

Abstract
Auditory training aims to compensate for degradation in the auditory signal and is offered as an intervention to help alleviate the most common complaint in people with hearing loss, understanding speech in a background noise. Yet there remain many unanswered questions. This article reviews some of the key pieces of evidence that assess the evidence for whether, and how, auditory training benefits adults with hearing loss. The evidence supports that improvements occur on the trained task; however, transfer of that learning to generalized real-world benefit is much less robust. For more than a decade, there has been an increasing awareness of the role that cognition plays in listening. But more recently in the auditory training literature, there has been an increased focus on assessing how cognitive performance relevant for listening may improve with training. We argue that this is specifically the case for measures that index executive processes, such as monitoring, attention switching, and updating of working memory, all of which are required for successful listening and communication in challenging or adverse listening conditions. We propose combined auditory-cognitive training approaches, where training interventions develop cognition embedded within auditory tasks, which are most likely to offer generalized benefits to the real-world listening abilities of people with hearing loss.
Keywords: Auditory training, hearing loss, working memory, attention, communication, hearing aids, executive function, speech perception
Learning Outcomes: As a result of this activity, the participant will be able to (1) describe four ways to assess the evidence for whether or not auditory training is effective for people with hearing loss; (2) explain how improvements on untrained speech and communication outcome measures may be attributed to executive processes (cognition).
Hearing loss results in significant difficulties in communication, which in turn can lead to social withdrawal and isolation, depression, and reduced quality of life.1 More recently, there is evidence that hearing loss is associated with an increased risk of developing dementia,2 and magnetic resonance imaging scans show that people with hearing loss have accelerated brain atrophy.3 Over the last decade, it has become increasingly evident that listening and communication require the contribution of both sensory and nonsensory factors, such as cognition, motivation, and context.4 5 6 This is particularly the case when listening to speech in adverse conditions, such as in fluctuating background noise or competing speakers,7 8 and more so in older listeners.9
To effectively communicate, whether a hearing loss is present or not, a person needs to access the acoustic information (hearing, a passive process), employ attention and intention (listening, an active process), correctly interpret the acoustic and linguistic information (comprehension, a unidirectional process), and use and transmit this information effectively (communication, a bidirectional process).10 This concept of communication, based on the World Health Organization International Classification of Functioning, Disability and Health Framework,11 has been developed further to suggest both positive and negative feedback loops exist whereby not only does improved listening result in better comprehension and communication but the converse also occurs.12 Consequently, there is an interplay between bottom-up and top-down processing that is important for successful communication. This interplay has been demonstrated empirically through physiologic and neurologic studies,13 14 15 studies of the role of cognition in hearing aid users,16 17 and in those using advanced hearing aid processing strategies, such as fast acting compression and noise reduction algorithms.18 19
Interventions for Hearing Loss
The main clinical intervention to benefit adults with hearing loss is the use of hearing aids, which provide significant benefits in terms of reduction in activity limitations (e.g., difficulties listening to speech in background noise) and participation restrictions (e.g., reduced active participation in social events).20 Despite recent advances in digital technology and improved users' satisfaction with hearing aids,21 users often continue to encounter difficulties in noisy and challenging listening environments.22 23 Furthermore, a large proportion of people who would benefit from hearing aids do not have them,24 and those who do wear hearing aids often delay seeking help, with many people having hearing difficulties for at least 10 years before obtaining hearing aids.1
When it comes to improving communication for people with hearing loss, it is clear that hearing aids alone are not the only option. A holistic approach to aural rehabilitation has been suggested,25 which includes management strategies to improve sensory deficits such as hearing aids and FM or wireless systems, instruction on technology and communication strategies, counseling to enhance participation in everyday life, and perceptual training. This review article focuses on recent developments in the field of auditory perceptual training. The article highlights work from our own laboratory, which is grounded in this literature and is aimed at improving speech perception, cognition, and self-reported communication abilities in adults with hearing loss, and identifying how improvements in these domains might best be measured.
Auditory Training and The Unanswered Questions
Auditory training as a means to compensate for the degraded auditory signal in people with hearing loss has been around since the mid-1950s, and until the mid-1990s was primarily delivered verbally, on a one-to-one basis.26 27 However, the advent of computer-based auditory training, either via PC or the Internet, provides more widespread, cost-effective, and easier-to-deliver training solutions. The added advantage of this approach is that training can be tailored to the individual's performance and conveniently delivered at home. Over the last decade, several review articles on auditory training have offered a range of different perspectives, including historical advances,27 28 rules and applications of training in adults and children,29 30 training-related changes in the brain,31 32 and conceptualization of the potential for auditory training.4 Commercial training applications for users of hearing aid and cochlear implants are listed in several articles.28 33 34
Several reviews and research articles have raised pertinent research questions (for a summary, see Table 1), but the question that has been most widely debated has been “Is auditory training effective?” This question has been directly examined by two systematic reviews. Sweetow and Palmer reviewed the literature and identified six published articles up until 1996.35 We followed this up with our own systematic review that identified 13 articles between 1996 to 2012 that used computer-based auditory training in adults with hearing loss.36 Systematic reviews differ from general literature reviews in that they ask a specific research question often using PICOS (participant, intervention, comparison, outcomes, study design) as a guide, use specific eligibility criteria and a systematic research strategy, assess the validity of the findings, and aim to provide robust evidence to support evidence-based practice. Within the hierarchy of evidence, systematic reviews, particularly if supported by a meta-analysis, provide the highest level of evidence.37
Table 1. Questions on Auditory Training Arising from the Literature.
