

Introduction
Health surveillance is the ongoing, systematic use of routinely collected health data to guide public health action in a timely fashion.1
This paper describes the creation and growth of national surveillance systems in Canada and their impact on chronic disease and injury prevention.
In 2008, the authors started a review process to retrace the history of the early development of national chronic disease surveillance in Canada from 1960 to 2000. A 1967 publication describes the history of the development of the Laboratory of Hygiene from 1921 to 1967.2 This review is a sequel to that paper and describes the history of the development of national chronic disease surveillance in Canada before and after the formation of the Laboratory Centre for Disease Control (LCDC).
A brief history of the structure of federal departments and agencies responsible for chronic disease surveillance in Canada
The 1867 British North America Act3 specified that the census and statistics are the responsibility of the federal government (Table 1). The first national census under the auspices of this act was conducted in 1871.
TABLE 1. History timeline in national chronic disease surveillance in Canada, 1867–2004.
| Year | Event |
|---|---|
| 1867 | British North America Act3 specified that the census and statistics are the responsibility of the federal government. |
| 1871 | The first national census was conducted in Canada under the auspices of the British North America Act. |
| 1918 | The Statistics Act4 created the Dominion Bureau of Statistics (DBS) (1918–1971) with a mandate to collect and publish statistical information relative to the social, economic and general activities and conditions of the population. |
| 1919 | Department of Health Act created the Department of Health (1919–1928).5 |
| 1921 | Division of Laboratories and Medical Research (DLMR) (1921-1925) was created in the Department of Health as a national laboratory for public health and research.2 |
| 1925 | DLMR was renamed Laboratory of Hygiene (1925–1971).2 |
| 1928 | The Department of Health was renamed Department of Pensions and National Health (DPNH) (1928–1944). |
| 1937 | Epidemiology Division was formed but was dissolved during World War II. |
| 1944 | Department of National Health and Welfare (DNHW) was created (1944–1993).53 DNHW was also referred to as Health and Welfare Canada (HWC) (1980–1993). |
| 1945 | The Rockefeller Foundation was commissioned to assess the need for epidemiology services in Canada. |
| 1947–1971 | The Epidemiology Division was re-established (1937–1939, 1947–1971) with a focus on infectious diseases. |
| 1954–1961 | Large cohort study of Canadian veterans and smoking.54,55 |
| 1959 | Publication of an article by Newcombe et al.38 described automatic linkage of vital records and stated that computers could be used to follow up individuals and families using files of routine vital statistics and health records. This included the British Columbia registry of handicapping conditions dating back to 1952, a surveillance scheme for congenital anomalies in British Columbia, and the later Registry of Handicapped Children and Adults, which removed the age limit of 21 following the thalidomide disaster in 1961. |
| 1961 | Thalidomide was marketed in Canada to treat nausea in early pregnancy. It was the cause of 115 known cases of severe birth defects. |
| 1961 | Royal Commission on Health Services (the Hall Commission) recommended that the Dominion Bureau of Statistics (DBS) collect and publish national morbidity statistics. To produce comparable statistics at a national level, DBS created the Hospital Morbidity program. |
| 1965 | DNHW established the Voluntary Drug Adverse Reaction Reporting Program (VDARRP). |
| 1966 | Maternal Child Health Program initiated a pilot birth-defect surveillance system in 4 provinces. |
| 1970 | Congenital Anomalies Surveillance System (CASS) was created, based on the success of a birth-defect surveillance pilot project. |
| 1971 | Dominion Bureau of Statistics was renamed Statistics Canada (1971–). |
| 1971 | Laboratory of Hygiene was renamed Canadian Communicable Disease Centre (CCDC) (1971). |
| 1972 | Epidemiology Division was renamed Bureau of Epidemiology (1972–1986) and merged with CCDC to become the Laboratory Centre for Disease Control (LCDC) (1972–2000). |
| 1972 | Health Protection Branch (HPB) (1972–2000) was created with 6 organizational units: LCDC, Foods Directorate, Drugs Directorate, Environmental Health Directorate, Field Operations Directorate and Administration Services. |
| 1972 | LCDC and Statistics Canada started to develop data infrastructure to monitor national chronic disease incidence and mortality. Examples include the Canadian Mortality Data Base (CMDB) (data from 1950 onward), a national cancer registry and a generalized record linkage system. |
| 1972 | National Cancer Incidence Reporting System (NCIRS), which includes the Canadian Cancer Data Base (CCDB; data from 1969 onward), was established. |
| 1972–1973 | LCDC initiated surveillance of cancer and cardiovascular disease. |
| 1973 | CASS was transferred from Environmental Health Directorate to LCDC. |
| 1976 | Royal Commission on the Health and Safety of Workers and Mines (the Ham Commission) published its report in response to a wildcat strike by mine workers in Elliott Lake over health and safety concerns. |
| 1978–1979 | Statistics Canada conducted Canada Health Survey (CHS). |
| 1979 | First record linkage workshop held at Statistics Canada devoted almost exclusively to applications in cancer epidemiology. |
| 1980 | LCDC initiated a journal, Chronic Diseases in Canada (CDIC) (1980–2011). The journal was renamed Chronic Diseases and Injuries in Canada (CDIC) in 2011 and Health Promotion and Chronic Disease Prevention in Canada: Research, Policy and Practice (HPCDP) in 2015. |
| 1981 | Howe and Lindsay40 describe the Generalized Iterative Record Linkage System (GIRLS), a Canadian invention that is now used worldwide. |
