

Abstract
Background:
The accuracy of three-dimensional (3D) reconstructions from cone-beam computed tomography (CBCT) has been particularly important in dentistry, which will affect the effectiveness of diagnosis, treatment plan, and outcome in clinical practice. The aims of this study were to assess the linear, volumetric, and geometric accuracy of 3D reconstructions from CBCT and to investigate the influence of voxel size and CBCT system on the reconstructions results.
Methods:
Fifty teeth from 18 orthodontic patients were assigned to three groups as NewTom VG 0.15 mm group (NewTom VG; voxel size: 0.15 mm; n = 17), NewTom VG 0.30 mm group (NewTom VG; voxel size: 0.30 mm; n = 16), and VATECH DCTPRO 0.30 mm group (VATECH DCTPRO; voxel size: 0.30 mm; n = 17). The 3D reconstruction models of the teeth were segmented from CBCT data manually using Mimics 18.0 (Materialise Dental, Leuven, Belgium), and the extracted teeth were scanned by 3Shape optical scanner (3Shape A/S, Denmark). Linear and volumetric deviations were separately assessed by comparing the length and volume of the 3D reconstruction model with physical measurement by paired t-test. Geometric deviations were assessed by the root mean square value of the imposed 3D reconstruction and optical models by one-sample t-test. To assess the influence of voxel size and CBCT system on 3D reconstruction, analysis of variance (ANOVA) was used (α = 0.05).
Results:
The linear, volumetric, and geometric deviations were −0.03 ± 0.48 mm, −5.4 ± 2.8%, and 0.117 ± 0.018 mm for NewTom VG 0.15 mm group; −0.45 ± 0.42 mm, −4.5 ± 3.4%, and 0.116 ± 0.014 mm for NewTom VG 0.30 mm group; and −0.93 ± 0.40 mm, −4.8 ± 5.1%, and 0.194 ± 0.117 mm for VATECH DCTPRO 0.30 mm group, respectively. There were statistically significant differences between groups in terms of linear measurement (P < 0.001), but no significant difference in terms of volumetric measurement (P = 0.774). No statistically significant difference were found on geometric measurement between NewTom VG 0.15 mm and NewTom VG 0.30 mm groups (P = 0.999) while a significant difference was found between VATECH DCTPRO 0.30 mm and NewTom VG 0.30 mm groups (P = 0.006).
Conclusions:
The 3D reconstruction from CBCT data can achieve a high linear, volumetric, and geometric accuracy. Increasing voxel resolution from 0.30 to 0.15 mm does not result in increased accuracy of 3D tooth reconstruction while different systems can affect the accuracy.
Keywords: Accuracy, Cone-beam Computed Tomography, Reconstruction, Tooth
INTRODUCTION
Since the 1990s, cone-beam computed tomography (CBCT) has been widely used to assess hard-tissue structures of the dentomaxillofacial region in clinical practice and research. Due to its reduced acquisition time, lower radiation doses, relatively small isotropic voxels, and high spatial resolution,[1,2,3,4] CBCT has been fundamentally replaced conventional computed tomography for most tasks in dentistry.[5,6]
In recent years, the rapid development of digital technology led to great upgrading in dental technology and comprehensive changes on oral health care equipment, such as CBCT. CBCT can provide information of root and bone without invasion. Gaining three-dimensional (3D) reconstruction models of teeth or bone from CBCT data is becoming increasingly more important in dentistry. For example, the 3D reconstruction teeth or bone model can help make the orthodontic treatment plan, construct individual appliances, and evaluate treatment results, especially to assess the root resorption caused by tooth movement in orthodontics. The 3D reconstruction teeth can be applied to quantitatively detect and measure the root resorption from a 3D reconstruction model.[7,8,9,10,11] In addition, the 3D reconstruction teeth or bone model can help design a custom-made root-analog implant for immediate implantation,[12] design a surgical guide for dental implant surgery,[13] and simulate and navigate an oral and maxillofacial surgery.[14] Using those models to aid in diagnosis, treatment planning, simulation, and outcome assessment will have a major impact on clinical practice in the near future and the accuracy of tooth or bone segmentation will affect the effectiveness of clinical practice. Therefore, the accuracy of 3D reconstructions from CBCT image data should be assessed.
Various factors possibly influence the accuracy of the 3D reconstruction, such as scanning system, field of view (FOV), examined objects, exposure time, tube voltage and amperage, and also spatial resolution defined by the voxel size.[15] In clinical practice, most CBCT parameters have been preestablished and cannot be adjusted. However, the limited factors, such as voxel size, scanner system, and FOV, might be adjusted by doctors for specific diagnostic tasks and these factors appear to be more important to clinical practice.
