emergency Department.
Exclusion Criteria
-
1-
Injuries to security or military personnel
-
2-
Blast injuries during wartime
-
3-
Other traumatic injuries (firearm wounds, traffic accidents, and falls from a height, etc.)
Data Analysis
Patient data recorded in sociodemographic forms included age, sex, site of incident (rural/urban/abroad), distribution of injured body parts (extremity, head, thorax, abdomen, other), location and distribution of extremity amputation, clinic of admission, type/site of explosion, distribution of clinical outcome of explosion, and distribution of occupation by type of explosive materials (mines, bombs, squibs, dynamites). Statistical analyses were performed using SPSS for Windows Ver. 15.0. Univariate analyses were performed using the Chi-Square test (χ2) for categorical variables and the student's t test for continuous variables. The study data were expressed as Mean±SD. A p value less than 0.05 was considered statistically significant.
Results
This study retrospectively examined 117 patients who presented to the emergency department of Dicle University, Faculty of Medicine, after a blast injury between January 2005 and September 2013 and met the inclusion criteria. (Table 1, Table 2, Table 3, Table 4)
Table 1.
Demographic properties by sex of the patients
| Demographic property | Male n=100 (85.5%) |
Female n=17 (14.5%) |
Total n=117 |
|||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Age (Years: Mean+SD) | 23.50+13.47 | 20.1 | 8+09.44 | 23.02+12.98 | ||
| Place of residence | ||||||
| Town | 44 | 37.60 | 11 | 9.40 | 55 | 47.01 |
| Village | 27 | 23.08 | 1 | 0.85 | 28 | 23.93 |
| Country | 23 | 19.66 | 5 | 4.27 | 28 | 23.93 |
| Abroad | 6 | 5.12 | — | — | 6 | 5.12 |
| Occupation | ||||||
| student | 37 | 31.62 | 5 | 4.27 | 42 | 35.90 |
| Other* | 26 | 22.22 | 11 | 9.40 | 37 | 31. 62 |
| Farmer | 24 | 20.51 | 1 | 0.85 | 25 | 21.36 |
| Driver | 7 | 5.98 | — | — | 7 | 5.98 |
| Shepherd | 6 | 5.12 | — | — | 6 | 5.12 |
| Site of incident | ||||||
| City center | 57 | 48.72 | 16 | 13.67 | 73 | 62.39 |
| Rural area | 36 | 30.77 | 1 | 0.85 | 37 | 31.62 |
| Abroad | 7 | 5.98 | — | — | 7 | 5.98 |
| Type of explosive | ||||||
| Bomb | 32 | 27.35 | 2 | 1.71 | 34 | 29.06 |
| Mine | 21 | 17.95 | 3 | 2.56 | 24 | 20.51 |
| Other** | 24 | 20.51 | 9 | 7.69 | 33 | 28.21 |
| Squib | 14 | 11.97 | 3 | 2.56 | 17 | 14.53 |
| Dynamite | 9 | 7.69 | — | — | 9 | 7.69 |
Other: Craftsmen (n=17), children <7 years of age (n=7), housewives (n=7), state officials (n=5), and workers (n=1);
Other: Improvised explosive device (n=14), shell casing explosion (n=6), propane cylinder explosion (n=3), Petroleum barrel explosion (n=2), Gas bomb (n=2), Firework explosion (n=1), Automobile LPG (liquefied petroleum gas) tank explosion (n=1), Lighter explosion (n=1), Pressure cooker explosion (n=1), vehicle power supply explosion (n=1), and Transformer explosion (n=1).
Table 2.
Distribution of patients by injured body parts
| Injured body part | Male n=100 (85.5%) |
Female n=17 (14.5%) |
Total n=117 |
|||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Extremity | 73 | 62.39 | 7 | 5.98 | 80 | 68.38 |
| Head and neck | 54 | 46.15 | 9 | 7.69 | 63 | 53.85 |
| Eyes only | 36 | 30.77 | 6 | 5.13 | 42 | 35.90 |
| Thorax | 15 | 12.82 | 4 | 3.42 | 19 | 16.24 |
| Penetrating | 9 | 7.69 | 3 | 2.56 | 12 | 10.26 |
| Lung only | 7 | 5.98 | 3 | 2.56 | 10 | 8.55 |
| Abdomen | 8 | 6.84 | 1 | 0.85 | 9 | 7.69 |
| Mild skin injury | 5 | 4.27 | 4 | 3.42 | 9 | 7.69 |
| Non-penetrating | 6 | 5.13 | 1 | 0.85 | 7 | 5.98 |
Table 3.
