

Abstract
Background:
China has not established social security system for rare diseases. Rare diseases could easily impoverish patients and their families. Little research has studied the equity and accessibility of health services for patients with rare diseases in China. This study aimed to explore the factors that influence health expenditure of rare diseases and evaluate its equity.
Methods:
Questionnaire survey about living conditions and cost burden of patients with rare diseases was conducted. Individual and family information, health expenditure and reimbursement in 2014 of 982 patients were collected. The impact of medical insurance, individual sociodemographic characteristics, family characteristics, and healthcare need on total and out-of-pocket (OOP) health expenditures was analyzed through the generalized linear model. Equity of health expenditure was evaluated by both concentration index and Lorenz curve.
Results:
Of all the surveyed patients, 11.41% had no medical insurance and 92.10% spent money to seek medical treatment in 2014. It was suggested female (P = 0.048), over 50 years of age (P = 0.062), high-income group (P = 0.021), hospitalization (P = 0.000), and reimbursement ratio (RR) (P = 0.000) were positively correlated with total health expenditure. Diseases not needing long-term treatment (P = 0.000) was negatively correlated with total health expenditure. Over 50 years of age (P = 0.065), high-income group (P = 0.018), hospitalization (P = 0.000) and having Urban Employee Basic Medical Insurance (UEBMI) (P = 0.022) were positively correlated with OOP health expenditure. Patient or the head of the household having received higher education (P = 0.044 and P = 0.081) and reimbursement ratio (P = 0.078) were negatively correlated with OOP health expenditure. The equity evaluation found concentration indexes of health expenditure before and after reimbursement were 0.0550 and 0.0539, respectively.
Conclusions:
OOP health expenditure of patients with UEBMI was significantly more than that of patients without medical insurance. However, for any other medical insurance, there was no difference between OOP health expenditure of the insured patients and patients without insurance. The current reimbursement policies have increased the equity of health expenditure, but are biased toward high-income people.
Keywords: Determinant, Equity Evaluation, Health Expenditure, Rare Disease
INTRODUCTION
Rare diseases are the diseases with a very low prevalence. The standard of rare diseases varies across countries.[1] World Health Organization defines rare diseases as the diseases of which the prevalence is 0.65−1%. Since 1980, some developed countries and regions have issued laws, regulations and supporting policies concerning rare diseases and orphan drugs to protect health right and interest of patients with the rare diseases.[2] The mature management system for rare diseases has improved the accessibility of orphan drugs and reduced the burden on patients. China has not established social security system for rare diseases yet. Rare diseases could easily impoverish the patients and their families.
The health expenditure of rare diseases is generally expensive, so exploring its determinants is important for policy makers. Many studies on policy evaluation of rare diseases and orphan drugs have been conducted, while little focused on the patient group. Disease burden of inherited ichthyosis, Duchenne and Becker muscular dystrophies, etc., in European Union, Australia and some other regions has been investigated.[3,4,5] One study applied catastrophic and impoverishment expenditure to evaluate the affordability of five rare diseases in China.[6] You and Kobayashi[7] have explored determinants of out-of-pocket (OOP) health expenditure using data from China Health and Nutrition Survey.
This study will focus on the entire rare disease patient group, present a detailed analysis of the total and OOP health expenditures on rare diseases and explore their determinants. On this basis, the study also evaluated the equity of rare disease health expenditure for sampled patients.
China has gradually brought rare diseases and orphan drugs into national planning, a national experts committee of diagnosis and security of rare disease has just established, so the study could provide a prospective reference for policy making.
METHODS
Data
The study collected information about living conditions and cost burden of patients with rare diseases through online questionnaire, which had been designed based on Andersen's Behavioral Model.[8] Information collected included individual demographic and socioeconomic background, household characteristics, type of medical insurance, utilization of curative healthcare services in 2014, total and OOP health expenditures for rare diseases in 2014, reimbursement rate (RR), self-reported health status, perceived severity of illness, etc. To get curative healthcare utilization, patients or their parents were asked whether any therapy was utilized.
There was no official registration system for rare disease patients in China. Neither was survey and database for them. However, many patients voluntarily joined in patient mutual aid organizations. We cooperated with Chinese Organization for Rare Disorders, one nongovernmental organizations in China, to contact the registered rare disease patients or their families. From May to July in 2015, we made contact with over 1500 patients or their families through telephone and sent the questionnaire to them through email and text message. Up to the end of September 2015, we received 1029 questionnaires (response rate 67.30%), of which 982 were valid (validity rate 95.40%). The surveyed patients were from all over the country, and various rare diseases were involved. To ensure data validity, we randomly chose 10% of the surveyed patients and called them back in October 2015. The answers of these patients for the questions were consistent with the online data, which indicated the data from the online survey was reliable. The database of our study was built with the standardized data.