Most previous studies usually assessed the accuracy of linear, volumetric measurements on dry skulls,[16,17,18,19,20] which are not so closed to physiological state and clinical practice. On the other side, Liu et al.[21] have collected CBCT data from orthodontic patients; however, they only assessed the volumetric deviation with the extracted teeth.
In this study, CBCT data from patients who need tooth extraction for orthodontic purpose were used and the extracted teeth were collected. Linear, volumetric, and geometric accuracy of the 3D reconstruction models from CBCT were assessed and the influences of voxel size and scanner system on the accuracy of 3D reconstruction models from CBCT were also investigated.
METHODS
Sample preparation
Orthodontic patients with first or second premolar extracted in the Second Dental Center, Peking University School and Hospital of Stomatology, Beijing, China from 2014 to 2015 were included in this prospective clinical study. Patients were scanned before tooth extraction by NewTom VG CBCT scanner (Aperio Services, Verona, Italy) with voxel size of 0.15 mm or 0.30 mm or VATECH DCTPRO CBCT scanner (VATECH Co., Ltd., Korea) with voxel size of 0.30 mm prescribed by orthodontist. All extracted teeth were brushed under running water to remove adherent blood and cleaned of residual bone, soft tissue, and then preserved in 0.9% normal saline. Patient's teeth with metallic restorations, caries, resin fillings, or fraction were excluded. In total, fifty teeth of 18 patients (ranging from 14 to 31 years of age) were included in the sample and then assigned to three groups according to CBCT system and voxel size: NewTom VG 0.15 mm group, NewTom VG 0.30 mm group, and VATECH DCTPRO 0.30 mm group.
The estimated sample number was at least 15 teeth for each group and detailed information of the groups is shown in Table 1. The clinical study was approved by the Peking University School and Hospital of Stomatology Ethnics Committee (PKUSSIRB-201311105), and informed consent was obtained from each patient.
Table 1.
Detailed information of fifty teeth of 18 patients in three groups
| Groups | Sample numbers (teeth/patient) | Voxel size (mm) | FOV (cm) | Tube voltage (kV) | Tube current (mA) | ST (s) | ET (s) |
|---|---|---|---|---|---|---|---|
| NewTom VG 0.15 mm | 17/6 | 0.15 | Medium; 12×8 | 110 | 1–20 | 18 | 3.6 |
| NewTom VG 0.30 mm | 16/6 | 0.30 | Medium; 12×8 | 110 | 1–20 | 18 | 3.6 |
| VATECH DCTPRO 0.30 mm | 17/6 | 0.30 | Medium; 16×10 | 90 | 6 | 24 | 24 |
FOV: Field of view; ST: Scanning time; ET: Exposure time.
Tooth segmentation
Since there was no fully automatic segmentation method available as yet, we carried out a manual segmentation. CBCT data were exported in DICOM format and then imported into Materialise Mimics 18.0 (Mimics Innovation Suite18.0, Materialise Dental, Leuven, Belgium) [Figure 1]. First, a single threshold value was selected based on a local gray level value and image gradient to create a mask to segment the target tooth from the background. And then, we drew or erased the mask manually layer by layer on at least two orientations to segment the tooth. The pulp cavity of the tooth was filled. At last, we smoothed and adjusted the mask according to the tooth border using the “Contour Edit” in this software. After segmentation, the 3D triangle-based surface of each tooth was reconstructed in Stereo Lithography (STL) format.
Figure 1.
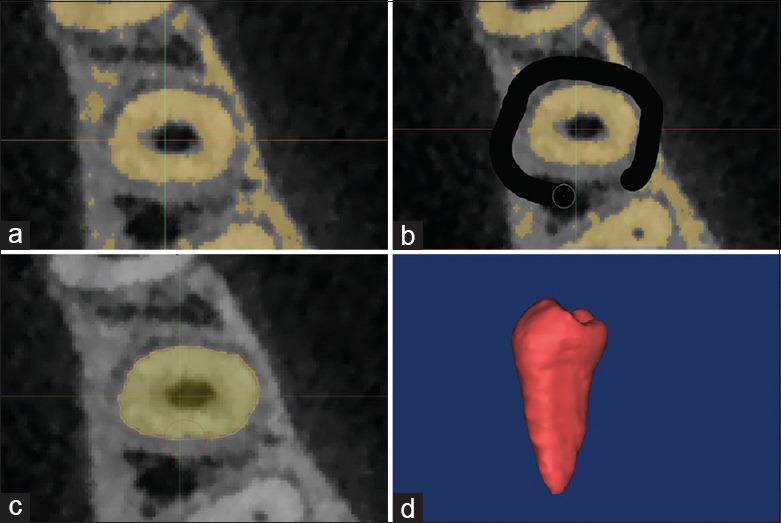
Manual tooth segmentation from CBCT image with Mimics 18.0. (a) Choose a threshold to create a mask to segment the interested tooth from the background. (b) Draw or erase the mask layer by layer to segment the tooth. (c) Smooth and adjust the mask according to the tooth border using the “Contour Edit”. (d) Export 3D reconstruction model in STL file. STL: Stereo Lithography; CBCT: Cone-beam computed tomography; 3D: Three-dimensional.