| A. What are the optimal training parameters that provide the greatest benefits? |
| B. What are the relative benefits of auditory and cognitive training? |
| C. What are the optimal outcome measures to measure benefits of auditory training? |
| D. What is the optimal duration of training? |
| E. What are the long-term effects of training? Is booster training needed? |
| F. What factors predict benefits from training in individuals? |
| G. What are the motivations underlying adherence, and how can adherence and engagement be improved? |
| H. Can auditory training improve acclimatization in hearing aid and cochlear implant users? |
Does Auditory Training Work?
We assessed the evidence for this in a systematic review by asking several questions.36
Does Evidence Exist to Support Improvements on the Trained Task (“On-task” Learning)?
The evidence was clear that for adults with mild to moderate hearing loss, whether hearing aid users or not, on-task learning always occurred for a range of stimuli including phonemes, words, and sentences.36 The same trend was shown for cochlear implants users,36 with the exception of one study that had only 10 participants.38 That on-task learning occurs is interesting academically and supports animal models of neuroplasticity.39 However, from a clinical perspective when considering auditory training as an intervention, the following question is more relevant.
Does the Evidence Exist to Support Improvements in Untrained Measures to Provide Patient Benefit?
This is often referred to as off-task, generalized or transfer of learning. Further examination of transfer to untrained measures can be considered on a spectrum of near transfer (e.g., outcome is close to the trained task) to far transfer (e.g., outcome is in a different modality or measures a different construct). Traditionally, many training studies of adults with hearing loss have focused primarily on improving the sensory detection of auditory stimuli (e.g., identification or discrimination) to improve overall speech perception performance. The outcome measures used are often similar speech perception tasks (i.e., near transfer). However, if the aim of auditory training is to improve communication in everyday life, as seen in the models of Kiessling10 and Sweetow,12 other outcome measures that are different to the trained task and reflect real-world benefit also need to be considered. For people with hearing loss, these include both self-reported measures of communication and cognition (i.e., far transfer), both of which are important for listening.
In our systematic review,36 the generalization of learning to untrained measures was mixed. It was notable that all the studies used at least one outcome measure of speech perception, yet only two studies used a self-reported measure of communication to tap into perceived real-world benefits,12 40 and just one study measured cognition.12 Although generalized improvements were shown for speech perception (11/13 articles), self-report of communication (1/2), and cognition (1/1), these improvements were inconsistent across studies, and the magnitude of improvement was small and not robust. Similar results have been shown for speech perception in a review of mainly noncomputerized training articles from 1970 to 2009, with a small effect size (Cohen d = 0.35).41 Our systematic review highlighted that the quality of the evidence for included studies was very low to moderate. Reasons for this included failure to include a control group, power calculation, participant and tester blinding, and a lack of randomization. The study that was rated most positively for quality of evidence (moderate) was that by Sweetow and Sabes.12
Since our systematic review, several auditory training studies have addressed some of these methodological and quality issues in adults with hearing loss.42 43 44 For example, these studies all included a control group. Moreover, they used outcome measures that assess cognition (i.e., memory and attention), self-reported communication, or both. These studies will be discussed further in a later section.
Does Any Improvement in Trained and Untrained Measures Remain after Training Has Ceased (Retention of Learning)?
To assess the long-term benefits of training interventions for people with hearing loss, follow-up assessment is required. As with many intervention studies, follow-up is often not conducted.45 In our systematic review, retention of learning was assessed in 8/13 articles, and ranged from 4 days to 7 months. All studies showed retention of learning to trained and untrained measures to various degrees with only some reporting the statistical effects. Recently, other studies have demonstrated significant retention of learning,43 46 47 with the possibility of top-up sessions remaining as a means to maintain learning-related benefits.48
What Is the Adherence of Individuals with Computer-based Training?