Study variables
Most patients with rare diseases need lifelong treatment, so health expenditure in one year was taken as the index. Total health expenditure and OOP health expenditure for rare diseases in 2014 were obtained from the questionnaires and taken as the dependent variables. Total health expenditure included spending on consultations, tests, and medicines, and additional payments related to the treatment for the rare diseases while OOP health expenditure was net of any reimbursement that patients have received or expect to receive from their medical insurance programs.
In Andersen's Behavioral Model, the factors that determine demand for healthcare fall into three categories: predisposing, enabling and need variables.[9] Following this model and based on the survey data, we classified gender, age, marital status, and household head as predisposing factors; education, employment, urban/rural, household size, household income and medical insurance status as enabling factors; and perceived severity of illness and self-reported health status as need factors. The description and descriptive statistics of dependent and independent variables are shown in Supplement Table 1.
Supplement Table 1.
Description and descriptive statistics of dependent and independent variables (n=982)
| Independent variable | Sample size, n (%) | Description |
|---|---|---|
| Individual characteristics | ||
| Gender | ||
| Male (reference) | 593 (60.39) | = 0 if male |
| Female | 389 (39.61) | = 1 if female |
| Age | ||
| 0–20 years (reference) | 581 (59.16) | |
| 21–30 years | 156 (15.89) | = 1 if 21–30, = 0 otherwise |
| 31–40 years | 139 (14.15) | = 1 if 31–40, = 0 otherwise |
| 41–50 years | 66 (6.72) | = 1 if 41–50, = 0 otherwise |
| ≥51 years | 40 (4.07) | = 1 if ≥51, = 0 otherwise |
| Marital status | ||
| Unmarried (reference) | 758 (77.19) | = 0 if unmarried |
| Married | 224 (22.81) | = 1 if married |
| Education status | ||
| Primary school or below (reference) | 550 (56.01) | |
| Junior and senior school | 224 (22.81) | = 1 if junior or senior school, = 0 if otherwise |
| College degree or above | 208 (21.18) | = 1 if college degree or above, = 0 if otherwise |
| School/employment status | ||
| Student and preschool children (reference) | 539 (54.89) | |
| Employed and unemployed with employability | 215 (21.89) | = 1 if employed or unemployed with employability, = 0 if otherwise |
| Employment inability and retired | 228 (23.22) | = 1 if employment inability or retired, = 0 if otherwise |
| Medical insurance | ||
| No health insurance (reference) | 112 (11.41) | |
| UEBMI | 196 (19.96) | = 1 if UEBMI, = 0 otherwise |
| URBMI | 251 (25.56) | = 1 if URBMI, = 0 otherwise |
| NRCMS | 411 (41.85) | = 1 if NRCMS, = 0 otherwise |
| Government insurance | 12 (1.22) | = 1 if government insurance, = 0 otherwise |
| Severity of disease | ||
| Needing long-term treatment (reference) | 896 (91.24) | = 0 if needing long-term treatment |
| No needing long-term treatment | 86 (8.76) | = 1 if no needing long-term treatment |
| Provincial hospital for diagnosis or not | ||
| No (reference) | 202 (20.57) | = 0 if no |
| Yes | 780 (79.43) | = 1 if yes |
| Municipal hospital for diagnosis or not | ||
| No (reference) | 797 (81.16) | = 0 if no |
| Yes | 185 (18.84) | = 1 if yes |
| Outpatient visit or not | ||
| No (reference) | 524 (53.36) | = 0 if no |
| Yes | 458 (46.64) | = 1 if yes |
| Hospitalization or not | ||
| No (reference) | 617 (62.83) | = 0 if no |
| Yes | 365 (37.17) | = 1 if yes |
| Health status | ||
| Good or excellent (reference) | 130 (13.24) | |
| Fair | 371 (37.78) | = 1 if fair, = 0 otherwise |
| Poor or terrible | 481 (48.98) | = 1 if poor or terrible, = 0 otherwise |
| Household characteristics | ||
| Income level (based on annual household income) | ||
| Lowest 20% (reference) | 197 (20.06) | |
| Lower 20% | 196 (19.96) | = 1 if lower 20, = 0 otherwise |
| Middle 20% | 196 (19.96) | = 1 if middle 20, = 0 otherwise |
| Richer 20% | 196 (19.96) | = 1 if richer 20, = 0 otherwise |
| Richest 20% | 197 (20.06) | = 1 if richest 20, = 0 otherwise |
| Education status of household head | ||
| Primary school or below (reference) | 149 (15.17) | Reference |
| Junior and senior school | 492 (50.1) | = 1 if junior or senior school, = 0 if otherwise |
| College degree or above | 341 (34.73) | = 1 if college degree or above, = 0 if otherwise |
| Household size (capita) | ||
| 1–3 (reference) | 392 (39.92) | |
| 4–5 | 465 (47.35) | = 1 if 4–5, = 0 if otherwise |
| ≥6 | 125 (12.73) | = 1 if≥6, = 0 if otherwise |
| Household living status | ||
| Below the minimum living standard (reference) | 182 (18.53) | = 0 if below the minimum living standard |
| Above the minimum living standard | 800 (81.47) | = 1 if above the minimum living standard |
| Regional characteristics | ||
| Urban (reference) | 579 (58.96) | = 0 if urban |
| Rural | 403 (41.04) | = 1 if rural |
| Dependent variables | Expenditure (RMB Yuan), median (IQR) | Description |
| Y1: Total health expenditure for rare disease in 2014 | 20,000 (33,500) | Incurred when seeking care through self-medication or going for health services |
| Y2: OOP health expenditure for rare disease in 2014 | 17,000 (24,000) | Total health expenditure net of any reimbursement |
UEBMI: Urban Employee Basic Medical Insurance; URBMI: Urban Resident Basic Medical Insurance; NRCMS: New Rural Cooperative Medical Scheme; OOP: Out-of-pocket; IQR: Interquartile range.