To test the reproducibility of tooth segmentation, 15 teeth were chosen randomly by casting lots to be segmented by another professional examiner using the same protocol above. Pearson correlation coefficients were used to determine the reliability of segmentation between the two examiners.
Linear deviation
The STL files of teeth were imported in Geomagic Qualify 2012 (Raindrop, USA). The length of tooth from the buccal cusp to the root apex (buccal root apex if with two roots) on the 3D reconstruction model was measured. The tooth length was also measured on the corresponding extracted teeth at the same landmarks using electronic digital caliper (Guanglu Co., Ltd., Guilin, China; resolution: 0.01 mm) and designated as the reference value. The linear deviation was defined as the difference of tooth length between 3D reconstruction model and the physical measurement. All the measurements were made in duplicate by the two examiners. The mean and standard deviations (SDs) were calculated. Pearson correlation coefficients were used to determine the reliability between the first and second measurements of two observers. An intraclass correlation coefficient (ICC) was calculated on the measurements to determine the level of interobserver reliability.[21] Moreover, paired Student's t-test was used to assess the linear deviation.
Volumetric deviation
The volume of each 3D reconstruction model was calculated by Geomagic Qualify 2012 automatically. The volume of the corresponding extracted teeth was measured by water displacement technique using a high precise Mettler-Toledo XPE205 Analytical Balances (Mettler-Toledo LLC, Switzerland; resolution: 0.01 mg). The physical volume of the teeth was calculated as shown in Equation 1 and designated as the reference value. Accuracy of CBCT volume measurements was assessed by comparing the volume of 3D reconstruction model with the physical volume. The volume deviation was defined by Equation 2. Paired Student's t-test was used to assess the volumetric deviation. Equation 1: Physical volume = (Weightin air− Weightin water)/Water density (room temperature). Equation 2: Volume deviation = (Volume3D surface model− Volumephysical)/Volumephysical× 100%.
Geometric deviation and visualization
The extracted teeth were scanned by 3Shape R700 optical scanner (3Shape A/S, Denmark; accuracy: 15 µm) to gain the optical model and designated as the reference models. The 3D reconstruction model (test) and the corresponding optical model (reference) were imported in Geomagic Qualify 2012 and brought into alignment automatically using the Iterated Closest Points algorithm.[22] These algorithms bring the two models into alignment by minimizing the distance between the two surfaces by calibrating six degrees transformation parameters (three rotation and three translation) [Figure 2a–2c].[23] The distribution of the distance was graphically visualized with a color map, starting with blue (minimum distances) and passing through yellow and then ending with red (maximum distances) [Figure 2d]. For each superimposed model, root mean square (RMS) was calculated and tested by one-sample t-test for each group to assess the geometric deviations (test value was 0).
Figure 2.
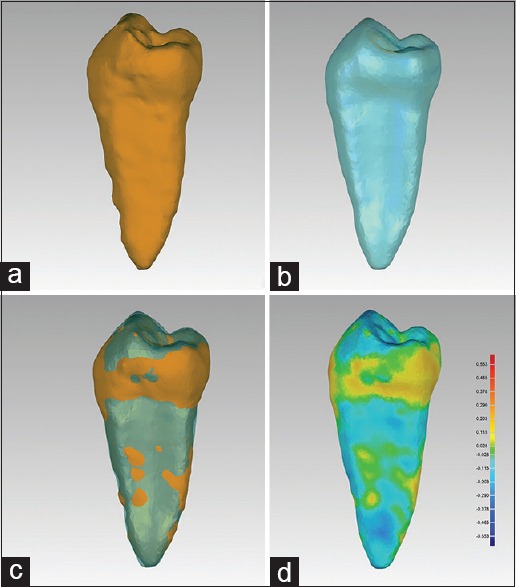
Align the 3D reconstruction model to optical model and 3D color map. (a) The 3D reconstruction model from CBCT. (b) Optical model of the corresponding extracted teeth. (c) The imposed 3D reconstruction model and optical models. (d) 3D color map of the geometric deviation. CBCT: Cone-beam computed tomography; 3D: Three-dimensional.