Distribution of the patients by the locations of amputation after explosion
| Location of amputation | Male n=100 |
Female n=17 |
Total n=117 |
|||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| None | 64 | 54.70 | 16 | 13.68 | 80 | 68.38 |
| upper extremity | 25 | 21.37 | 1 | 0.85 | 26 | 22.22 |
| Finger | 13 | 11.11 | 1 | 0.85 | 14 | 11.96 |
| Lower extremity | 11 | 9.40 | — | — | 11 | 9.40 |
| Wrist | 10 | 8.55 | — | — | 10 | 8.55 |
| Knee | 5 | 4.27 | — | — | 5 | 4.27 |
| Toe | 4 | 3.42 | — | — | 4 | 3.42 |
| shoulder | 1 | 0.85 | — | — | 1 | 0.85 |
| Ankle | 1 | 0.85 | — | — | 1 | 0.85 |
| Elbow | 1 | 0.85 | — | — | 1 | 0.85 |
| Hip | 1 | 0.85 | — | — | 1 | 0.85 |
Table 4.
Distribution of the patients by the clinic of admission
| Clinic of admission | Male n=100 |
Female n=17 |
Total n=117 |
|||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Emergency service | 23 | 19.66 | 7 | 5.98 | 30 | 25.64 |
| Orthopedics | 30 | 25.64 | — | — | 30 | 25.64 |
| Plastic surgery | 19 | 16.24 | 2 | 1.71 | 21 | 17.95 |
| Ophthalmology | 13 | 11.11 | 4 | 3.42 | 17 | 14.53 |
| Neurosurgery | 5 | 4.27 | 1 | 0.85 | 6 | 5.13 |
| Chest surgery | 3 | 2.56 | 3 | 2.56 | 6 | 5.13 |
| General surgery | 5 | 4.27 | — | — | 5 | 4.27 |
| Cardiovascular surgery | 2 | 1.71 | — | — | 2 | 1.71 |
The rate of dynamite explosions was 7.69%. Of these patients, 6.84% (n=8) were farmers. Dynamite-induced injuries affected significantly more farmers than any other occupation (p>0.05). Although statistically non-significant, some explosives affected particular worker classes more frequently, with shepherds being more affected by mines and dynamite and the majority of those injured by squibs were students (8.55%) and craftsmen (3.42%). The majority of our patients injured by bombs were students (11.97%) and craftsmen (6.84%).
Discussion
A total of 117 cases of blast injuries presented to our hospital within an eight year time period. The seemingly low number of cases is the result of inclusion of only civilians, because injured military personnel or members of illegal terrorist organizations are usually not brought to our hospital. In addition, victims that were killed at the site of incident or in an ambulance while being transported to the hospital were also excluded.1, 8
A review of the literature on injuries with explosive materials revealed that most victims were young males, while women, children, and the elderly were injured less frequently.9, 10, 11, 12, 13, 14 Our study similarly demonstrated that the victims of blast injuries were mostly young people and males. Land mines usually harm military personnel during wartime, whereas they primarily affect poor, rural people during peacetime. Thus, the weakest and poorest are the victims of these weapons.[5] Previous studies in the literature usually compared explosives and firearm injuries, or they provided information on a specific type of explosive material.1, 5, 15, 16 In a study from Cambodia that studied 863 firearm injuries, land mines were the cause of injuries in 37% of cases.[15] On the other hand, most of the victims in our study were injured by bombs or mines. In rural areas, dynamite injuries also existed along with mine injuries. This is because dynamite is commonly used in rural areas of our region for fishing in brooks or ponds.
Terrorist organizations generally target crowded public places and young people.1, 4, 11, 13, 16, 17 The primary goal of these attacks is to create a state of fear and chaos.1, 4, 17 The attacks usually have political motives and are performed for the interests of a religious or nationalist group.[4] A study performed in Israel revealed that 54% of people injured in explosions were injured in public places while 36% were injured in attacks to commercial buildings and main roads. Another study from Israel showed that most attacks targeted buses and bus routes.[9] In our study, blast injuries mostly occurred in public areas or by explosions due to victims manual handling explosive material. A study reported from Madrid, Spain revealed that explosions mostly occurred at the end of the business day and on the way home. It appears that such attacks usually target working class people.[16] However, students and farmers were injured most frequently in our study. Students were affected because explosions took place in city centers, in the vicinity of schools. Farmers, on the other hand, were affected by land mines.