Some independent variables were divided into groups. Age was categorized into five groups while it may have no linear relationship with health expenditure. Marital status was divided into two groups, married and unmarried (including single, divorced, and widowed). Medical insurance was categorized according to the situation of China, including Urban Employee Basic Medical Insurance (UEBMI) for most employees, Urban Resident Basic Medical Insurance (URBMI) for urban residents, New Rural Cooperative Medical Scheme (NRCMS) for rural residents and government insurance which mainly for government employees. Hospital type for diagnosis and whether long-term treatment was needed were uses to indicate disease severity. Use of health service was represented by whether there was outpatient visit or hospitalization in 2014.
Statistical analysis
Of the sampled patients, 78 did not have total and OOP health expenditures. Since our study focused on RR, the 78 patients were dropped in the analysis. First, one-way analysis of variance (ANOVA) was applied to analyze the total and OOP health expenditures of patients across different gender, age, education, and self-reported health status groups. Wilcoxon rank-sum test (gender analysis) and Kruskal-Wallis H test were used (other variables). The health expenditure did not fit normal distribution, and the effect of determinants might not possess linear additivity. Therefore, generalized linear model (GLM) was used to analyze the determinants of health expenditure. The model is shown as follows:
Y1i = g–1(ΣjXijαj+εj),
Y2i = g–1(ΣjXijβj+εj),

Where Y1 and Y2 was the total and OOP health expenditures of sampled patients. Xij was matrix of independent variable, α and β were corresponding parameters to be estimated, εj and Σj represented the error terms. Moreover, g (x) was the link function for the logarithmic transformation of the dependent variable, V (x) was the variance function, Φ was the dispersion parameters, ωi was the weight.
To further explore equity of health expenditure, we adopted the equity assessment methods used in most studies.[10,11] Concentration indexes before and after the reimbursement, as well as Lorenz curve, were calculated. The concentration index was calculated as follow:

Where µ was mean of health expenditure, Hj and Nj indicated accessibility and sample population.
We used Stata® version 13.1 (StataCorp LP, College Station, TX, USA) to clear the original data. The descriptive analysis, GLM regression and equity evaluation were all performed in Stata® version 13.1. A P < 0.10 was considered statistically significant.
RESULTS
The descriptive statistics of total sample are presented in Supplement Table 1. A total of 982 patients were included in the analysis, of which 60.39% were male. The mean age of the sampled patients was 18.3 ± 16.2 years. Many rare diseases were pretty severe and 91.24% of the patients needed long-term treatment. Overall, 65.78% of the patients sought care from outpatient visit or hospitalization in 2014 and the others took other treatment or no treatment. All sampled patients reported the OOP health expenditure for rare diseases and reimbursement in survey, the median total and OOP health expenditures were RMB 20,000 Yuan (interquartile range [IQR] 33,500 Yuan) and RMB 17,000 Yuan (IQR 24,000 Yuan), with average RMB 58,120.3 Yuan and RMB 29,918.1 Yuan.
One-way analysis of variance
Results of one-way ANOVA showed total health expenditure of female patients was significantly higher than that of male patients (RMB 80,656.4 Yuan vs. RMB 51,270.1 Yuan, Z = −2.649, P = 0.0081) while no statistical difference was found for OOP health expenditure. Total health expenditure was significantly different across different age groups. Total health expenditures were the lowest for patients 31–40 years of age and the highest for patients 41–50 years of age (RMB 40,466.6 Yuan vs. RMB 107,263.8 Yuan, H = 10.959, P = 0.0270). A significant difference was also found in OOP health expenditure across different age groups. OOP health expenditures were the lowest for patients 41–50 years of age and the highest for patients over 51 years of age (RMB 23,103.5 Yuan vs. RMB 71,097.2 Yuan, H = 12.270, P = 0.0155). OOP health expenditure was significantly different across different education groups (H = 7.173, P = 0.0277), with OOP health expenditure of patients with college degree or above being the lowest. Moreover, results of Kruskal-Wallis H test showed there were significant differences in total and OOP health expenditures of patients with different self-reported health statuses. Both total and OOP health expenditures were the lowest for patients whose self-reported health was excellent and the highest for patients whose self-reported health was terrible (total health expenditure: RMB 24,146.7 Yuan vs. RMB 81,588.7 Yuan, H = 9.865, P = 0.0428; OOP health expenditure: RMB 21,866.7 Yuan vs. RMB 43,035.4 Yuan, H = 13.747, P = 0.0081).