Influence of voxel size and cone-beam computed tomography system
To assess the influence of voxel size and CBCT system on the linear, volumetric, and geometric measurements, all fifty teeth were designed into three groups according to the CBCT system and voxel size [Table 1]: NewTom VG 0.15 mm group, NewTom VG 0.30 mm group, and VATECH DCTPRO 0.30 mm group. Linear, volumetric, and geometric deviations between each group were tested by one-way analysis of variance (ANOVA).
Statistical analysis
All statistical analyses were performed with a standard statistical software package (version 22.0, SPSS Inc., Chicago, IL, USA). Paired Student's t-test was used to assess the linear deviation, volumetric deviation for each group. One-sample t-test was used to assess the geometric deviations and the test value was 0. ANOVA was used to assess the influence of voxel size and CBCT system. The level of significance was set at 5% (α = 0.05).
RESULTS
Reproducibility of segmentation and measurement
To test the reproducibility of tooth segmentation, 15 teeth were randomly chosen to be segmented by the two examiners. The interexaminer reproducibility of 15 volume data was very high, with a Pearson correlation coefficient of 0.963 between the two examiners.
For linear measurement, Pearson correlation coefficients were 0.999 and 0.998 for the two observers, and ICC was 0.998 and 0.999 for model measurement and physical measurement to show a high level of intra- and inter-observer reliability, respectively.
Linear deviation
Lengths of 3D reconstruction teeth from CBCT in NewTom VG 0.15 mm group, NewTom VG 0.30 mm group, VATECH DCTPRO 0.30 mm group were 20.41 ± 1.74 mm, 20.11 ± 1.43 mm, and 19.28 ± 1.27 mm and tooth lengths on extracted teeth measured by electronic digital caliper (reference values) were 20.41 ± 1.80 mm, 20.14 ± 1.56 mm, and 20.21 ± 1.25 mm, respectively. Strong correlation coefficient of the tooth length between 3D reconstruction models and extracted teeth was found for each group (NewTom VG 0.15 mm group: r2 = 0.951; NewTom VG 0.30 mm group: r2 = 0.974; and VATECH DCTPRO 0.30 mm group: r2 = 0.949). Linear deviation values between the CBCT model and extracted teeth in each group were −0.03 ± 0.48 mm (NewTom VG 0.15 mm group: t = −0.263, P = 0.796), –0.45 ± 0.42 mm (NewTom VG 0.30 mm group: t = −4.313, P = 0.001), and −0.93 ± 0.40 mm (VATECH DCTPRO 0.30 mm group: t = −9.585, P < 0.001), respectively [Table 2]. Significant difference was found between NewTom VG 0.15 mm group and NewTom VG 0.30 mm group (P = 0.021) and between VATECH DCTPRO 0.30 mm group and NewTom VG 0.30 mm group(P = 0.008) [Figure 3a].
Table 2.
The linear, volumetric, and geometric comparison between 3D reconstructions of teeth from cone-beam computed tomography and the physical measurements of the extracted teeth (mean ± SD)
| Groups | Linear measurement (mm) | t | P | Volumetric measurement (mm3) | t | P | Geometric measurement (mm) | t | P | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 3D reconstruction | Extracted tooth | 3D reconstruction | Extracted tooth | ||||||||
| A (n = 17) | 20.41 ± 1.74 | 20.41 ± 1.80 | −0.263 | 0.796 | 499.302 ± 79.018 | 523.704 ± 85.437 | −8.079 | 0.000 | 0.117 ± 0.018 | 25.834 | 0.000 |
| B (n = 16) | 20.11 ± 1.43 | 20.14 ± 1.56 | −4.313 | 0.001 | 450.524 ± 78.628 | 475.691 ± 77.320 | −5.131 | 0.000 | 0.116 ± 0.014 | 34.071 | 0.000 |
| C (n = 17) | 19.28 ± 1.27 | 20.21 ± 1.25 | −9.585 | 0.000 | 455.037 ± 91.713 | 481.809 ± 105.003 | −3.922 | 0.001 | 0.194 ± 0.117 | 6.823 | 0.000 |
Paired Student’s t-test was used to assess the linear and volumetric deviation between 3D reconstructions of teeth from cone-beam computed tomography and the physical measurements of the extracted teeth. One-sample t-test was used to assess the geometric deviations and the test value was 0 (α = 0.05). A: NewTom VG 0.15 mm group; B: NewTom VG 0.30 mm group; C: VATECH DCTPRO 0.30 mm group. SD: standard deviation; 3D: Three-dimensional.
Figure 3.