For an intervention to be considered successful, it is crucial that individuals adhere to the intervention as this is strongly related to outcomes.49 This was highlighted in a subsample of 50 hearing aid users from a large multicenter randomized controlled trial (RCT) of Listening and Communication Enhancement (LACE) that showed those who adhered to LACE training had significantly better outcomes for untrained speech tests than those who were classified as nonadherers.50 However, our systematic review showed that adherence, like retention, was reported infrequently (only in 6/13) and defined in different ways (e.g., proportion who completed the training or proportion who dropped out). Where adherence was reported, it was high, both for laboratory-based (81%) and for home-based interventions (73 to 100%). This suggests that those who undertake home-based training, where lack of supervision might be expected to result in lower adherence, were at least as compliant as those who undertook supervised training within a laboratory setting. However, this contrasts with a large-scale study that used LACE routinely in clinical practice, where adherence was low, with only 30% completing 10 or more of the 20 sessions.51
Although there have been suggestions as to which factors are important in encouraging high adherence,51 such as clinician–patient interactions and patient motivations, to date there has been little research on this. We explored patient motivations for uptake, participation, and compliance with a home-delivered phoneme discrimination training program,43 based on the self-determination theory.52 Initial participation in the study was associated with extrinsic motivation (e.g., hearing difficulties), whereas engagement and adherence with training was influenced by intrinsic (e.g., a desire to achieve higher scores), in addition to extrinsic (e.g., to help others with hearing loss) motivations. Gaining a better understanding of users' motivations will help inform future theory-driven developments of auditory training, including the consideration of game play.53
The Importance of Clinically Significant Patient Benefits
When considering the benefits of interventions for clinical populations, it is important to understand what is meant by patient benefit. There are two points of note here: (1) clinical significance and (2) individual differences. Research studies in auditory training often report the results of improvement in terms of statistical significance. However, a study that shows a statistically significant improvement, particularly in large sample sizes, does not necessarily represent clinically significant patient benefit if the improvement is too small to impact on a patient's everyday life.54 As such, the effect size (i.e., the magnitude of improvement) is of critical importance and may be as important if not more important than statistical significance.55 Typically, effect size is described by Cohen d as small, moderate, or large (0.2, 0.5, and 0.8, respectively).56 Similarly, studies often present research findings in terms of group means, whereas in clinical practice, clinicians are faced with an individual rather than an average patient, and so individual differences are important to establish who benefits from training, and how.57
Recent Advances in Auditory Training Research on Communication and Cognitive and Speech Perception Abilities: The Role of Executive Processes
When considering outcome measures to show the benefits of auditory training and other interventions, it is important that outcome measures explicitly relate to the needs and goals of the individuals for whom the intervention is aimed at.58 Speech perception measures, particularly in noise, have been measured universally in auditory training studies of adults with hearing loss. Although it is important to demonstrate measureable improvements in speech perception performance, it is also important for those undertaking training to obtain self-perceived benefits in their everyday communication, which is best measured using self-report questionnaires.
Subjective Assessment of Communication
In our RCT of phoneme discrimination training in 44 adults with mild hearing loss,43 communication as assessed by the Glasgow Hearing Aid Benefit Profile showed a significant pre- to posttraining improvement in the overall score for hearing disability, with a moderate effect size (d = 0.51). There was no significant effect in the waitlist control (no training) group. Although this suggested that training conferred everyday real-world benefits, more interesting were the results from the four individual predefined situations. The only situation that showed a significant pre- to posttraining improvement was that for the most complex and challenging listening situation “having a conversation with several people in a group” (d = 0.68). To be able to carry out a conversation in a group, the listener is required to identify the specific speech source against a background of other talkers and to simultaneously monitor and switch attention to other auditory streams or sound sources (i.e., other talkers).8 59 This requires the engagement of executive processes that regulate, control, and manage other cognitive resources, such as attention and working memory, to aid inhibition, updating, and task switching.60 There were no significant improvements for the simpler, less challenging listening situations such as “having a conversation with one other person when there is no background noise.” If the benefits of auditory training for everyday communication are primarily evident and relevant to challenging listening situations, then to demonstrate these benefits it is important to use outcome measures that are appropriately complex and challenging to be sensitive to the effects of auditory training.
These results were supported by qualitative thematic analysis of open-ended questions from all the participants, in addition to two representative focus groups (n = 10 participants).61 From the open-ended question that asked “What was the best aspect of your experience with the training program?” around one-quarter of the participants provided unprompted reports of improved listening, concentration, and attention after they had completed the training. Furthermore, one of the key themes from the focus groups was “increased concentration, attention and focus in everyday listening.” Two subthemes were “improved listening skills” and “development of strategies for listening,” and all but one focus group participant reported that training made them concentrate more. Typical comments were:
“It [the training] made me concentrate more, it certainly did.”
“I think it just made me aware that if I do want to hear what's going off, I've got to pay attention and focus more than I used to.”
Taken together, the results from this training study suggest that the benefits of phoneme discrimination training yielded a perception of benefit, but this was only demonstrated for situations that index executive processes. To ensure that the benefits of training are captured, future training studies should carefully consider the inclusion of appropriate and sensitive outcome measures at the outset.
Behavioral Assessment of Cognition and Speech Perception
The auditory training literature suggests that people improve on what they train on, and this is also true in the cognitive training literature.62 Although the LACE program is referred to as an auditory training program, it also includes cognitive components for auditory working memory, speed of processing task, and auditory closure tasks. Two published LACE studies, one with older adults with hearing loss and the other with younger (19 to 35 years) normally hearing participant,12 63 showed statistically significant on-task learning for the auditory memory and closure tasks. Furthermore, in one study,12 generalization to improvements in untrained cognitive measures also was shown for a Listening Span test (near transfer working memory) and the Stroop Color test (far transfer speed of processing). Both these tests index executive processes.