| 1981–1986 | Statistics Canada operated the Canadian Renal Failure Registry with joint funding through Health and Welfare Canada (HWC), Statistics Canada and the Kidney Foundation of Canada. |
| 1984 | Canada Health Act56 was adopted. The Act specifies the conditions and criteria with which the provincial and territorial health insurance programs must conform to receive federal health transfer payments. These criteria require universal coverage (for all “insured persons”) for all “medically necessary” hospital and physician services, without co-payments. |
| 1984 | Recommendations of a Health Protection Branch (HPB) science panel on epidemiology included: (a) surveillance of human health risks related to products regulated by HPB, (b) new data sources, (c) communication and (d) collaboration between personnel and coordination of activities in HPB and in other agencies. |
| 1984 | The Bureau of Epidemiology initiated plans for Nova Scotia–Saskatchewan Cardiovascular Disease Mortality Study (NSSCDMS), including validation of hospitalization data on myocardial infarctions. |
| 1985 | National diabetes task force meeting in Montebello, Quebec, recommended developing and implementing a national program to combat diabetes. |
| 1985–1988 | LCDC led the Community Risk Factor Survey to assess risk factor prevalence at the local level. |
| 1985–1989 | LCDC conducted the LCDC/National Health Research and Development Program (NHRDP) Epidemiology Graduate Student Training Program. |
| 1986 | Bureau of Epidemiology was split into the Bureau of Communicable Disease Epidemiology and the Bureau of Non-communicable Disease Epidemiology (BNDE) (1986). |
| 1986 | The first provincial heart health survey, under the Canadian Heart Health Initiative (CHHI) of the Health Promotion Directorate, was conducted in Nova Scotia. Eventually all 10 provinces undertook heart health surveys between 1986 and 1995. |
| 1987 | BNDE was renamed the Bureau of Chronic Disease Epidemiology (BCDE) (1987–1995). |
| 1987 | BCDE initiated surveillance of asthma morbidity and mortality using Statistics Canada national databases. This report17 led to a national workshop on asthma that recommended carrying out descriptive, case-control and cohort studies. Subsequently, several studies were conducted.57-59 |
| 1987 | Canadian Renal Failure Registry was incorporated into the Canadian Organ Replacement Registry and run by Hospital Medical Records Institute (HMRI). It was funded as a partnership of the federal and provincial governments. |
| 1987 | BCDE organized a national workshop on Alzheimer disease that strongly recommended a national multi-centre research study. |
| 1989 | Statistics Canada initiates its journal Health Reports (HR) (1989–). |
| 1989 | Statistics Canada initiates development of the Canadian Cancer Registry (CCR) (1992–). |
| 1989 | BCDE collaborated with the Canadian Pediatrics Society to initiate the Children's Hospitals Injury Research and Prevention Program (CHIRPP) (1989–, renamed Canadian Hospitals Injury Reporting and Prevention Program in 1991) for the surveillance of childhood injuries. |
| 1989 | The first Canadian Epidemiology Research Conference and record linkage workshop were held. Follow-up from these meetings led to the establishment of the Canadian Society for Epidemiology and Biostatistics (CSEB) in 1990. |
| 1989 | BCDE collaborated with the University of Ottawa to initiate the Canadian Study of Health and Aging (CSHA), which had 3 study phases of data collection (1991–1992, 1996–1997, 2001–2002). |
| 1990 | BCDE initiated active surveillance of childhood cancers, asthma, diabetes, child maltreatment and perinatal health. |
| 1990 | Mortality study of Canadian male farm operators60 was the first cohort study of cancer risks in relation to pesticide use among farmers and also the first epidemiologic study based on linkage of general population and agricultural census records. |
| 1991 | Health Canada published first report on Economic Burden of Illness in Canada (EBIC) with 1986 data.31 These analyses of direct and indirect costs of illness in Canada included estimates for major disease categories and injuries. |
| 1992 | Canadian Cancer Registry (CCR) was established (1992–). |
| 1992 | Proposal to develop a childhood cancer control program was submitted and accepted under the federal Brighter Futures initiative. Funds started in 1994, as did registration in the national database of the Canadian Childhood Cancer Control Program (CCCCP).13 |
| 1992–1994 | The Cancer Bureau contracted University of Toronto and the Ontario Cancer Treatment and Research Foundation (OCTRF) to conduct the Great Lakes Basin Cancer Risk Assessment Study (GLBCRAS).14,15 |
| 1993 | DNHW was restructured, and the health component was renamed Health Canada (1993–). |
| 1993 | Development of the Canadian Birth Data Base (CBDB) and Canadian Stillbirth Data Base (CSDB) (data from 1985) was initiated to study reproductive outcomes using record linkages. |
| 1993 | An asthma program was established in BCDE as a separate division because of observed increases of hospitalization and mortality rates due to asthma among young Canadians. |
| 1993 | Canadian Breast Cancer Screening Data Base (CBCSD) was established by BCDE to monitor and evaluate organized breast cancer screening programs. |
| 1994 | The Canadian Institute for Health Information (CIHI) (1994–) was established to provide essential information on Canada's health system and the health of Canadians. Responsibility for hospital separation data was transferred from Statistics Canada to CIHI. |
| 1994 | Statistics Canada started the National Population Health Survey (NPHS) (1994–). |
| 1994–1995 | LCDC identified perinatal health as a priority health surveillance gap. |