The linear, volumetric and geometric deviation between 3D reconstructions of teeth from CBCT the physical measurements of the extracted teeth for the three groups. (a) Linear deviation. (b) Volumetric deviation. (c) Geometric deviation. A: NewTom VG 0.15 mm group (n = 17); B: NewTom VG 0.30 mm group (n = 16); C: VATECH DCTPRO 0.30 mm group (n = 17). *P < 0.01; †P> 0.05. CBCT: Cone-beam computed tomography; 3D: Three-dimensional.
Volumetric deviation
Volumes of 3D reconstruction teeth from CBCT in NewTom VG 0.15 mm group, NewTom VG 0.30 mm group, and VATECH DCTPRO 0.30 mm group were 499.302 ± 79.018 mm3, 450.524 ± 78.628 mm3, and 455.037 ± 91.713 mm3, and the physical measured volumes of extracted teeth (reference values) were 523.704 ± 85.437 mm3, 475.691 ± 77.320 mm3, and 481.809 ± 105.003 mm3, respectively. Strong correlation coefficients were found between the volumes of the 3D reconstruction models and physical measured volumes of extracted teeth (NewTom VG 0.15 mm group: r2 = 0.985; NewTom VG 0.30 mm group: r2 = 0.987; and VATECH DCTPRO 0.30 mm group: r2 = 0.985). Volumetric deviation values between the CBCT model and extracted teeth in each group were −5.4 ± 2.8% (NewTom VG 0.15 mm group: t = −8.079, P < 0.001), −4.5 ± 3.4% (NewTom VG 0.30 mm group: t = −5.131, P < 0.001), and −4.8 ± 5.1% (VATECH DCTPRO 0.30 mm group: t = −3.922, P = 0.001), respectively [Table 2]. However, there was no statistically significant difference (P > 0.05) between groups [Figure 3b].
Geometric deviation and visualization
Geometric deviation values in the three groups were 0.117 ± 0.018 mm (NewTom VG 0.15 mm group, t = 25.834, P < 0.001), 0.116 ± 0.014 mm (NewTom VG 0.30 mm group, t = 34.071, P < 0.001), and 0.194 ± 0.117 mm (VATECH DCTPRO 0.30 mm group, t = 6.823, P < 0.001), respectively [Table 2]. No statistically significant difference was observed between NewTom VG 0.15 mm and NewTom VG 0.30 mm groups (P = 0.999), but statistically significant difference was found between VATECH DCTPRO 0.30 mm and NewTom VG 0.30 mm groups (P = 0.006) [Figure 3c]. The distance between the imposed models was shown with a 3D color map. In general, the maximum deviation of segmentation region was mostly distributed at apex of the root or cusp and groove on occlusal surfaces [Figure 2d].
DISCUSSION
In this study, we used computer-assisted methods to determine if CBCT can be used to accurately reconstruct 3D tooth model. CBCT data and extracted teeth from patients for orthodontic purpose were used to make the study more relevant to clinical practice.
Accuracy of linear, volumetric, and geometric deviation on three-dimensional construction model from cone-beam computed tomography data
The first aim of this study was to assess the accuracy of the linear, volumetric, and geometric measurement of the 3D reconstruction models from CBCT data. In our study, Pearson correlation coefficients between the 3D reconstruction model and extracted teeth were high on linear and volumetric measurements, which confirmed the reliability of 3D reconstruction from CBCT data.
The linear deviations in NewTom VG 0.15 mm group, NewTom VG 0.30 mm group, and VATECH DCTPRO 0.30 mm group were −0.03 ± 0.48 mm, −0.45 ± 0.42 mm, and −0.93 ± 0.40 mm and the volume deviations were −5.4 ± 2.8%, −4.5 ± 3.4%, and −4.8 ± 5.1%, respectively. There was a tendency to underestimate the reference values in consistent with previous studies.[17,18,19,20,21]
Liu et al.[21] found that the volumetric measurements of teeth derived from CBCT deviated slightly from the physical volumes within the range of −4–7% and smoothing operations reduced volume measurements by 3–12%. In our study, the volume deviation was lower than Liu et al.'s results. One possible reason was that more accurate volume measurement technique was used in our study. The smoothing operations in tooth segmentation might be another reason to explain the difference between our results and Liu's.
Maret et al.[16] compared 120 pairs of micro-computed tomography (CT) (41 µm) and CBCT (76 µm) surfaces (one pair representing a single tooth), and the RMS between micro-CT and CBCT surfaces ranged from 0.051 to 0.249 mm. In our study, optical scans of the extracted teeth were taken as reference because it was more accurate (<20 µm) and more available. Geometric deviation between the CBCT surface and optical scans in our study ranged from 0.075 to 0.142 mm (NewTom VG 0.15 mm), 0.094–0.148 mm (NewTom VG 0.30 mm), and 0.154–0.330 mm (VATECH DCTPRO 0.30 mm). The high accuracy in our study confirmed the reliability of accurately reconstruct 3D tooth model from CBCT data.