Similar results were shown in two studies that used the Brain Fitness program (Posit Science),42 64 an auditory-based cognitive training program, with significant improvements in auditory short-term memory and sentence in noise (QuickSIN) shown for the trained but not the control groups. Additionally, there were significant improvements in auditory and visual sustained attention,64 and also in speed of processing.42 These results suggest that training also can improve the neurophysiological processes underlying speech perception in noise, specifically improvements in temporal and spectral deficits.
In our own laboratory, we have performed a series of auditory and cognitive training studies that used outcome measures of cognition, communication, and speech perception.43 65 66 These findings have been summarized elsewhere.67 For the phoneme discrimination training RCT,43 there were no pre-/posttraining improvements for simple measures of cognition (i.e., single sustained attention and simple-digit span working memory) for either the trained or control group. These results are consistent with a large study of multitask cognitive training in 11,000 participants, that showed on-task learning but no generalization to a simple-digit span working memory test.68 However, of note, our RCT showed generalized far transfer improvements, with moderate effect sizes, for complex measures of cognition that indexed executive processes.43 Specifically, these were a test of divided attention (Test of Everyday Attention [TEA]) and updating of working memory using a visual letter monitoring task. Notably, there were no improvements in the two speech tests, both of which used energetic noise maskers (i.e., digit triplets in speech-shaped noise, Adaptive Sentence List sentences in 8-Hz modulated noise).
This led us to reconsider our speech perception results and ask the question: would a speech test that engaged executive processes, such as an informational masked speech task,69 result in improvements in speech perception performance? We examined this further in a study using phoneme discrimination in noise training in existing hearing aid users.65 Significant pre-/posttraining improvements were shown for a competing speech test that used a male and a female talker (Modified Coordinate Response Measure), with a moderate effect size (d = 0.47), and no improvements for the control period. This contrasts with the results from the speech in (energetic) noise tests and suggests that it may be important to use speech measures that are relevant to the cognitive benefits provided by auditory training. Furthermore, a dual task of listening (AB words in noise) and memory (digit span)70 showed highly significant pre-/posttraining improvements with a large effect size (p < 0.001, d = 0.77), but only for an intermediate condition (0-dB signal-to-noise ratio) that was neither too easy (quiet) nor too difficult (−4-dB signal-to-noise ratio; see Fig. 1). These results were consistent with the results from our previous study for cognition and communication whereby outcome measures need to be appropriately challenging to be sensitive to posttraining benefits.43 Taken together, these results suggest that the value of auditory training to mediate top-down cognitive skills may be more important than the refinement of bottom-up sensory skills.
Figure 1.
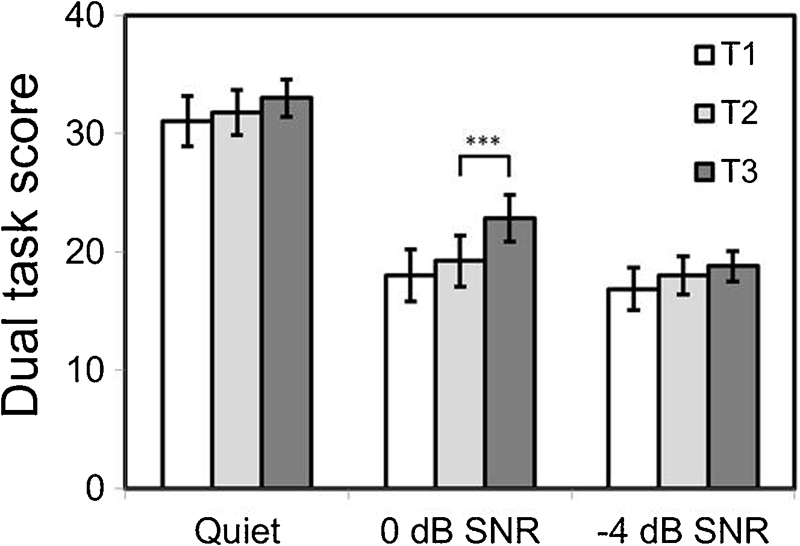
Mean and 95% confidence intervals for dual-task score (maximum value = 40) across three speech-in-noise (SNR) conditions for existing hearing aid users. Pre- and posttraining with phoneme discrimination in noise. T1 and T2 = pretraining, T3 = immediate posttraining, T1 to T2 = 1 week, T2 to T3 = 1 week. ***p = 0.001.
Finally, one of the prerequisites for an outcome measure that is used across multiple visits is that it has high test reliability to minimize measurement error. Across our two auditory training studies, test–retest reliability for cognitive and speech perception tests was generally high, and 15/18 measures exceeded an interclass correlation coefficient (ICC) of 0.7 (Table 2). However, it is noteworthy that as test complexity increases, test–retest reliability decreases. For memory, the digit span is a simple memory storage task whereas the visual monitoring tasks involve working memory and executive processing (memory updating) and have lower ICC than the digit span. For attention, the simpler single TEA task has a higher ICC than the more complex TEA dual task that has a lower ICC, which is further reflected in the differential between the two (dual task decrement). Similarly, this same trend is seen for the speech perception tests that increase in complexity from a digit triplet (word) and sentence in energetic noise to a competing speech test. This suggests that when choosing appropriate outcome measures for auditory training studies, consideration of a compromise between high sensitivity and high test–retest reliability may be warranted.