| 1994–1997 | National Enhanced Cancer Surveillance System (NECSS) was conducted through federal–provincial collaboration. Detailed risk factor questionnaire information was collected (beginning in 1994) from a Canada-wide sample of patients recently diagnosed with cancer and population control subjects. |
| 1995 | Creation of 3 chronic disease bureaus within LCDC: (1) Cancer Bureau (CB) (1995–2000), (2) Bureau of Reproductive and Child Health (BRCH) (1995–2000) and (3) Bureau of Cardio-Respiratory Diseases and Diabetes (BCRDD) (1995–2000).8 |
| 1995 | Canadian Perinatal Surveillance System (CPSS) (1995–) was initiated to collect and analyze data on all recognized pregnancies (regardless of their outcome) and on the health of the baby during the first year of life. |
| 1995–1996 | The Student Lung Health Survey (SLHS) was a school-based survey of children aged 5–19 years in 9 voluntary health units across Canada. |
| 1995–2000 | LCDC led the National Asthma Control Task Force (NACTF) and developed the National Asthma Prevention and Control Strategy. |
| 1996 | LCDC officially launched its website to provide public health information online. |
| 1996 | National Diabetes Surveillance System (NDSS) was initiated (1996–2009). NDSS expanded and became the Canadian Chronic Disease Surveillance System (CCDSS) in 2009. |
| 1996 | Development of a child maltreatment surveillance program began. Canadian Incidence Study of Reported Child Abuse and Neglect (CIS) started collecting data in 1998. |
| 1996–1997 | BCRDD conducted the Physician Asthma Management Survey (PAMS) to identify physicians' practices in Canada. |
| 1996–1998 | To address the key components of perinatal health, Canadian Perinatal Surveillance System (CPSS) created (1) the Fetal and Infant Health Study Group, (2) the Maternal Health Study Group and (3) the Maternal Experiences Study Group. |
| 1997 | Health Canada published second report on Economic Burden of Illness in Canada (EBIC) with 1993 data.32 |
| 1998 | LCDC participated in a steering committee on risk factor surveillance at the local level. In 1999, a pilot project was conducted to test the concept and a prototype of a rapid risk factor surveillance system at the local level.42 This subsequently led to the Rapid Risk Factor Surveillance System (RRFSS), which has been in operation in Ontario since then. |
| 2000 | LCDC was dissolved and reorganized as the Population and Public Health Branch (PPHB) (2000–2004) of Health Canada. The Centre for Chronic Disease Prevention and Control (CCDPC) (2000–2012, renamed Centre for Chronic Disease Prevention, CCDP, in 2012) was created to include the 3 chronic disease bureaus of the former LCDC. |
| 2000 | Statistics Canada started the Canadian Community Health Survey (CCHS) (2000–). |
| 2000 | First Canadian Perinatal Health Report was published. |
| 2002 | Health Canada published online the third report on Economic Burden of Illness in Canada (EBIC) with 1998 data.33 |
| 2004 | PPHB was reorganized and upgraded to a higher level, and the Public Health Agency of Canada (PHAC) (2004–) was established. The work of PHAC covers both chronic and infectious disease surveillance and emergency preparedness. A branch within PHAC, the Health Promotion and Chronic Disease Prevention Branch (HPCDPB) (2004–), was created to oversee chronic diseases, including surveillance. |
| 2004 | Chronic Disease Surveillance Division (CDSD) (2004–2010) within the Centre for Chronic Disease Prevention and Control (CCDPC) of the Health Promotion and Chronic Disease Prevention Branch (HPCDPB) specifically plans, co-ordinates and conducts national chronic disease surveillance. It was renamed as the Chronic Disease Surveillance and Monitoring Division (CDSM) in 2010 and the Surveillance and Epidemiology Division (SED) in 2014 (2014–). |
The 1918 federal Statistics Act4 created the Dominion Bureau of Statistics (DBS, called Statistics Canada as of 1971) with a mandate to collect and publish statistical information.
The 1919 Department of Health Act created the Department of Health.5 In 1937, the Epidemiology Division was formed in what was then the Department of Pensions and National Health, but was dissolved during World War II, and re-established in 1947 with a focus on infectious diseases. When the Health Protection Branch (HPB) was created within the Department of National Health and Welfare (DNHW) in 1972, the Epidemiology Division was renamed the Bureau of Epidemiology and merged with the much larger Canadian Communicable Disease Centre (formerly called the Division of Laboratories and Medical Research, established in 1921, and renamed the Laboratory of Hygiene in 1925)2 to form the new the Laboratory Centre for Disease Control (LCDC). In 1972–1973, LCDC's Bureau of Epidemiology initiated the surveillance of cancer and cardiovascular diseases. Surveillance activities for cancer used provincial cancer registry data, while those for cardiovascular disease relied on survey and mortality data.6,7 In 1995, three bureaus were created in LCDC—the Cancer Bureau, the Bureau of Reproductive and Child Health (BRCH) and the Bureau of Cardio-Respiratory Diseases and Diabetes (BCRDD).8
In 2000, Health Canada was reorganized, and LCDC was combined with the Health Promotion and Programs Branch (HPPB) to create a new branch, the Population and Public Health Branch (PPHB).9 In 2004, PPHB was reorganized and became part of the Public Health Agency of Canada (PHAC).
Figure 1 summarizes the organizational evolution of the federal health departments, branches and directorates that relate to the development of national chronic disease surveillance in Canada.
FIGURE 1. Organizational changes in the Canadian federal government departments and agencies that conducted national chronic disease surveillance, 1960–2010.
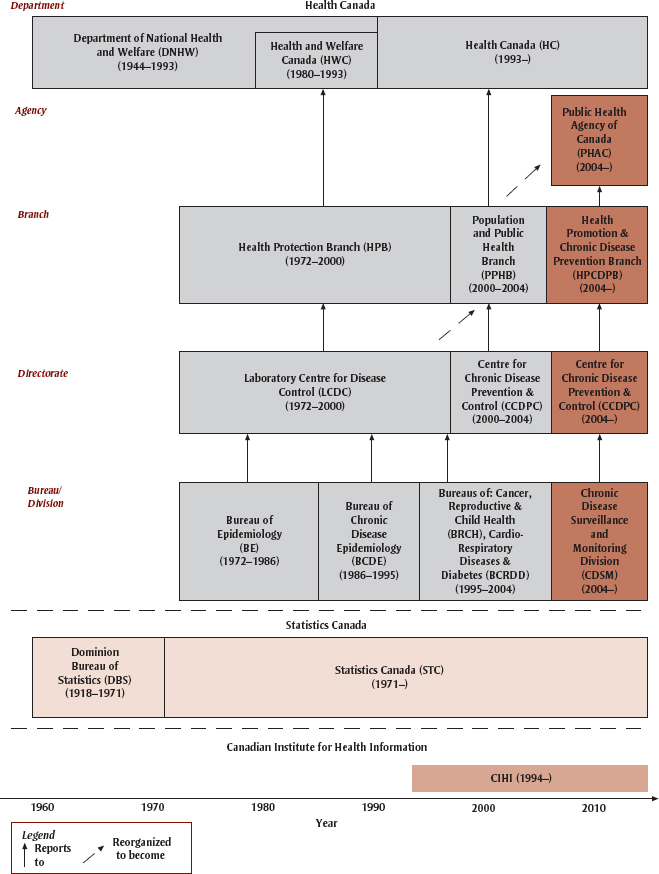
Besides Health Canada and PHAC, two other major organizations that contribute to national chronic disease surveillance are Statistics Canada and Canadian Institute for Health Information (CIHI).