On the geometric color map, the maximum deviation usually existed on the apex or groove on the occlusal surface [Figure 2d]. Because of the low contrast to noise ratio in CBCT, it was hard to distinguish the apex with the alveolar bone [Figure 4c, 4j, and 4k] and grooves details were less visible in comparison with optical scans [Figure 4d, 4h, and 4l].
Figure 4.

The influence of voxel size and CBCT system on the CBCT image quality. (a-d) NewTom VG 0.15 mm group: a sharp border and high signal-to-noise ratio. (e-h) NewTom VG 0.30 mm group, relative clear tooth border. (i-l) VATECH DCTPRO 0.30 mm group: ambiguous tooth border especially on apex, and higher beam hardening artifacts. CBCT: Cone-beam computed tomography.
Influence of voxel size and cone-beam computed tomography system on the accuracy of tooth segmentation
Many factors possibly influence the accuracy of the 3D reconstruction, including scanning system, FOV, examined object, exposure time, tube voltage and amperage, and also spatial resolution defined by the voxel size.[15] In clinical practice, most scanning and reconstruction parameters are preestablished and cannot be adjusted and limited parameters, such as voxel size, scanner system, FOV, can be chosen by dentist for specific diagnostic tasks and the study on these factors might be more usually to clinical practice.
Therefore, the second aim of the study was to investigate the influence of voxel size and CBCT system on the accuracy of 3D reconstruction. Medium FOV, mostly used in clinical practice, was chosen in our study. Two popular CBCT systems (NewTom VG CBCT scanner and VATECH DCTPRO CBCT scanner) and two commonly used voxel size of 0.15 mm and 0.30 mm were chosen in our study. However, 0.15 mm voxel size was unavailable in VATECH DCTPRO CBCT scanner system (the minimum voxel size was 0.20 mm). Hence, there were only three groups (NewTom VG 0.15 mm, NewTom VG 0.30 mm, and VATECH DCTPRO 0.30 mm) and no VATECH DCTPRO 0.15 mm group. No significant difference was found on volumetric and geometric measurement between the different voxel size groups in the same CBCT system (NewTom VG) in our study. The increased voxel resolution did not cause a significant difference on accuracy of the reconstruction models.
The diagnostic ability of CBCT images appears to be influenced by voxel size. Reducing the voxel resolution can result in a lower-quality image, more noise and artifacts, and less detailed anatomic information. Greater voxel size results in generally “sharper” images by increasing the signal-to-noise ratio [Figure 4a–4h]. However, greater voxel resolution is accomplished with an increased scanning time, exposing the patient to a higher radiation dosage also an increased risk of patient movement. Moreover, the patient movement will decrease the image quality and increase the difficulty of tooth segmentation [Figure 4].[24]
Liedke et al.[25] investigated simulated external root resorption of tooth roots imaged with voxel sizes of 0.40, 0.30, and 0.20 mm. They concluded that the results from the different voxel sizes were the same even if diagnosis was easier at a smaller voxel size of 0.30 or 0.20 mm. In our study, no significant difference was found between the NewTom VG 0.15 mm and NewTom VG 0.30 mm groups and it indicated that the benefits of a shorter scanning time (i.e., lower radiation exposure and less patient movement) might outweigh the poorer resolution. In addition, the lower voxel size scans needed a lower storage space in computer and were easier to transport on local area network. It implied in clinical practice, 0.30 mm would be suitable for accurate tooth segmentation. However, care must be taken when it came to a different CBCT system.
In our study, the geometric accuracy of the NewTom VG system was higher than the VATECH DCTPRO system even if using the same voxel size. Image quality was variant between different CBCT systems because of differences in detector type, scanning, and reconstruction parameters can cause different artifact levels. CBCT suffers from beam hardening artifacts because enamel is the hardest tissue in the human body, and the X-ray beam cannot be kept completely uniform.[26,27] However, the influence of beam hardening artifacts is much lower when a higher kVp (110 kVp in NewTom VG system, 90 kVp in VATECH DPRO system) leading a higher beam throughput and more uniform filtration and with more acquisitions available [Figure 4e–4l]. Besides, compared with VATECH DPRO system, NewTom VG equips with lower scan time to decrease movement artifact and better detector to get more volume information for reconstruction available.
In conclusion, CBCT can be used to accurately reconstruct 3D tooth model for linear, volumetric, and geometric measurements. Increasing the voxel resolution from 0.30 to 0.15 mm to construct a 3D model does not result in increased accuracy. However, different CBCT systems can have different measurement results even with the same voxel size.