Determinants of health expenditure
A total of 904 patients were included in the GLM analysis. Two models were built, with Model 1 and Model 2 taking total expenditure and OOP expenditure for rare diseases as the dependent variable, respectively. Table 1 presents the estimation results of GLM for health expenditure. The median total health expenditure was RMB 21,000 Yuan (IQR 38,000 Yuan) and RMB 20,000 Yuan (IQR 26,000 Yuan), with average RMB 63,135.1 Yuan and RMB 32,499.5 Yuan after reimbursement of these 904 patients.
Table 1.
Estimated coefficients of GLM for reported health expenditure (n=904)
| Independent variables | Total health expenditure | OOP health expenditure | ||||
|---|---|---|---|---|---|---|
| Coefficient | SD | P | Coefficient | SD | P | |
| Individual characteristics | ||||||
| Gender | ||||||
| Male (reference) | ||||||
| Female | 0.185 | 0.094 | 0.048 | 0.140 | 0.093 | 0.131 |
| Age | ||||||
| 0–20 years (reference) | ||||||
| 21–30 years | 0.031 | 0.265 | 0.906 | 0.149 | 0.260 | 0.567 |
| 31–40 years | –0.053 | 0.291 | 0.855 | 0.085 | 0.290 | 0.768 |
| 41–50 years | 0.113 | 0.317 | 0.723 | –0.023 | 0.324 | 0.942 |
| ≥51 years | 0.712 | 0.382 | 0.062 | 0.708 | 0.384 | 0.065 |
| Marital status | ||||||
| Unmarried (reference) | ||||||
| Married | –0.257 | 0.177 | 0.146 | –0.194 | 0.179 | 0.280 |
| Education status | ||||||
| Primary school or below (reference) | ||||||
| Junior and senior school | 0.028 | 0.176 | 0.874 | –0.257 | 0.196 | 0.189 |
| College degree or above | –0.238 | 0.225 | 0.290 | –0.481 | 0.239 | 0.044 |
| School/employment status | ||||||
| Student and preschool children (reference) | ||||||
| Employed and unemployed with employability | –0.502 | 0.244 | 0.039 | –0.342 | 0.242 | 0.157 |
| Employment inability and retired | –0.065 | 0.219 | 0.768 | 0.035 | 0.217 | 0.873 |
| Medical insurance | ||||||
| No health insurance (reference) | ||||||
| UEBMI | 0.239 | 0.201 | 0.236 | 0.471 | 0.205 | 0.022 |
| URBMI | –0.110 | 0.159 | 0.486 | –0.068 | 0.162 | 0.673 |
| NRCMS | –0.067 | 0.153 | 0.662 | –0.027 | 0.152 | 0.857 |
| Government insurance | –0.174 | 0.432 | 0.688 | 0.074 | 0.430 | 0.863 |
| Critical illness insurance covering status | ||||||
| Covering (reference) | ||||||
| No covering | 0.184 | 0.217 | 0.397 | 0.138 | 0.218 | 0.527 |
| Reimbursement rate | 2.615 | 0.181 | 0.000 | –0.381 | 0.216 | 0.078 |
| Severity of disease | ||||||
| Needing long-term treatment (reference) | ||||||
| No needing long-term treatment | –0.635 | 0.175 | 0.000 | –0.461 | 0.177 | 0.009 |
| Provincial hospital for diagnosis or not | ||||||
| No (reference) | ||||||
| Yes | –0.131 | 0.116 | 0.258 | –0.168 | 0.115 | 0.144 |
| Municipal hospital for diagnosis or not | ||||||
| No (reference) | ||||||
| Yes | –0.426 | 0.361 | 0.238 | –0.507 | 0.359 | 0.158 |
| Outpatient visit or not | ||||||
| No (reference) | ||||||
| Yes | –0.083 | 0.093 | 0.372 | –0.130 | 0.093 | 0.162 |
| Hospitalization or not | ||||||
| No (reference) | ||||||
| Yes | 0.406 | 0.093 | 0.000 | 0.578 | 0.092 | 0.000 |
| Health status | ||||||
| Good or excellent (reference) | ||||||
| Fair | –0.075 | 0.140 | 0.595 | 0.032 | 0.141 | 0.823 |
| Poor or terrible | 0.040 | 0.139 | 0.776 | 0.120 | 0.139 | 0.388 |
| Household characteristics | ||||||
| Income level (based on annual household income) | ||||||
| Lowest 20% (reference) | ||||||
| Lower 20% | –0.113 | 0.145 | 0.435 | –0.147 | 0.143 | 0.305 |
| Middle 20% | 0.038 | 0.149 | 0.797 | 0.080 | 0.147 | 0.588 |
| Richer 20% | 0.090 | 0.151 | 0.552 | 0.138 | 0.147 | 0.350 |
| Richest 20% | 0.385 | 0.167 | 0.021 | 0.391 | 0.165 | 0.018 |
| Education status of household head | ||||||
| Primary school or below (reference) | ||||||
| Junior and senior school | –0.085 | 0.131 | 0.519 | –0.169 | 0.132 | 0.202 |
| College degree or above | –0.185 | 0.153 | 0.227 | –0.274 | 0.157 | 0.081 |
| Household size (capita) | ||||||
| 1–3 (reference) | ||||||
| 4–5 | –0.013 | 0.100 | 0.897 | 0.018 | 0.101 | 0.860 |
| ≥6 | –0.114 | 0.152 | 0.451 | –0.143 | 0.151 | 0.345 |
| Household living status | ||||||
| Below the minimum living standard (reference) | ||||||
| Above the minimum living standard | 0.015 | 0.126 | 0.907 | –0.063 | 0.124 | 0.611 |