A brief history of major initiatives for chronic disease surveillance in Canada
Cardiovascular disease
The Nova Scotia–Saskatchewan Cardiovascular Disease Mortality Study (NSSCDMS) was a collaborative surveillance project initiated in 1984 by the Bureau of Epidemiology. This study produced the first population-based estimates of acute myocardial infarction incidence, recurrence and survival in Canada.10 Existing administrative data sets were used for surveillance purposes through record linkage, linking hospital admission/separation records with mortality data, and thus creating person-oriented information for the first time.11
Important provincial partnerships with the Canadian Heart Health Initiative (CHHI) (1986–1995) of the Health Promotion Directorate supported standardized risk factor surveys in the provinces, including both behavioural and biological measures, and paved the way for the future work in Canada. In 1986, the first provincial heart health survey was conducted in Nova Scotia. Eventually, all 10 provinces undertook heart health surveys between 1986 and 1995. Through home interviews and clinic visits, the heart health surveys collected information and physical measures on cardiovascular risk factors as well as knowledge of the causes and consequences of cardiovascular disease.12
Cancer
The National Cancer Incidence Reporting System (NCIRS) was initiated in 1972 by Statistics Canada in collaboration with the National Cancer Institute of Canada and Health and Welfare Canada. Eventually, data were collected back to 1969 from all of the provincial and territorial cancer registries. In 1974, the Bureau of Epidemiology formed a section to accelerate analysis of national cancer incidence and mortality data. The Canadian Cancer Registry (CCR) was established in 1992. The person-oriented CCR was developed over 10 years from 1988 to 1998, and starting with data from 1992, featured internal record linkage to remove duplicates and death clearance to permit calculation of survival rates. As of 1987, Canadian Cancer Statistics provides annual ongoing national surveillance of trends as well as current year estimates of the cancer burden.
In 1992, the Bureau of Chronic Disease Epidemiology (BCDE) initiated the Canadian Childhood Cancer Control Program (CCCCP). BCDE worked with the 21 pediatric oncology centres in Canada to collect childhood cancer data with detailed patient information that allowed for enhanced surveillance and etiological research.13
In 1992–1994, the Cancer Bureau participated in the Great Lakes Basin Cancer Risk Assessment Study (GLBCRAS) in collaboration with the Environmental Health Directorate of the Health Protection Branch (HPB) and Environment Canada. The Division contracted the University of Toronto and the Ontario Cancer Treatment and Research Foundation (OCTRF) to study the effect of chlorinated drinking water on the development of bladder and colon cancers.14,15
In collaboration with the Health Programs and Services Branch of Health Canada, the BCDE established the Canadian Breast Cancer Screening Database (CBCSD) in 1993 to monitor and evaluate organized breast cancer screening programs.
Between 1994 and 1997, LCDC conducted the National Enhanced Cancer Surveillance System (NECSS) in collaboration with the provincial cancer registries, collecting detailed risk factor information by questionnaire from a Canada-wide sample of over 20 000 patients diagnosed with one of 19 types of cancer and over 5000 population-based control subjects.16 The Environmental Quality Data Base (EQDB) was developed in parallel to link with the subjects' residential histories and aid research on the relationships between cancer and measures of industrial activity, and air and drinking water quality.
Asthma
In 1987, the Bureau of Chronic Disease Epidemiology (BCDE) began the surveillance of asthma morbidity and mortality using Statistics Canada's national databases.17 After detecting an epidemic of asthma deaths among Canadians aged 15 to 34 years, BCDE convened a national workshop in 1987 that stimulated research on asthma and highlighted the need for improved asthma treatment. In 1993, an asthma program was established in BCDE.
In 1995, the BCRDD, in partnership with national medical and health professional associations, established the National Asthma Control Task Force (NACTF) to reduce asthma morbidity and mortality in Canada. Between 1995 and 2000 the NACTF developed the National Asthma Prevention and Control Strategy. To collect necessary data for formulation of effective asthma intervention strategies, an asthma supplement survey was incorporated into the National Population Health Survey (NPHS) in 1995.
The Student Lung Health Survey (SLHS; 1995–1996), a school-based survey of children aged 5 to 19 years in nine voluntary health units across Canada, was part of a Sentinel Health Unit Surveillance System.18 BCRDD conducted the Physician Asthma Management Survey (PAMS; 1996–1997) to identify physicians' practices in Canada.19,20
Diabetes
BCRDD initiated the National Diabetes Surveillance System (NDSS) in 1996. The NDSS was the first such system to use provincial data on physician encounters and hospitalizations to calculate disease prevalence. NDSS was a network of regionally distributed diabetes surveillance systems that compiled administrative health care data relating to diabetes and sent aggregate anonymous data to Health Canada for national analyses. In 2009, NDSS expanded into the Canadian Chronic Disease Surveillance System (CCDSS) with the addition of hypertension, asthma and other chronic disease surveillance.
Child and maternal health
The thalidomide disaster in 1961 caused 115 known cases of severe birth defects during 1961 and 1962.21 As a result, Department of National Health and Welfare (DNHW) established the Voluntary Drug Adverse Reaction Reporting Program (VDARRP) in 1965. In 1966, the Child and Maternal Health Division started a pilot system of birth-defects surveillance in 4 provinces (British Columbia, Alberta, Manitoba and New Brunswick),22 and in 1966, the Congenital Anomalies Surveillance System (CASS) was established. By 1989, the system included Alberta, Manitoba, Ontario, New Brunswick, Nova Scotia, Prince Edward Island and the Northwest Territories, while British Columbia had stopped submitting data.23 Newfoundland joined in 2004.24 This was the first national purpose-built surveillance system based on vital statistics data.