Financial support and sponsorship
The work was supported by the grant from the Beijing Municipal Natural Science Foundation (No. Z151100003715007).
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to thank Dr. Dian-Yun Zhang, Dr. Jian-Min Han of the Dental Materials Laboratory for the help on the volume measurements of extracted teeth.
Footnotes
Edited by: Ning-Ning Wang
REFERENCES
- 1.Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone-beam computed tomography in dental practice. J Can Dent Assoc. 2006;72:75–80. [PubMed] [Google Scholar]
- 2.Dawood A, Patel S, Brown J. Cone beam CT in dental practice. Br Dent J. 2009;207:23–8. doi: 10.1038/sj.bdj.2009.560. doi: 10.1038/sj.bdj.2009.560. [DOI] [PubMed] [Google Scholar]
- 3.Watanabe H, Honda E, Tetsumura A, Kurabayashi T. A comparative study for spatial resolution and subjective image characteristics of a multi-slice CT and a cone-beam CT for dental use. Eur J Radiol. 2009;77:397–402. doi: 10.1016/j.ejrad.2009.09.023. doi: 10.1016/j.ejrad.2009.09.023. [DOI] [PubMed] [Google Scholar]
- 4.Bartling SH, Majdani O, Gupta R, Rodt T, Dullin C, Fitzgerald PF, et al. Large scan field, high spatial resolution flat-panel detector based volumetric CT of the whole human skull base and for maxillofacial imaging. Dentomaxillofac Radiol. 2007;36:317–27. doi: 10.1259/dmfr/19164138. doi: 10.1259/dmfr/19164138. [DOI] [PubMed] [Google Scholar]
- 5.Scarfe WC, Farman AG, Levin MD, Gane D. Essentials of maxillofacial cone beam computed tomography. Alpha Omegan. 2010;103:62–7. doi: 10.1016/j.aodf.2010.04.001. doi: 10.1016/j.aodf.2010.04.001. [DOI] [PubMed] [Google Scholar]
- 6.Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am. 2008;52:707–30. doi: 10.1016/j.cden.2008.05.005. doi: 10.1016/j.cden.2008.05.005. [DOI] [PubMed] [Google Scholar]
- 7.Li W, Chen F, Zhang F, Ding W, Ye Q, Shi J, et al. Volumetric measurement of root resorption following molar mini-screw implant intrusion using cone beam computed tomography. PLoS One. 2013;8:e60962. doi: 10.1371/journal.pone.0060962. doi: 10.1371/journal.pone.0060962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lee RJ, Weissheimer A, Pham J, Go L, de Menezes LM, Redmond WR, et al. Three-dimensional monitoring of root movement during orthodontic treatment. Am J Orthod Dentofacial Orthop. 2015;147:132–42. doi: 10.1016/j.ajodo.2014.10.010. doi: 10.1016/j.ajodo.2014.10.010. [DOI] [PubMed] [Google Scholar]
- 9.Kobayashi K, Shimoda S, Nakagawa Y, Yamamoto A. Accuracy in measurements of distance using limited cone-beam computerized tomography. Int J Oral Maxillofac Implants. 2004;19:228–30. [PubMed] [Google Scholar]
- 10.Han G, Huang S, Von den Hoff JW, Zeng X, Kuijpers-Jagtman AM. Root resorption after orthodontic intrusion and extrusion: An intraindividual study. Angle Orthod. 2005;75:912–8. doi: 10.1043/0003-3219(2005)75[912:RRAOIA]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Baysal A, Karadede I, Hekimoglu S, Ucar F, Ozer T, Veli I, et al. Evaluation of root resorption following rapid maxillary expansion using cone-beam computed tomography. Angle Orthod. 2012;82:488–94. doi: 10.2319/060411-367.1. doi: 10.2319/060411-367.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mangano FG, Cirotti B, Sammons RL, Mangano C. Custom-made, root-analogue direct laser metal forming implant: A case report. Lasers Med Sci. 2012;27:1241–5. doi: 10.1007/s10103-012-1134-z. doi: 10.1007/s10103-012-1134-z. [DOI] [PubMed] [Google Scholar]
- 13.Shen P, Zhao J, Fan L, Qiu H, Xu W, Wang Y, et al. Accuracy evaluation of computer-designed surgical guide template in oral implantology. J Craniomaxillofac Surg. 2015;43:2189–94. doi: 10.1016/j.jcms.2015.10.022. doi: 10.1016/j.jcms.2015.10.022. [DOI] [PubMed] [Google Scholar]