Literature data suggest that the majority of explosions occur either in public transportation vehicles or crowded public places.1, 4, 16, 17 Husum et al. reported that injuries from land mine explosions primarily occurred in rural areas.[5] Although the majority of our patients were affected in city centers, land mine explosions occurred in rural areas. This indicates that our results were in agreement with literature data. Ron Golan et al. from Israel studied the distribution of body parts affected by explosion and found that the face, neck, thorax, and upper extremities were affected most.[9] In contrast, Karaca et al. reported that lower extremities were most commonly affected. Extremity injuries resulted in amputation in most cases.[18] The reasons for a higher rate of upper extremity injuries in the present study were manual handling of squibs and raking up discovered bombs and land mines. Not surprisingly, amputations mainly affected upper extremities, with hand and wrist regions being the most affected body parts.
The most important aspects of blast injuries include their economic burden on a society, high treatment costs, and patient difficulties during the rehabilitation process.7, 19, 20 Land mineassociated injuries require more hospital resources, an increased number of transfusion products and operations, and longer rehabilitation and reintegration processes.[21] As a result of high treatment costs, 85% of affected persons suffer financial problems.[22] A quarter of our patients were discharged after a 24-hour follow-up period in the emergency department. The remaining three quarters had extremity injuries or amputations and, as expected, were admitted to the departments of Orthopedics and Traumatology, Plastic, Eye, Reconstructive, and Aesthetic Surgery, or the intensive care unit.
Literature data suggest that explosions mostly occur in summer months.1, 4, 11, 13, 17 In our study, blast injuries most commonly occurred in July and August (Figure 1). Attacks with explosives are dependent on the internal dynamics of countries or regions. Therefore, it would be erroneous to reach a conclusion with regard to yearly distribution of explosions. In our region, due to shifts in the political climate, 2008 was the calmest year while 2012 had the highest number of explosions (Figure 2).
Figure 1.
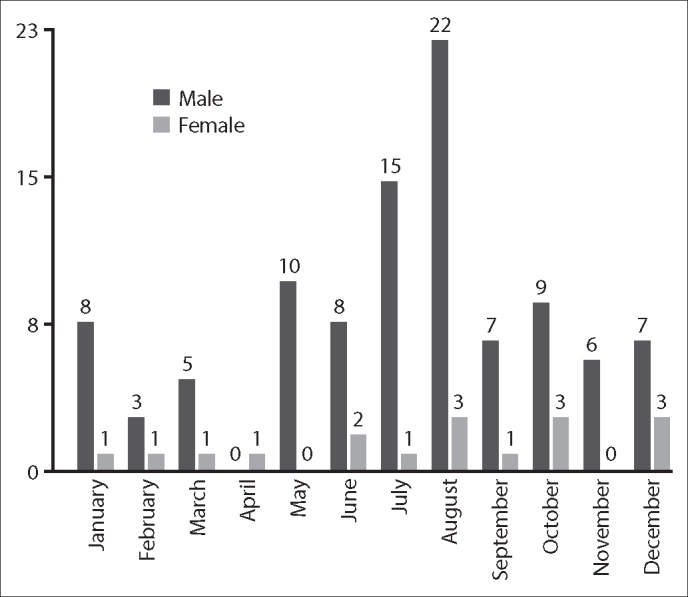
Distribution of patients by the month of incident.
Figure 2.
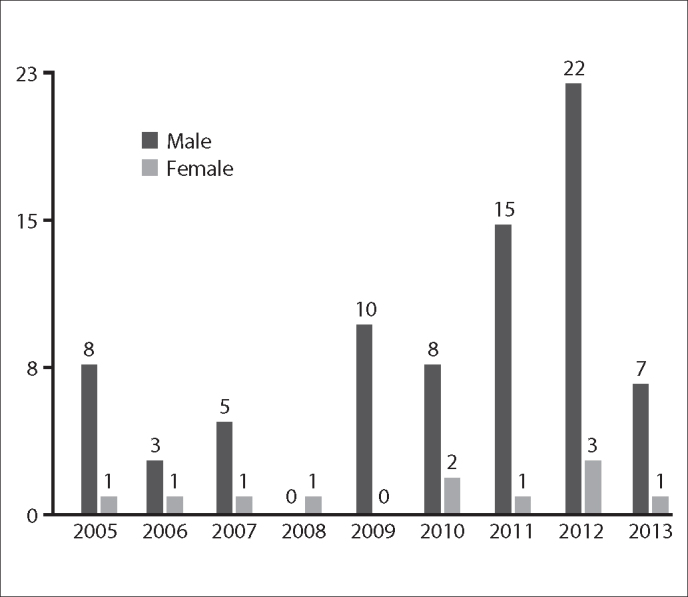
Distribution of the patients by years of presentation.