In 1989, the BCDE collaborated with the Canadian Pediatrics Society to initiate the Children's Hospitals Injury Research and Prevention Program (CHIRPP). CHIRPP became the Canadian Hospitals Injury Reporting and Prevention Program in 1991. In 1995, the Canadian Perinatal Surveillance System (CPSS) was initiated to collect and analyze data on all recognized pregnancies and on the health of the baby during the first year of life. This is an ongoing national surveillance program, now delivered through PHAC. In 1996, the Bureau of Reproductive and Child Health (BRCH) initiated a child maltreatment surveillance program, the Canadian Incidence Study of Reported Child Abuse and Neglect (CIS), which collects data from all Canadian jurisdictions.25
Starting in 1993, Statistics Canada provided the Canadian Birth Data Base (CBDB) and the Canadian Stillbirth Data Base (CSDB) with data from 1985 onward, in response to the ongoing need for the Canadian Perinatal Surveillance System and other uses.26,27
Aging-related diseases
In 1989, the BCDE collaborated with the University of Ottawa to initiate 3 phases of the Canadian Study of Health and Aging (CSHA), designed to measure the incidence and prevalence of Alzheimer's disease and other dementias and explore potential causal factors on a national scale.28 The CSHA operated in 18 centres across all provinces and, in 1991 to 1992, recruited over 10 000 seniors who participated in screening interviews, a risk factor questionnaire, a clinical examination and clinical tests.29,30
Cost of illness
The Economic Burden of Illness in Canada (EBIC) is an analysis of the direct and indirect costs of illness in Canada. LCDC published the first EBIC report with 1986 data in 1991,31 and again with 1993 data in 1997.32 The 1998 data were published online.33
The first EBIC report provides comprehensive and authoritative estimates of the cost of illness in Canada. These estimates are vital to setting priorities for allocating limited health resources. The second report improved significantly on the first, providing estimates of the direct and indirect costs of illness in Canada by age and sex. To research and write the third report, LCDC staff collaborated with their colleagues in Statistics Canada, CIHI and Health Canada to provide information by cost component (direct and indirect), diagnostic category, age, sex and province/territory.33 The project was moved from LCDC's Cancer Bureau to the Bureau of Policy and Planning, and is now managed by PHAC.
Surveys and administrative databases
National surveying of chronic diseases was in its infancy in Canada when the LCDC was formed in 1972. Early surveys included the Canadian Sickness Survey (1950–1951), the Survey of Smoking Habits (supplements to the Labour Force Survey) (1966–1975) and the Nutrition Canada Survey (1970–1972).34
In the 1970s, LCDC and Statistics Canada developed data infrastructure to monitor national chronic disease trends and to facilitate the conduct of major epidemiology (cohort) studies. The computerized Canadian Mortality Data Base (CMDB) was initiated to facilitate record linkage to national death records (from 1950 onwards) for a major cohort study35 after the National Cancer Institute of Canada provided a small subvention. The NCIRS (from 1969 onward) was used not only for surveillance but also to evaluate screening programs, to conduct cohort studies and, eventually, for survival analysis.36,37 With the process of record linkage pioneered by Newcombe,38,39 utilizing these databases was facilitated by the development of a Generalized Iterative Record Linkage System (GIRLS).40,41
Since the Canada Health Survey was conducted in 1978 to 1979, more surveys have become available. Examples include the General Social Surveys (1985–), the Health and Activity Limitations Survey (1983–), the Heart Health Surveys (1986–1995), the National Population Health Survey (1994–) and the National Longitudinal Survey of Children and Youth (1995–).34 The Canadian Community Health Survey (2000–) and the Canadian Health Measures Survey (2007–) are the most recent national health surveys relevant to chronic disease surveillance.
In 1998, LCDC collaborated with Cancer Care Ontario, Ontario Ministry of Health and Durham Regional Health Authority to set up a steering committee on risk factor surveillance at the local level. In 1999, a pilot project was conducted in the Durham health region to test the concept and a prototype of a rapid risk factor surveillance system at the local level. The pilot project, which proved to be a success,42 subsequently led to the Rapid Risk Factor Surveillance System (RRFSS) still in operation in Ontario today.
Record linkage
A significant achievement in science was the Canadian invention of the world's first protocol for computerized record linkage. Methodological research on computerized record linkages arose out of the necessity to link individuals' records from different databases. The LCDC conducted this research in collaboration with Statistics Canada and the National Cancer Institute of Canada (NCIC) Epidemiology Unit at the University of Toronto.26,38-40,43-46 In the mid-1970s, the GIRLS was developed to facilitate cohort studies.40,41 From 1978 to 2000, LCDC funded several occupational and environmental health research projects involving record linkage.27,47,48
Although record linkage was initially to assess risk, it has become a valuable tool for surveillance. The NDSS (1996–2009) and the subsequent CCDSS (2009–) rely heavily on record linkage. Computerized record linkage is now widely used across Canada and around the world.
Information dissemination
In 1980, LCDC started a journal, Chronic Diseases in Canada (CDIC) (1980–2011), which was renamed Chronic Diseases and Injuries in Canada (CDIC) in 2011 and Health Promotion and Chronic Disease Prevention in Canada: Research, Policy and Practice in 2015. In 1989, the Health Statistics Division of Statistics Canada initiated its new journal, Health Reports (HR) (1989–). Both journals publish peer-reviewed articles on chronic disease epidemiology, public health, biostatistics, behavioural sciences, health services and health economics. Many disease- and topic-specific publications have also been produced by the former LCDC, PHAC, Statistics Canada and CIHI.
In 1996, LCDC officially launched its website to provide public health information online. Moving into the electronic age, the general public has benefited greatly from online information products such as Disease Surveillance On-Line (http://www.phac-aspc.gc.ca/dsol-smed/) and Injury Surveillance On-Line (http://www.phac-aspc.gc.ca/surveillance-eng.php). Since 2000, Health Indicators has been produced jointly by Statistics Canada and CIHI (http://www.cihi.ca/cihiweb/dispPage.jsp?cw_page=indicators_e). An online publication, Health Indicators is a compilation of indicators measuring health status, non-medical determinants of health, health-system performance, and community and health-system characteristics.