| Regional characteristics | ||||||
| Urban (reference) | ||||||
| Rural | 0.082 | 0.122 | 0.501 | 0.098 | 0.122 | 0.420 |
GLM: Generalized linear model; OOP: Out-of-pocket; UEBMI: Urban Employee Basic Medical Insurance; URBMI: Urban Resident Basic Medical Insurance; NRCMS: New Rural Cooperative Medical Scheme; SD: Standard deviation.
Model 1 showed the factors that influenced total health expenditure. Of the individual characteristics, total health expenditure of female patients was more than that of male patients (Z = 1.98, correlation coefficient [CC] = 0.185, 95% confidence interval [CI] = 0.002–0.369, P = 0.048). Compared with patients 0–20 years of age, health expenditure of patients over 50 years of age was more (Z = 1.87, CC = 0.712, 95% CI = −0.036–1.459, P = 0.062), but the differences between other age groups and the reference group (0–20 years of age) were not statistically significant. Total health expenditure was also influenced by employment status. Total health expenditure of patients with employability was less than that of the student and preschool children (Z = −2.06, CC = −0.502, 95% CI = −0.980–−0.025, P = 0.039), while impact of employment inability and retirement on total health expenditure was not significant. Among household characteristics, total health expenditure of patients belonging to the richest 20% group was significantly more than that of patients belonging to the lowest 20% group (Z = 2.31, CC = 0.385, 95% CI = 0.059–0.711, P = 0.021). Effects of other income groups were similar to the reference group. Patients who did not need long-term treatment spent less (Z = −3.63, CC = −0.635, 95% CI = −0.978–−0.292, P = 0.000). Total health expenditure of patients who sought health care from hospitalization was more than that of patients with any other treatment (Z = 4.38, CC = 0.406, 95% CI = 0.224–0.587, P = 0.000). With patients under no health insurance as reference, the effects of all the medical insurances, including UEBMI, URBMI, NRCMS and government insurance, were not statistically significant. Moreover, whether the rare diseases were covered by critical illness insurance had no significant influence on total health expenditure. Taking RR into consideration, the higher RR was, the more total health expenditure was (Z = 14.47, CC = 2.615, 95% CI = 2.260–2.969, P = 0.000).
Model 2 took reimbursement into consideration and took OOP health expenditure as the dependent variable. Different from Model 1, gender had no significant influence on OOP health expenditure. The effect of age was similar to Model 1. OOP health expenditure of patients over 50 years of age was significantly more (Z = 1.84, CC = 0.708, 95% CI = −0.045–1.462, P = 0.065). There was no statistically significant difference between other age groups and the reference group (0–20 years of age). OOP health expenditure of patients with college degree or above was lower than that of patient with primary school or below (Z = −2.01, CC = −0.481, 95% CI = −0.950 to −0.012, P = 0.044), whereas no significant effect was found compared with junior and senior school group. OOP health expenditure of patients belonging to the richest 20% group was more (Z = 2.37, CC = 0.391, 95% CI = 0.068–0.713, P = 0.018). Education of the household head being college degree or above decreased the OOP health expenditure (Z = −1.75, CC = −0.274, 95% CI = −0.581–0.034, P = 0.081). Effect of disease severity and use of health service were consistent with Model 1. OOP health expenditure of patients who did not need long-term treatment was significantly less (Z = −2.61, CC = −0.461, 95% CI = −0.807–−0.114, P = 0.009); OOP health expenditure of patients who sought health care from hospitalization was more than that of patients with any other treatment (Z = 6.26, CC = 0.578, 95% CI = 0.397–0.759, P = 0.000). Compared with OOP health expenditure of patients without health insurance, OOP health expenditure of patients under UEBMI was higher (Z = 2.29, CC = 0.471, 95% CI = 0.068–0.873, P = 0.022), and OOP health expenditure of patients with other medical insurances were not significantly different. The higher RR was, the less OOP health expenditure was (Z = −1.76, CC = −0.381, 95% CI = −0.805–0.043, P = 0.078).