Table 2. ICC and 95% CIs for Tests of Cognition and Speech Perception from Two Auditory Training Studies.
| 95% CI | ||||
|---|---|---|---|---|
| ICC | Lower | Upper | P | |
| Ferguson et al (2014)43 | ||||
| Digit span | 0.88 | 0.70 | 0.95 | <0.001 |
| Visual monitoring task: slow (1/2 s) | 0.70 | 0.23 | 0.88 | 0.007 |
| Visual monitoring task: fast (1/1 s) | 0.72 | 0.28 | 0.89 | 0.005 |
| TEA single task (subtest 6) | 0.93 | 0.82 | 0.97 | <0.001 |
| TEA dual task (subtest 7) | 0.83 | 0.59 | 0.93 | <0.001 |
| TEA dual-task decrement | 0.72 | 0.30 | 0.89 | 0.004 |
| Digit triplet test | 0.87 | 0.66 | 0.94 | <0.001 |
| ASL sentence test | 0.67 | 0.21 | 0.86 | 0.007 |
| Henshaw and Ferguson (2014)65 | ||||
| Dual task word repetition (2 task) | 0.93 | 0.85 | 0.97 | < 0.001 |
| Quiet | 0.90 | 0.78 | 0.96 | < 0.001 |
| 0 dB | 0.80 | 0.58 | 0.91 | < 0.001 |
| −4 dB | 0.35 | −3.70 | 0.69 | 0.128 |
| Dual task digit recall (1 task) | 0.86 | 0.70 | 0.94 | < 0.001 |
| Quiet | 0.81 | 0.60 | 0.91 | < 0.001 |
| 0 dB | 0.76 | 0.49 | 0.88 | < 0.001 |
| −4 dB | 0.72 | 0.41 | 0.87 | 0.001 |
| Letter number sequencing task | 0.83 | 0.65 | 0.92 | < 0.001 |
| Competing speech (MCRM) threshold | 0.45 | 0.17 | 0.83 | 0.063 |
Abbreviations: ASL, Adaptive Sentence List; CI, confidence intervals; ICC, intraclass correlation coefficient; MCRM, Modified Coordinate Response Measure; TEA, Test of Everyday Attention.
Objective Assessment of Cognition
Studies that use objective outcome measures rather than subjective self-report and behavioral measures have the benefits of reducing any participant response or cognitive bias. One novel objective marker is pupil dilation, which has been used as a marker for the cognitive demands of listening in older adults, including those with hearing loss.71 Kuchinsky et al demonstrated that the peakedness of the pupil response increased during a word recognition task that was particularly challenging.72 In a follow-up speech perception training study,44 pupil size measured posttraining was larger and peaked more rapidly during a speech perception task. The authors suggested that increased arousal and a possible increase in attentional focus or engagement occurs as a result of training. Other electrophysiologic measures, such as α waves,73 also may be a marker of attention or engagement with a task, and offer a potential measure of changes in the cognitive resources required for listening following auditory training.
What About Training Cognition Directly?
Given that cognition appears to play a critical role in pre- to post-auditory training benefits, can training cognition offer a more direct route for people with hearing loss? Studies of a commercial working memory training program (Cogmed RM) have shown generalized posttraining improvements for attention and self-report of cognition in younger and older adults and speech perception in children with cochlear implants.74 75 To date, there have been no published studies of Cogmed RM in adults with mild to moderate hearing loss.
Our third training study was a registered clinical RCT using Cogmed RM in a sample of 57 existing hearing aid users.66 Cogmed RM uses an adaptive paradigm for the trained group and a fixed three-item span paradigm for the active control group, which allowed blinding of both the participants and the researchers. The results, not yet published, showed that there was near transfer for an untrained working memory task but no far transfer to a cognitively two-competing talker speech perception task (informational masking). These results are broadly consistent with the cognitive neuroscience literature. A systematic review of 52 cognitive training studies showed statistically significant differences for those undergoing cognitive training compared to control groups, with small and moderate effect sizes for nonverbal and verbal memory, working memory, and processing speed.62 However, there were no significant effects seen for executive function and attention, indicating no generalization to the broader underlying cognitive constructs.76 Working memory training enhances working memory tasks that have a similar underlying cognitive construct and share similar structural features.77 It may be that training-related improvements in working memory are mediated by specific strategies that are employed by participants, such as chunking or grouping.78
Where To Next?
People improve on what they train on, whether the training stimuli are auditory or cognitive. Generalization of learning to untrained tasks is more uncertain, although more likely to occur for near transfer than far transfer. A theme that seems to be coming to the fore is the role of cognition in auditory training, specifically executive processes such as attention switching and updating of memory. These are processes that are integral for successful listening in challenging or adverse conditions, therefore training stimuli that engage these processes may well be the key to providing benefits from training programs.