Discussion
National chronic disease surveillance has a critical role in determining trends in chronic diseases. Surveillance enables governments and stakeholders to monitor the effects of public health interventions and project health resource requirements. The basic question is, what effect has surveillance information and activities had on improving the health of Canadians? Surveillance is only a means to an end. Surveillance is useful only if the results can be applied to reduce morbidity and suffering, save lives and improve the quality of life of the population.
The disease surveillance work in Canada has helped improve a number of health conditions. The decline in lung cancer cases was partly due to the surveillance and epidemiology work on tobacco use that provided the basis for a major push in the tobacco area. Some LCDC scientists were recognized as expert witnesses in court cases on tobacco. Cancer incidence and mortality data were used to prioritize and evaluate cancer control programs, such as screening for breast and colorectal cancer. The British Columbia Health Surveillance Registry was used early on to assess genetic risk,49,50 and these data have been quoted in several subsequent reports from official international committees concerned with the potential health risks of exposure to ionizing radiation.51,52 Other examples of impact on policy and programs include reduced mortality in cardiovascular disease, asthma and many forms of cancer, increased use of folic acid in relation to heart disease, and increased supplementation of food in relation to hydrocephalus and spinal bifida. The discovery in the childhood injury surveillance program of unusual occurrences was useful in generating modifications to baby cribs to prevent further accidents.
This article retraces the history of the development of national chronic disease surveillance in Canada from 1960 to 2004. Our aim was to describe the early milestones in the development and operation of national public health surveillance in Canada. We hope that this will lead to an appreciation of the need for surveillance and act as a catalyst for progress.
Acknowledgements
We thank the 126 former staff of the LCDC at Health Canada and of Statistics Canada and the National Cancer Institute of Canada, who had participated in national chronic disease surveillance in Canada during 1960–2000, for their assistance in acquiring historical data, in many cases from their own historical records, early publications, unpublished personal transcripts and memory. We gratefully acknowledge peer reviews and constructive comments by a large number of colleagues at the Public Health Agency of Canada.
References
- 1.Hockin J. Surveillance. In: Breslow L, editor. Encyclopedia of PublicHealth. Woodbridge (CT): MacMillan Reference USA; 2001. pp. 1171–72. Quoted in Chambers LW, Ehrlich A, O'Connor KS, Edwards P, Hockin J. Health surveillance: an essential tool to protect and promote the health of the public [Internet]. Can J Public Health. 2006 [cited 2014 Apr 25];97:suppl 2-8. Available from: http://journal.cpha.ca/index.php/cjph/article/download/736/736. [Google Scholar]
- 2.Gibbard J, Bynoe ET. The Laboratory of Hygiene: a history of its development. Med Services J Can. 1967;23:1445–60. [PubMed] [Google Scholar]
- 3.The Solon Law Archive. The Constitution Act, 1867 (The British North America Act, 1867) [Internet] [modified 2009 Jun 4; cited 2014 May 9]. Available from: http://www.solon.org/Constitutions/Canada/English/ca_1867.html. [Google Scholar]
- 4.Worton D, editor. The Dominion Bureau of Statistics: a history of Canada's central statistical office and its antecedents, 1841-1972. Montréal (QC): McGill-Queen's University Press; 1998. The Statistics Act, 8-9 George V, c. 43, assented to May 24, 1918. Appendix H, pp. 331-41. [Google Scholar]
- 5.Creating a federal health department [Internet] Canadian Museum of History; 2010 Mar 31 [updated 2010 Apr 21; cited 2014 Feb 9] Available from: http://www.historymuseum.ca/cmc/exhibitions/hist/medicare/medic-1h11e.shtml. [Google Scholar]
- 6.Johansen HL. Hypertension in Canada: risk factor review and recommendations for further work. Can J Public Health. 1983;74:123–8. [PubMed] [Google Scholar]
- 7.Nichols ES, Johansen HL. Implications of changing trends in cerebrovascular and ischemic heart disease mortality. Stroke. 1983;14:153–156. doi: 10.1161/01.str.14.2.153. [DOI] [PubMed] [Google Scholar]
- 8.Wigle DT, McCourt C, Li F. Restructuring of the Chronic Disease Program at the Laboratory Centre for Disease Control. Chronic Dis Can. 1996;17((2)):74–6. [PubMed] [Google Scholar]
- 9.Gray C. Health Canada undergoes a shakeup. CMAJ. 2000;163:80–1. [PMC free article] [PubMed] [Google Scholar]
- 10.Gibbons L, Poliquin C, Fair M, Wielgosz A, Mao Y. Patterns of recurrence and survival in AMI patients in Canada. Can J Cardiol. 1993;9:661–5. [PubMed] [Google Scholar]
- 11.Nova Scotia-Saskatchewan Cardiovascular Disease Epidemiology Group Estimation of the incidence of acute myocardial infarction using record linkage: a feasibility study in Nova Scotia and Saskatchewan. Can J Public Health. 1989;80:412–7. [PubMed] [Google Scholar]
- 12.MacLean DR, Petrasovits A, Nargundkar M, et al. Canadian heart health surveys: a profile of cardiovascular risk survey methods and data analysis. CMAJ. 1992;146:1969–74. [PMC free article] [PubMed] [Google Scholar]