Equity evaluation
We found that concentration indexes of health expenditures before and after reimbursement were 0.0550 and 0.0539, respectively. The concentration curves are shown in Figures 1 and 2. It was shown that health expenditures before and after reimbursement were higher than the line of equality from both figures. In addition, concentration indexes of health expenditures before and after reimbursement were both above zero, which indicated total and OOP health expenditures of rare diseases were mainly seen in high-income groups. This suggested that total and OOP health expenditures of patients in the high-income group were more than those of patients in the low-income group. The decrease of concentration index absolute value after reimbursement disclosed the equity of health expenditure was improved by reimbursement.
Figure 1.
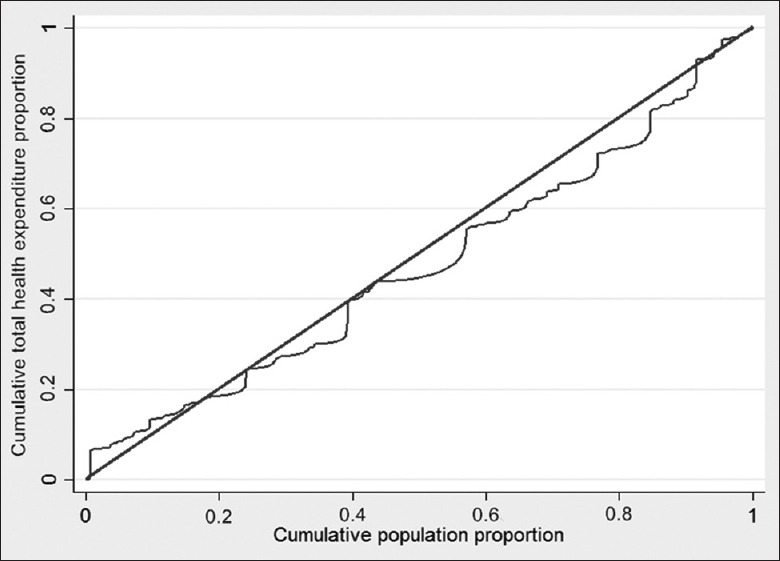
Concentration curve of total health expenditure for rare diseases.
Figure 2.
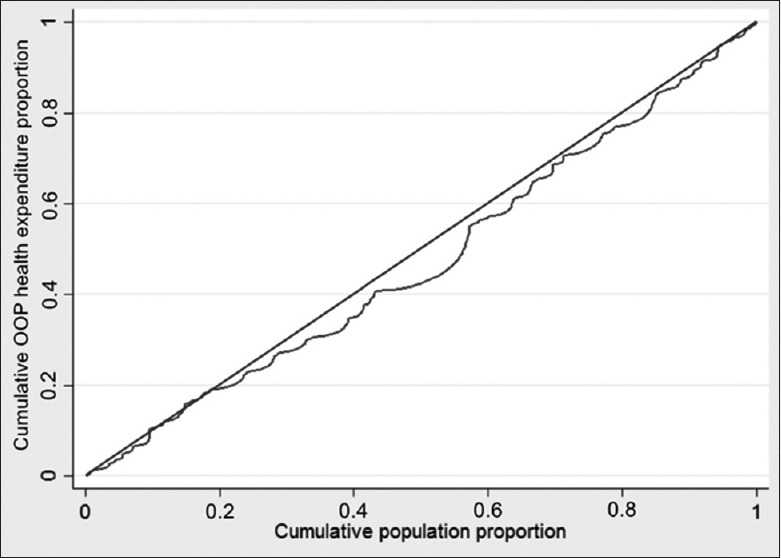
Concentration curve of OOP health expenditure for rare diseases. OOP: Out-of-pocket.
DISCUSSION
The result of our descriptive statistics showed characteristics of patients with rare diseases. We found that male patients accounted for most of the sampled patients, which might be because most rare diseases are genetic disorders and some diseases are Y-linked inheritable diseases.[12] There were studies showing that life expectancy of patients with rare diseases was low and over 50% of patients with rare diseases were children. Overall, the mean age of the sampled patients was young, which was consistent with what was found in above studies. Most diseases of the sample were pretty severe, which were difficult to diagnose and treat.[13] We found that 79.43% of the sampled patients got the definite diagnosis in provincial hospitals and that almost all sampled patients needed long-term treatment.