To optimize the benefits of training to everyday real-world communication, we propose that an integrated auditory-cognitive approach is taken. Training would, for example, target the cognitive processes that underpin speech perception within speech tasks rather than directly training cognition, which is far removed from speech perception or speech-in-noise perception that has limited cognitive involvement (e.g., uses energetic masking).
Reviewing the unanswered questions posed in Table 1, there appears to be some headway made in addressing questions A to C. Training parameters in auditory stimuli that engage executive processes rather than cognitive training in isolation may provide greater real-world benefits. The benefits of auditory training may be best demonstrated if outcome measures are appropriate and sensitive to the underlying mechanisms of benefit, such as those that underpin executive processes. Further research is needed to specifically address these hypotheses, and of course, many questions remain unanswered.
Returning to the main problem that many people with hearing loss experience, that of listening to speech in background noise. A holistic rehabilitative approach that aims to reduce activity limitations and participation restrictions has been suggested by Boothroyd.25 We would like to propose that for rehabilitation, auditory training is expanded to target both listening and communication abilities through appropriately designed training programs that enhance cognition, specifically executive processes. Furthermore, this training should be delivered in a way that promotes both intrinsic and extrinsic motivations of the user to enhance enjoyment and adherence. This type of approach would be best considered in conjunction with hearing aids and management strategies outside of the scope of this article. Such strategies may include individualized educational programs that encourage active engagement of the patient with educational materials to enhance knowledge of hearing loss, hearing aids, and effective communication,79 80 81 appropriate setting of expectations, patient motivations, and shared goal-setting,82 alongside the active inclusion of patients' communication partners.83
Finally, with the increasing use of the Internet and smartphone technologies, even in older people,84 and the growing interest in the concept of tele-audiology, auditory-cognitive training is ideally suited for online delivery that can be tailored to meet an individual's needs, can be easily accessed when needed, with increased game play and interaction elements, and delivered alongside other hearing management strategies.85 But that's another story, for another day.
Acknowledgments
This article presents independent research funded by the National Institute for Health Research (NIHR) Biomedical Research Unit Program. The views expressed are those of the authors and not necessarily those of the National Health Service, the NIHR, or the Department of Health. There are no conflicts of interest.
References
- 1.Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I. Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models. Health Technol Assess. 2007;11(42):1–294. doi: 10.3310/hta11420. [DOI] [PubMed] [Google Scholar]
- 2.Lin F R, Metter E J, O'Brien R J, Resnick S M, Zonderman A B, Ferrucci L. Hearing loss and incident dementia. Arch Neurol. 2011;68(2):214–220. doi: 10.1001/archneurol.2010.362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lin F R, Ferrucci L, An Y. et al. Association of hearing impairment with brain volume changes in older adults. Neuroimage. 2014;90:84–92. doi: 10.1016/j.neuroimage.2013.12.059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Boothroyd A. Adapting to changed hearing: the potential role of formal training. J Am Acad Audiol. 2010;21(9):601–611. doi: 10.3766/jaaa.21.9.6. [DOI] [PubMed] [Google Scholar]
- 5.Pichora-Fuller M K, Singh G. Effects of age on auditory and cognitive processing: implications for hearing aid fitting and audiologic rehabilitation. Trends Amplif. 2006;10(1):29–59. doi: 10.1177/108471380601000103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tun P A, Williams V A, Small B J, Hafter E R. The effects of aging on auditory processing and cognition. Am J Audiol. 2012;21(2):344–350. doi: 10.1044/1059-0889(2012/12-0030). [DOI] [PubMed] [Google Scholar]
- 7.Akeroyd M A. Are individual differences in speech reception related to individual differences in cognitive ability? A survey of twenty experimental studies with normal and hearing-impaired adults. Int J Audiol. 2008;47 02:S53–S71. doi: 10.1080/14992020802301142. [DOI] [PubMed] [Google Scholar]