Many studies have reported that land mine explosions occur in rural areas.19, 20, 21 The majority of patients coming from rural areas were victims of land mine or dynamite explosions. Consequently, farmers were by far the most affected worker class. In non-rural regions, on the other hand, students led other social classes, most being injured by bombs and squibs.
Although mortality rates differ in individual studies, they have usually been high. Some studies reported that 35% to 50% of deaths occurred during the prehospital period due to delays in accessing healthcare.7, 22 Husum et al. reported a prehospital death rate of 75%.20, 21 They emphasized that with timely response and first aid performed by mobilized healthcare teams, the mortality rate could be reduced by half in four years. The mean mortality rates in different studies reportedly ranged from 36% to 52%.11, 21 In our study, only two patients died in the hospital. Among those who survived long enough to reach the hospital, the mortality rate was 1.7%. This rate was lower than previous studies, since patients who died at the site of incident or during transport were excluded. The mortality rate of those injured in mine explosions was 8.33%.
Limitations
Records of those who died at the site of incident or during transport and those referred to other hospitals could not be reached. We could not access the records of all patients with blast injuries and were missing some data about injury mechanisms. We do not know the exact number of these missing patients. Other limitations are the study's retrospective nature, the fact it was conducted in a single center, and the exclusion of military personnel.
Conclusion
In conclusion, blast injuries have high mortality and morbidity rates. Therefore, the number of trauma centers and emergency teams in the region should be increased. In addition, mined lands should be cleared of mines and the local community should be educated about explosives. Further large-scale studies will be beneficial to prevent future injuries and their sequelae. They will also aid in prevention of blast injuries and ensure correct triage, rapid intervention, and a multidisciplinary approach. Finally, they will prevent further workforce losses after blast injuries.
Conflict of Interest
The authors declare that there is no potential conflicts of interest.
Footnotes
Published online: February 18, 2015
References
- 1.Frykberg ER, Tepas JJ., 3rd Terrorist bombings. Lessons learned from Belfast to Beirut. Ann Surg. 1988;208:569–576. doi: 10.1097/00000658-198811000-00005. CrossRef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Eşsizoğlu A, Yaşan A, Bülbül I, Onal S, Yildirim EA, Aker T. Factors affecting the diagnosis of post-traumatic stress disorder after a terrorist attack. Turk Psikiyatri Derg. 2009;20:118–126. [Article in Turkish] [PubMed] [Google Scholar]
- 3.Klamkam P, Jaruchinda P, Nivatwongs S, Muninnobpamasa T, Harnchumpol P, Nirattisai S. Otologic manifestations from blast injuries among military personnel in Thailand. Am J Otolaryngol. 2013;34:287–291. doi: 10.1016/j.amjoto.2012.12.007. CrossRef. [DOI] [PubMed] [Google Scholar]
- 4.Mirza FH, Parhyar HA, Tirmizi SZ. Rising threat of terrorist bomb blasts in Karachi–a 5-year study. J Forensic Leg Med. 2013;20:747–751. doi: 10.1016/j.jflm.2013.04.014. CrossRef. [DOI] [PubMed] [Google Scholar]
- 5.Jahunlu HR, Husum H, Wisborg T. Mortality in land-mine accidents in Iran. Prehosp Disaster Med. 2002;17:107–109. doi: 10.1017/s1049023x00000261. [DOI] [PubMed] [Google Scholar]