Our results strongly suggested that predisposing, enabling and need factors work together to determine the amount of total and OOP health expenditures for rare diseases in China. The age of ≥51 years was an important contributor to the amount of health spending, which was consistent with other study on the population without rare diseases.[14] With medical advances and economic development, life expectancy of patients with rare diseases would gradually increase. Elderly population of rare diseases will bring challenges to the health system in China. There was no significant difference in total health expenditure among patients in different education groups. After reimbursement, patients with college degree or above paid less for rare disease healthcare, which might be explained by that patients with higher education usually live in developed regions and could enjoy better health insurance policies. Roy et al.[15] and You et al.[7] have conducted health service utilization studies in India and China, respectively, and have found the higher the income of the family was, the more they spent on health. We found total and OOP health expenditures of patients in the richest 20% group were significantly more than those of the lowest 20% group. Health expenditure of rare diseases was usually expensive, and the average OOP health expenditure of the sampled patients in 2014 was RMB 32,499.5 Yuan, much more than per capita annually disposable income in 2014 (RMB 20,167.1 Yuan).[16] We knew from the survey that many patients could not afford the expenditure so that they did not get necessary treatment, such as taking medicines less than doctors advised. This might be one of the reasons why health expenditure of patients in high-income groups was higher.
Several studies have identified self-reported health status as an important determinant of health expenditure.[17,18] However, we did not find a significant difference in total and OOP health expenditures between patients whose self-reported health status was good or excellent and the other patients. Self-reported health status was an important measurement index for healthcare need. Most rare diseases cannot be cured, almost all the sampled patients had healthcare need. Therapeutic effects are different across different rare diseases, for instance, some patients can lead a normal life as long as they stick to the standard of care.
Medical insurance programs are designed to decrease OOP health expenditure of patients through subsidizing payment, but we found the coefficient of UEBMI was significantly positive in Model 2. The funding and RR of UEBMI were the highest in China while the insured patients were urban employees. A possible explanation for this result was that patients under UEBMI had higher income and were more likely to afford the standard of care. Moreover, we found critical illness insurance did not reduce OOP health expenditure of patients with rare diseases. That was because only a few rare diseases are covered by critical illness insurance and the RR is rather low.
We could also evaluate the current medical insurance programs through concentration index. Concentration index dropped a little bit after reimbursement, which indicated that current reimbursement policies might increase equity of health expenditure of patients with rare diseases. The evaluation results of concentration index and concentration curves were consistent with our common sense, in that patients in high-income groups had stronger ability to pay for rare diseases treatment. However, the results of equity evaluation have shown that the current reimbursement policies were more inclined to high-income groups, which could be improved in future. There are several types of government-run medical insurance with different RR and ceiling in China and therein high-income groups often tend to receive better medical insurance programs.[19]
Our study had several limitations. Data were collected by questionnaire survey, in which OOP health expenditure and RR were all self-reported by patients, thus were subject to recall errors. Reimbursement policies vary in all cities in China. Although Chinese government now has not well established nation-level social security system for rare diseases, some cities have gradually included such diseases into the scope of medical insurance reimbursement. For instance, the RR for patients with certain rare diseases in Qingdao reaches up to 70% while patients in some other cities with the same disease cannot receive any reimbursement. Unfortunately, we did not include cities as a factor in our analysis since the samples available were limited. In addition, charity organizations in some districts may also make cash fund or drug donation to low-income patients, but our data did not allow us to identify this phenomenon.
Furthermore, China is planning to bring laws on rare diseases and orphan drugs and take action to build up a corresponding social security system. Patients with rare diseases in China are a group of huge number, but the accessibility of health service for them has yet to be improved. The current medical security system has not taken full account of patients with rare diseases, whose OOP payments with various types of medical insurance have shown no difference from those of patients without any medical insurance, and the OOP payments of patients with UEBMI turned out even higher. The accessibility and equity of health service for patients with rare diseases need to be improved.