- 8.Shinn-Cunningham B G, Best V. Selective attention in normal and impaired hearing. Trends Amplif. 2008;12(4):283–299. doi: 10.1177/1084713808325306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Moore D R, Edmondson-Jones M, Dawes P. et al. Relation between speech-in-noise threshold, hearing loss and cognition from 40–69 years of age. PLoS ONE. 2014;9(9):e107720. doi: 10.1371/journal.pone.0107720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kiessling J, Pichora-Fuller M K, Gatehouse S. et al. Candidature for and delivery of audiological services: special needs of older people. Int J Audiol. 2003;42 02:S92–S101. [PubMed] [Google Scholar]
- 11.WHO . Geneva, Switzerland: WHO; 2001. International Classification of Functioning, Disability and Health: ICF. [Google Scholar]
- 12.Sweetow R W, Sabes J H. The need for and development of an adaptive Listening and Communication Enhancement (LACE) program. J Am Acad Audiol. 2006;17(8):538–558. doi: 10.3766/jaaa.17.8.2. [DOI] [PubMed] [Google Scholar]
- 13.Anderson S, White-Schwoch T, Parbery-Clark A, Kraus N. A dynamic auditory-cognitive system supports speech-in-noise perception in older adults. Hear Res. 2013;300:18–32. doi: 10.1016/j.heares.2013.03.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.de Boer J, Thornton A RD. Neural correlates of perceptual learning in the auditory brainstem: efferent activity predicts and reflects improvement at a speech-in-noise discrimination task. J Neurosci. 2008;28(19):4929–4937. doi: 10.1523/JNEUROSCI.0902-08.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tremblay K L, Billings C J, Friesen L M, Souza P E. Neural representation of amplified speech sounds. Ear Hear. 2006;27(2):93–103. doi: 10.1097/01.aud.0000202288.21315.bd. [DOI] [PubMed] [Google Scholar]
- 16.Lunner T. Cognitive function in relation to hearing aid use. Int J Audiol. 2003;42 01:S49–S58. doi: 10.3109/14992020309074624. [DOI] [PubMed] [Google Scholar]
- 17.Gatehouse S, Naylor G, Elberling C. Benefits from hearing aids in relation to the interaction between the user and the environment. Int J Audiol. 2003;42 01:S77–S85. doi: 10.3109/14992020309074627. [DOI] [PubMed] [Google Scholar]
- 18.Lunner T, Sundewall-Thorén E. Interactions between cognition, compression, and listening conditions: effects on speech-in-noise performance in a two-channel hearing aid. J Am Acad Audiol. 2007;18(7):604–617. doi: 10.3766/jaaa.18.7.7. [DOI] [PubMed] [Google Scholar]
- 19.Sarampalis A, Kalluri S, Edwards B, Hafter E. Objective measures of listening effort: effects of background noise and noise reduction. J Speech Lang Hear Res. 2009;52(5):1230–1240. doi: 10.1044/1092-4388(2009/08-0111). [DOI] [PubMed] [Google Scholar]
- 20.Chisolm T H, Johnson C E, Danhauer J L. et al. A systematic review of health-related quality of life and hearing aids: final report of the American Academy of Audiology Task Force on the Health-Related Quality of Life Benefits of Amplification in Adults. J Am Acad Audiol. 2007;18(2):151–183. doi: 10.3766/jaaa.18.2.7. [DOI] [PubMed] [Google Scholar]
- 21.Kochkin S. MarkeTrak VIII: consumer satisfaction with hearing aids is slowly increasing. Hearing J. 2010;63(1):19–20. [Google Scholar]
- 22.Johnson E E, Dillon H. A comparison of gain for adults from generic hearing aid prescriptive methods: impacts on predicted loudness, frequency bandwidth, and speech intelligibility. J Am Acad Audiol. 2011;22(7):441–459. doi: 10.3766/jaaa.22.7.5. [DOI] [PubMed] [Google Scholar]
- 23.Dubno J R. Benefits of auditory training for aided listening by older adults. Am J Audiol. 2013;22(2):335–338. doi: 10.1044/1059-0889(2013/12-0080). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.World Health Organization Deafness and hearing loss 2015. Available at: http://www.who.int/mediacentre/factsheets/fs300/en/. Accessed April 14, 2015
- 25.Boothroyd A. Adult aural rehabilitation: what is it and does it work? Trends Amplif. 2007;11(2):63–71. doi: 10.1177/1084713807301073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bamford J. Auditory train. What is it, what is it supposed to do, and does it do it? Br J Audiol. 1981;15(2):75–78. doi: 10.3109/03005368109081418. [DOI] [PubMed] [Google Scholar]
- 27.Kricos P B, McCarthy P. From ear to there: a historical perspective on auditory training. Semin Hear. 2007;28(2):89–98. [Google Scholar]
- 28.Pichora-Fuller M K, Levitt H. Speech comprehension training and auditory and cognitive processing in older adults. Am J Audiol. 2012;21(2):351–357. doi: 10.1044/1059-0889(2012/12-0025). [DOI] [PubMed] [Google Scholar]
- 29.Moore D R, Amitay S. Auditory training: rules and applications. Semin Hear. 2007;28(2):99–109. [Google Scholar]
- 30.Moore D R, Halliday L F, Amitay S. Use of auditory learning to manage listening problems in children. Philos Trans R Soc Lond B Biol Sci. 2009;364(1515):409–420. doi: 10.1098/rstb.2008.0187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tremblay K. Training-related changes in the brain: evidence from human auditory-evoked potentials. Semin Hear. 2007;28(2):120–132. [Google Scholar]