- 6.Andersson N, da Sousa CP, Paredes S. Social cost of land mines in four countries: Afghanistan, Bosnia, Cambodia, and Mozambique. BMJ. 1995;311:718–721. doi: 10.1136/bmj.311.7007.718. CrossRef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Husum H, Gilbert M, Wisborg T, Van Heng Y, Murad M. Land mine injuries: a study of 708 victims in North Iraq and Cambodia. Mil Med. 2003;168:934–940. [PubMed] [Google Scholar]
- 8.Coupland RM. The effect of weapons on health. Lancet. 1996;347:450–451. doi: 10.1016/s0140-6736(96)90017-3. CrossRef. [DOI] [PubMed] [Google Scholar]
- 9.Golan R, Soffer D, Givon A, Peleg K. The ins and outs of terrorist bus explosions: injury profiles of onboard explosions versus explosions occurring adjacent to a bus. Injury. 2014;45:39–43. doi: 10.1016/j.injury.2013.02.004. CrossRef. [DOI] [PubMed] [Google Scholar]
- 10.Pyper PC, Graham WJ. Analysis of terrorist injuries treated at Craigavon Area Hospital, Northern Ireland, 1972-1980. Injury. 1983;14:332–338. doi: 10.1016/0020-1383(83)90250-4. CrossRef. [DOI] [PubMed] [Google Scholar]
- 11.Aharonson-Daniel L, Waisman Y, Dannon YL, Peleg K, Members of the Israel Trauma Group Epidemiology of terror-related versus non-terror-related traumatic injury in children. Pediatrics. 2003;112:e280. doi: 10.1542/peds.112.4.e280. CrossRef. [DOI] [PubMed] [Google Scholar]
- 12.Yavuz MS, Asirdizer M, Cetin G, Yavuz MF, Cansunar FN, Kolusayin RO. Deaths due to terrorist bombings in Istanbul (Turkey) J Clin Forensic Med. 2004;11:308–315. doi: 10.1016/j.jcfm.2004.06.002. CrossRef. [DOI] [PubMed] [Google Scholar]
- 13.Bilukha OO, Becknell K, Laurenge H, Danee L, Subedi KP. Fatal and non-fatal injuries due to intentional explosions in Nepal, 2008-2011: analysis of surveillance data. Confl Health. 2013;7:5. doi: 10.1186/1752-1505-7-5. CrossRef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Centers for Disease Control and Prevention (CDC) Homemade chemical bomb incidents - 15 states, 2003-2011. MMWR Morb Mortal Wkly Rep. 2013;62:498–500. [PMC free article] [PubMed] [Google Scholar]
- 15.Meddings DR, O'Connor SM. Circumstances around weapon injury in Cambodia after departure of a peacekeeping force: prospective cohort study. BMJ. 1999;319:412–415. doi: 10.1136/bmj.319.7207.412. CrossRef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Turégano-Fuentes F, Caba-Doussoux P, Jover-Navalón JM, Martín-Pérez E, Fernández-Luengas D, Díez-Valladares L. Injury patterns from major urban terrorist bombings in trains: the Madrid experience. World J Surg. 2008;32:1168–1175. doi: 10.1007/s00268-008-9557-1. CrossRef. [DOI] [PubMed] [Google Scholar]
- 17.Mayo A, Kluger Y. Terrorist bombing. World J Emerg Surg. 2006;1:33. doi: 10.1186/1749-7922-1-33. CrossRef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Karaca MA, Erbil B, Karakılıç E, Kunt MM, Kavalcı C, Akpınar E. “Evaluation of Injuries Due to a Terrorist Bombing in Ankara, 20 September 2011”. Eur J Surg Sci. 2014;5:20–26. [Google Scholar]
- 19.Aharonson-Daniel L, Peleg K ITG. The epidemiology of terrorism casualties. Scand J Surg. 2005;94:185–190. doi: 10.1177/145749690509400302. [DOI] [PubMed] [Google Scholar]
- 20.Jeffrey SJ. Antipersonnel mines: who are the victims? J Accid Emerg Med. 1996;13:343–346. doi: 10.1136/emj.13.5.343. CrossRef. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Husum H, Resell K, Vorren G, Heng YV, Murad M, Gilbert M. Chronic pain in land mine accident survivors in Cambodia and Kurdistan. Soc Sci Med. 2002;55:1813–1816. doi: 10.1016/s0277-9536(01)00315-x. CrossRef. [DOI] [PubMed] [Google Scholar]
- 22.Ascherio A, Biellik R, Epstein A, Snetro G, Gloyd S, Ayotte B. Deaths and injuries caused by land mines in Mozambique. Lancet. 1995;346:721–724. doi: 10.1016/s0140-6736(95)91501-x. CrossRef. [DOI] [PubMed] [Google Scholar]