Supplementary information is linked to the online version of the paper on the Chinese Medical Journal website.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Edited by: Xin Chen
REFERENCES
- 1.Liu BC, He L, He G, He Y. A cross-national comparative study of orphan drug policies in the United States, the European Union, and Japan: Towards a made-in-China orphan drug policy. J Public Health Policy. 2010;31:407–20. doi: 10.1057/jphp.2010.30. doi: 10.1057/jphp.2010.30. [DOI] [PubMed] [Google Scholar]
- 2.Gong SW, Jin S. Current progress in the management of rare diseases and orphan drugs in China. Intractable Rare Dis Res. 2012;1:45–52. doi: 10.5582/irdr.2012.v1.2.45. doi: 10.5582/irdr.2012.v1.2.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dufresne H, Hadj-Rabia S, Méni C, Sibaud V, Bodemer C, Taïeb C. Family burden in inherited ichthyosis: Creation of a specific questionnaire. Orphanet J Rare Dis. 2013;8:73–83. doi: 10.1186/1750-1172-8-28. doi: 10.1186/1750-1172-8-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schreiber-Katz O, Klug C, Thiele S, Schorling E, Zowe J, Reilich P, et al. Comparative cost of illness analysis and assessment of health care burden of Duchenne and Becker muscular dystrophies in Germany. Orphanet J Rare Dis. 2014;9:210. doi: 10.1186/s13023-014-0210-9. doi: 10.1186/s13023-014-0210-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hime NJ, Fitzgerald D, Robinson P, Selvadurai H, Van Asperen P, Jaffé A, et al. Childhood interstitial lung disease due to surfactant protein C deficiency: Frequent use and costs of hospital services for a single case in Australia. Orphanet J Rare Dis. 2014;9:36. doi: 10.1186/1750-1172-9-36. doi: 10.1186/1750-1172-9-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Xin XX, Guan XD, Shi LW. Research on rare disease security mechanism in China based on the affordability evaluation of 5 rare diseases. China Pharm. 2014;25:404–7. doi: 10.6039/j.issn.1001-0408.2014.05.07. [Google Scholar]
- 7.You X, Kobayashi Y. Determinants of out-of-pocket health expenditure in China: Analysis using China health and nutrition survey data. Appl Health Econ Health Policy. 2011;9:39–49. doi: 10.2165/11530730-000000000-00000. doi: 10.2165/11530730-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 8.Kehrer BH, Andersen R, Glaser WA. A behavioral model of families’ use of health services. J Hum Resour. 1972;7:125–127. doi: 10.2307/145064. [Google Scholar]
- 9.Aday LA, Andersen R. A framework for the study of access to medical care. Health Serv Res. 1974;9:208–20. [PMC free article] [PubMed] [Google Scholar]
- 10.Goddard M, Smith P. Equity of access to health care services: Theory and evidence from the UK. Soc Sci Med. 2001;53:1149–62. doi: 10.1016/s0277-9536(00)00415-9. doi: 10.1016/S0277-9536(00)00415-9. [DOI] [PubMed] [Google Scholar]
- 11.Zhou ZL, Gao JM, Zhou ZY, Yang XW, Xue QX. Effects of new rural cooperative medical scheme on the equity of health care utilization. Chin Health Econ. 2012;31:37–9. doi: 10.3969/j.issn.1003-0743.2012.04.010. [Google Scholar]
- 12.Stolk P, Willemen MJ, Leufkens HG. Rare essentials: Drugs for rare diseases as essential medicines. Bull World Health Organ. 2006;84:745–51. doi: 10.2471/blt.06.031518. doi: 10.2471/BLT.06.031518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Budych K, Helms TM, Schultz C. How do patients with rare diseases experience the medical encounter? Exploring role behavior and its impact on patient-physician interaction. Health Policy. 2012;105:154–64. doi: 10.1016/j.healthpol.2012.02.018. doi: 10.1016/j.healthpol.2012.02.018. [DOI] [PubMed] [Google Scholar]
- 14.Murphy JF, Hepworth JT. Age and gender differences in health services utilization. Res Nurs Health. 1996;19:323–9. doi: 10.1002/(SICI)1098-240X(199608)19:4<323::AID-NUR6>3.0.CO;2-K. doi: 10.1002/(SICI) 1098-240X(199608)19:4<323:AID-NUR6>3.0.CO; 2-K. [DOI] [PubMed] [Google Scholar]
- 15.Roy K, Howard DH. Equity in out-of-pocket payments for hospital care: Evidence from India. Health Policy. 2007;80:297–307. doi: 10.1016/j.healthpol.2006.03.012. doi: 10.1016/j.healthpol.2006.03.012. [DOI] [PubMed] [Google Scholar]
- 16.2015 Chinese Statistical Yearbook. Beijing: National Bureau of Statistics of China. 2015. [Last accessed on 2015 Dec 02]. Available from: http://www.stats.gov.cn/tjsj/ndsj/2015/indexch.htm .
- 17.Chou KL, Chi I. Factors associated with the use of publicly funded services by Hong Kong Chinese older adults. Soc Sci Med. 2004;58:1025–35. doi: 10.1016/s0277-9536(03)00275-2. doi: 10.1016/S0277-9536(03)00275-2. [DOI] [PubMed] [Google Scholar]
- 18.Fleishman JA, Cohen JW, Manning WG, Kosinski M. Using the SF-12 health status measure to improve predictions of medical expenditures. Med Care. 2006;44(5 Suppl):I54–63. doi: 10.1097/01.mlr.0000208141.02083.86. doi: 10.1097/01.mlr.0000208141.02083.86. [DOI] [PubMed] [Google Scholar]
- 19.Wang T, Yu BR, Yang F. Analysis on hospitalization expenditure and hospital day of diabetic patient with different type of medical insurance. Health Econ Res. 2013;2:52–3. doi: 10.3969/j.issn.1004-7778.2013.02.018. [Google Scholar]