- 13.Gibbons L, Mao Y, Levy IG, Miller AB. The Canadian Childhood Cancer Control Program. CMAJ. 1994;151:1704–9. [PMC free article] [PubMed] [Google Scholar]
- 14.Marrett LD, King WD. Great Lakes basin cancer risk assessment: a case-control study of cancers of the bladder, colon and rectum. Ottawa (ON): Laboratory Centre for Disease Control, Health Canada; 1995. [Google Scholar]
- 15.King WD, Marrett LD, Woolcott CG. Case-control study of colon and rectal cancers and chlorination by-products in treated water. Cancer Epidemiol Biomarkers Prev. 2000;9:813–8. [PubMed] [Google Scholar]
- 16.Johnson KC, Mao Y, Argo J, Dubois S, Semenciw R, Lava J. The National Enhanced Cancer Surveillance System: a case-control approach to environment-related cancer surveillance in Canada. Environmetrics. 1998;9((5)):495–504. [Google Scholar]
- 17.Mao Y, Semenciw R, Morrison H, MacWilliam L, Davies J, Wigle D. Increased rates of illness and death from asthma in Canada. CMAJ. 1987;137:620–4. [PMC free article] [PubMed] [Google Scholar]
- 18.Mo F, Robinson C, Choi BC, Li FC. Childhood asthma management and control. Analysis of the Student Lung Health Survey (SLHS) database, Canada 1996. Int J Adolescent Med Health. 2004;16:29–40. doi: 10.1515/ijamh.2004.16.1.29. [DOI] [PubMed] [Google Scholar]
- 19.Jin R, Choi BC. The 1996 and 1997 national survey of physician asthma management practices: background and study methodology. Can Respir J. 1999;6:269–72. doi: 10.1155/1999/143258. [DOI] [PubMed] [Google Scholar]
- 20.Jin R, Choi BC, Chan BT, et al. Physician asthma management practices in Canada. Can Respir J. 2000;7:456–65. doi: 10.1155/2000/587151. [DOI] [PubMed] [Google Scholar]
- 21.Webb JF. Canadian thalidomide experience. CMAJ. 1963;89:987–92. [PMC free article] [PubMed] [Google Scholar]
- 22.Banister P. Congenital malformations: preliminary report of an investigation of reduction deformities of the limbs, triggered by a pilot surveillance system [Internet] Can Med Assoc J. 1970;103:466–72. [cited 2014 Feb 9] Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1930471/ [PMC free article] [PubMed] [Google Scholar]
- 23.Lowry RB, Thunem NY, Anderson-Redick S. Alberta Congenital Anomalies Surveillance System. CMAJ. 1989;141:1155–9. [PMC free article] [PubMed] [Google Scholar]
- 24.Paquette D, Lowry RB, Sauve R. Two to three percent of infants are born with a congenital anomaly, but who's counting? A national survey of congenital anomalies surveillance in Canada. Chronic Dis Can. 2006;27:36–8. [PubMed] [Google Scholar]
- 25.Phaneuf G, Tonmyr L. Status report: new research initiatives from the Child Maltreatment Division. Chronic Dis Can. 1998;19:71–2. [PubMed] [Google Scholar]
- 26.Fair ME, Cyr M. The Canadian Birth Data Base: a new research tool to study reproductive outcomes. Health Rep. 1993;5:281–90. [Statistics Canada, Catalogue No.: 82-003] [PubMed] [Google Scholar]
- 27.Fair ME, Carpenter M, Aylwin H. Occupational and environmental health research projects: a descriptive catalogue, 1978 to 2005 [Internet] Ottawa (ON): Statistics Canada; 2006. [cited 2013 Feb 17]. Available from: http://publications.gc.ca/Collection/Statcan/82-581-XIE/82-581-XIE2006001.pdf [Statistics Canada, Catalogue No.: 82-581-XIE] [Google Scholar]
- 28.Lindsay J, Sykes E, McDowell I, Verreault R, Laurin D. More than the epidemiology of Alzheimer's disease: contributions of the Canadian Study of Health and Aging. Can J Psychiatry. 2004;49:83–91. doi: 10.1177/070674370404900202. [DOI] [PubMed] [Google Scholar]
- 29.Gauthier S, McDowell I, Hill G. Canadian Study of Health and Aging (CaSHA) Psychiatr J Univ Ott. 1990;15:227–9. [PubMed] [Google Scholar]
- 30.McDowell I, Helliwell B, Sykes E, Hill G, Lindsay J. Study organization in the Canadian Study of Health and Aging. Int Psychogeriatr. 2001;13 Suppl 1:41–8. doi: 10.1017/s1041610202007974. [DOI] [PubMed] [Google Scholar]
- 31.Wigle DT, Mao Y, Wong T, Lane R. Economic burden of illness in Canada, 1986. Chronic Dis Can. 1991;12((3 Suppl)):1–37. [Google Scholar]
- 32.Moore R, Mao Y, Zhang J, Clarke K. Economic burden of illness in Canada, 1993. Ottawa (ON): Health Canada; 1997. [Catalogue No.: H21-136/1998E]. Catalogue no. H21-136/1993E. [PubMed] [Google Scholar]
- 33.Policy Research Division, Strategic Policy Directorate, Population and Public Health Branch, Health Canada . Economic burden of illness in Canada, 1998 [Internet] Ottawa (ON): Health Canada; 2002. [cited 2013 Aug 9]. Available from: http://www.publications.gc.ca/site/eng/448770/publication.html [Catalogue No.: H21-136/1998E] [Google Scholar]
- 34.Kendall O, Lipskie T, MacEachern S. Canadian health surveys, 1950-1997. Chronic Dis Can. 1997;18:70–90. [PubMed] [Google Scholar]
- 35.Miller AB, Howe GR, Sherman GJ, et al. Mortality from breast cancer after radiation during fluoroscopic examination in patients being treated for tuberculosis. New Engl J Med. 1989;321:1285–89. doi: 10.1056/NEJM198911093211902. [DOI] [PubMed] [Google Scholar]
- 36.Band P, Gaudette LA, Hill GB, et al. The making of the Canadian Cancer Registry: cancer incidence in Canada and its regions, 1969 to 1988. Ottawa (ON): Statistics Canada; 1993. [Google Scholar]
- 37.Gaudette LA, Lee JM. Cancer incidence in Canada, 1969-1993. Ottawa (ON): Statistics Canada. [Catalogue No.: 82-566-XPB] [Google Scholar]