- 14.Eggers G, Mühling J, Hofele C. Clinical use of navigation based on cone-beam computer tomography in maxillofacial surgery. Br J Oral Maxillofac Surg. 2009;47:450–4. doi: 10.1016/j.bjoms.2009.04.034. doi: 10.1016/j.bjoms.2009.04.034. [DOI] [PubMed] [Google Scholar]
- 15.Kamburoglu K, Murat S, Kolsuz E, Kurt H, Yüksel S, Paksoy C. Comparative assessment of subjective image quality of cross-sectional cone-beam computed tomography scans. J Oral Sci. 2011;53:501–8. doi: 10.2334/josnusd.53.501. doi: 10.2334/josnusd.53.501. [DOI] [PubMed] [Google Scholar]
- 16.Maret D, Molinier F, Braga J, Peters OA, Telmon N, Treil J, et al. Accuracy of 3D reconstructions based on cone beam computed tomography. J Dent Res. 2010;89:1465–9. doi: 10.1177/0022034510378011. doi: 10.1177/0022034510378011. [DOI] [PubMed] [Google Scholar]
- 17.Brown AA, Scarfe WC, Scheetz JP, Silveira AM, Farman AG. Linear accuracy of cone beam CT derived 3D images. Angle Orthod. 2009;79:150–7. doi: 10.2319/122407-599.1. doi: 10.2319/122407-599.1. [DOI] [PubMed] [Google Scholar]
- 18.Mischkowski RA, Pulsfort R, Ritter L, Neugebauer J, Brochhagen HG, Keeve E, et al. Geometric accuracy of a newly developed cone-beam device for maxillofacial imaging. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:551–9. doi: 10.1016/j.tripleo.2007.02.021. doi: 10.1016/j.tripleo.2007.02.021. [DOI] [PubMed] [Google Scholar]
- 19.Lagravère MO, Carey J, Toogood RW, Major PW. Three-dimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop. 2008;134:112–6. doi: 10.1016/j.ajodo.2006.08.024. doi: 10.1016/j.ajodo.2006.08.024. [DOI] [PubMed] [Google Scholar]
- 20.Stratemann SA, Huang JC, Maki K, Miller AJ, Hatcher DC. Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac Radiol. 2008;37:80–93. doi: 10.1259/dmfr/31349994. doi: 10.1259/dmfr/31349994. [DOI] [PubMed] [Google Scholar]
- 21.Liu Y, Olszewski R, Alexandroni ES, Enciso R, Xu T, Mah JK. The validity of in vivo tooth volume determinations from cone-beam computed tomography. Angle Orthod. 2010;80:160–6. doi: 10.2319/121608-639.1. doi: 10.2319/121608-639.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Besl PJ, McKay ND. A method for registration of 3-D shapes. IEEE Trans Pattern Anal Mach Intell. 1992;14:239–56. doi: 10.1109/34.121791. [Google Scholar]
- 23.Zhang Z. Iterative point matching for registration of free-form curves and surfaces. Int J Comput Vis. 1994;13:119–52. doi: 10.1007/BF01427149. [Google Scholar]
- 24.Damstra J, Fourie Z, Huddleston Slater JJ, Ren Y. Accuracy of linear measurements from cone-beam computed tomography-derived surface models of different voxel sizes. Am J Orthod Dentofacial Orthop. 2010;137:16, e1–6. doi: 10.1016/j.ajodo.2009.06.016. doi: 10.1016/j.ajodo.2009.06.016. [DOI] [PubMed] [Google Scholar]
- 25.Liedke GS, da Silveira HE, da Silveira HL, Dutra V, de Figueiredo JA. Influence of voxel size in the diagnostic ability of cone beam tomography to evaluate simulated external root resorption. J Endod. 2009;35:233–5. doi: 10.1016/j.joen.2008.11.005. doi: 10.1016/j.joen.2008.11.005. [DOI] [PubMed] [Google Scholar]
- 26.Herkströter FM, Ten Bosch JJ. Wavelength-independent microradiography: A method for non-destructive quantification of enamel and dentin mineral concentrations using polychromatic x-rays. J Dent Res. 1990;69:1522–6. doi: 10.1177/00220345900690081501. doi: 10.1177/00220345900690081501. [DOI] [PubMed] [Google Scholar]
- 27.Al-Rawi B, Hassan B, Vandenberge B, Jacobs R. Accuracy assessment of three-dimensional surface reconstructions of teeth from cone beam computed tomography scans. J Oral Rehabil. 2010;37:352–8. doi: 10.1111/j.1365-2842.2010.02065.x. doi: 10.1111/j.1365-2842.2010.02065.x. [DOI] [PubMed] [Google Scholar]