- 38.Newcombe HB, Kennedy JM, Axford SJ, James AP. Automatic linkage of vital records [Internet] Science. 1959;130:954–9. doi: 10.1126/science.130.3381.954. [cited 2013 Aug 10] Available from: http://www.cs.umd.edu/class/spring2012/cmsc828L/Papers/Newcombe59.pdf. [DOI] [PubMed] [Google Scholar]
- 39.Newcombe HB. Record linking: the design of efficient systems for linking records into individual and family histories. Am J Hum Gen. 1967;19((3 Pt 1)):335–59. [cited 2013 Aug 10] Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1706275/ [PMC free article] [PubMed] [Google Scholar]
- 40.Howe GR, Lindsay J. A generalized iterative record linkage computer system for use in medical follow-up studies. Comput Biomed Res. 1981;14((4)):327–40. doi: 10.1016/0010-4809(81)90004-5. [DOI] [PubMed] [Google Scholar]
- 41.Smith ME, Newcombe HB. Automated follow-up facilities in Canada for monitoring delayed health effects. Am J Public Health. 1980;70:1261–8. doi: 10.2105/ajph.70.12.1261. [cited 2014 Jan 2] Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1619645/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Choi BC, Mowat D. Vision of a rapid, flexible, cost effective, survey-based public health surveillance system. J Epidemiol Community Health. 2001;55:612. doi: 10.1136/jech.55.9.612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Newcombe HB. Handbook of record linkage: methods for health and statistical studies, administration, and business. Oxford: Oxford University Press; 1988. [Google Scholar]
- 44.Howe GR. National Cancer Institute Monograph No. 67. Bethesda, MD: National Cancer Institute; 1985. Use of computerized record linkage in follow-up studies of cancer epidemiology in Canada; pp. 117–121. [PubMed] [Google Scholar]
- 45.Fair ME. An overview of record linkage in Canada. In: Jamerson B, Alvey W, editors. Turning administrative systems into information systems [Internet] Washington (DC): Statistics of Income, Internal Revenue Services; 1995. pp. 139–150. [cited 2013 Aug 10] [Google Scholar]
- 46.Fair ME, Lalonde P, Newcombe HB. Applications of exact ODDS for partial agreements of names in record linkage. Comput Biomed Res. 1991;24((1)):58–71. doi: 10.1016/0010-4809(91)90013-m. [DOI] [PubMed] [Google Scholar]
- 47.Johansen H, Semenciw R, Morrison H, et al. Important risk factors for death in adults: a 10-year follow-up of the Nutrition Canada survey cohort. CMAJ. 1987;136:823–8. [PMC free article] [PubMed] [Google Scholar]
- 48.Semenciw RM, Morrison HI, Mao Y, Johansen H, Davies JW, Wigle DT. Major risk factors for cardiovascular disease mortality in adults: results from the Nutrition Canada Survey cohort. Int J Epidemiol. 1988;17:317–24. doi: 10.1093/ije/17.2.317. [DOI] [PubMed] [Google Scholar]
- 49.Trimble BK, Doughty JH. The amount of hereditary disease in human populations. Ann Hum Genet. 1974;38:199–233. doi: 10.1111/j.1469-1809.1974.tb01951.x. [DOI] [PubMed] [Google Scholar]
- 50.Trimble BK, Smith ME. The incidence of genetic disease and the impact on man of an altered mutation rate. Can J Genet Cytol. 1977;19:375–85. doi: 10.1139/g77-041. [DOI] [PubMed] [Google Scholar]
- 51.United Nations Scientific Committee on the Effects of Atomic Radiation . UNSCEAR 1977 report: sources and effects of ionizing radiation [Internet] New York: United Nations; 1977. Annex H: Genetic effects of radiation; pp. 427–9. [cited 2013 Mar 1] Available from: http://www.unscear.org/docs/reports/1977,%2032nd%20session%20%28Suppl.%20No.40%29/ANNEX-H-1_unscear.pdf. [Google Scholar]
- 52.United Nations Scientific Committee on the Effects of Atomic Radiation . UNSCEAR 1982 report: ionizing radiation: sources and biological effects [Internet] New York: United Nations; 1982. pp. 543–6. [cited 2013 Feb 9] Available from: http://www.unscear.org/unscear/en/publications/1982.html. [Google Scholar]
- 53.Auditor General of Canada . Chapter 12—Department of National Health and Welfare. 1982 Report of the Auditor General of Canada. Ottawa (ON): Office of the Auditor General of Canada; 1982. [Google Scholar]
- 54.Best ER, Josie GH, Walker CB. A Canadian study of mortality in relation to smoking habits. A preliminary report. Can J Public Health. 1961;52:99–106. [Google Scholar]
- 55.Department of National Health and Welfare . A Canadian study of smoking and health. Ottawa (ON): Department of National Health and Welfare; 1966. [Google Scholar]
- 56.Justice Laws Website [Internet] Ottawa (ON): Government of Canada; Canada Health Act. (R.S.C., 1985, c. C-6) [cited 2014 Feb 9]. Available from: http://laws-lois.justice.gc.ca/eng/acts/C-6/FullText.html. [Google Scholar]
- 57.Mao Y, Semenciw R, Morrison H, Wigle DT. Seasonality in epidemics of asthma mortality and hospital admission rates, Ontario, 1979-86. Can J Public Health. 1990;81:226–8. [PubMed] [Google Scholar]
- 58.Suissa S, Ernst P, Boivin JF, et al. A cohort analysis of excess mortality in asthma and the use of inhaled beta-agonists. Am J Respir Crit Care Med. 1994;149:604–10. doi: 10.1164/ajrccm.149.3.8118625. [DOI] [PubMed] [Google Scholar]
- 59.Tough SC, Green FH, Paul JE, Wigle DT, Butt JC. Sudden death from asthma in 108 children and young adults. J Asthma. 1996;33:179–88. doi: 10.3109/02770909609054550. [DOI] [PubMed] [Google Scholar]
- 60.Wigle DT, Semenciw RM, Wilkins K, et al. Mortality study of Canadian male farm operators: non-Hodgkin's lymphoma mortality and agricultural practices in Saskatchewan. J Natl Cancer Inst. 1990;82:575–82. doi: 10.1093/jnci/82.7.575. [DOI] [PubMed] [Google Scholar]