- 32.Anderson S, Kraus N. Auditory training: evidence for neural plasticity in older adults. . Perspect Hear Hear Disord Res Res Diagn. 2013;17(1):37–57. doi: 10.1044/hhd17.1.37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pizarek R, Shafiro V, McCarthy P. Effect of computerized auditory training on speech perception of adults with hearing impairment. Perspectives. 2013;20(3):91–106. [Google Scholar]
- 34.Zhang M, Miller A, Campbell M M. Overview of nine computerized, home-based auditory-training programs for adult cochlear implant recipients. J Am Acad Audiol. 2014;25(4):405–413. doi: 10.3766/jaaa.25.4.11. [DOI] [PubMed] [Google Scholar]
- 35.Sweetow R, Palmer C V. Efficacy of individual auditory training in adults: a systematic review of the evidence. J Am Acad Audiol. 2005;16(7):494–504. doi: 10.3766/jaaa.16.7.9. [DOI] [PubMed] [Google Scholar]
- 36.Henshaw H, Ferguson M A. Efficacy of individual computer-based auditory training for people with hearing loss: a systematic review of the evidence. PLoS ONE. 2013;8(5):e62836. doi: 10.1371/journal.pone.0062836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wong L L, Hickson L. San Diego, CA: Plural Publishing; 2012. Evidence-Based Practice in Audiology: Evaluating Interventions for Children and Adults with Hearing Impairment. [Google Scholar]
- 38.Stacey P C, Raine C H, O'Donoghue G M, Tapper L, Twomey T, Summerfield A Q. Effectiveness of computer-based auditory training for adult users of cochlear implants. Int J Audiol. 2010;49(5):347–356. doi: 10.3109/14992020903397838. [DOI] [PubMed] [Google Scholar]
- 39.Recanzone G H, Schreiner C E, Merzenich M M. Plasticity in the frequency representation of primary auditory cortex following discrimination training in adult owl monkeys. J Neurosci. 1993;13(1):87–103. doi: 10.1523/JNEUROSCI.13-01-00087.1993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ingvalson E M, Lee B, Fiebig P, Wong P C. The effects of short-term computerized speech-in-noise training on postlingually deafened adult cochlear implant recipients. J Speech Lang Hear Res. 2013;56(1):81–88. doi: 10.1044/1092-4388(2012/11-0291). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chisolm T, Arnold M. San Diego, CA: Plural Publishing; 2012. Evidence about the effectiveness of aural rehabilitation programs for adults. [Google Scholar]
- 42.Anderson S, White-Schwoch T, Parbery-Clark A, Kraus N. Reversal of age-related neural timing delays with training. Proc Natl Acad Sci U S A. 2013;110(11):4357–4362. doi: 10.1073/pnas.1213555110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ferguson M A, Henshaw H, Clark D P, Moore D R. Benefits of phoneme discrimination training in a randomized controlled trial of 50- to 74-year-olds with mild hearing loss. Ear Hear. 2014;35(4):e110–e121. doi: 10.1097/AUD.0000000000000020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kuchinsky S E, Ahlstrom J B, Cute S L, Humes L E, Dubno J R, Eckert M A. Speech-perception training for older adults with hearing loss impacts word recognition and effort. Psychophysiology. 2014;51(10):1046–1057. doi: 10.1111/psyp.12242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Barker F, Mackenzie E, Elliott L, Jones S, de Lusignan S. Interventions to improve hearing aid use in adult auditory rehabilitation. Cochrane Database Syst Rev. 2014;7:CD010342. doi: 10.1002/14651858.CD010342.pub2. [DOI] [PubMed] [Google Scholar]
- 46.Brown D J, Proulx M J. Increased signal complexity improves the breadth of generalization in auditory perceptual learning. Neural Plast. 2013;2013:879047. doi: 10.1155/2013/879047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Schumann A, Serman M, Gefeller O, Hoppe U. Computer-based auditory phoneme discrimination training improves speech recognition in noise in experienced adult cochlear implant listeners. Int J Audiol. 2015;54(3):190–198. doi: 10.3109/14992027.2014.969409. [DOI] [PubMed] [Google Scholar]
- 48.Burk M H, Humes L E, Amos N E, Strauser L E. Effect of training on word-recognition performance in noise for young normal-hearing and older hearing-impaired listeners. Ear Hear. 2006;27(3):263–278. doi: 10.1097/01.aud.0000215980.21158.a2. [DOI] [PubMed] [Google Scholar]
- 49.DiMatteo M R, Giordani P J, Lepper H S, Croghan T W. Patient adherence and medical treatment outcomes: a meta-analysis. Med Care. 2002;40(9):794–811. doi: 10.1097/00005650-200209000-00009. [DOI] [PubMed] [Google Scholar]
- 50.Chisolm T H, Saunders G H, Frederick M T, McArdle R A, Smith S L, Wilson R H. Learning to listen again: the role of compliance in auditory training for adults with hearing loss. Am J Audiol. 2013;22(2):339–342. doi: 10.1044/1059-0889(2013/12-0081). [DOI] [PubMed] [Google Scholar]
- 51.Sweetow R W, Sabes J H. Auditory training and challenges associated with participation and compliance. J Am Acad Audiol. 2010;21(9):586–593. doi: 10.3766/jaaa.21.9.4. [DOI] [PubMed] [Google Scholar]
- 52.Deci E, Ryan R. New York, NY: Plenum Press; 1985. Intrinsic Motivation and Self-Regulation in Human Behavior. [Google Scholar]
- 53.Bavelier D, Davidson R J. Games to do you good: neuroscientists should help to develop compelling videogames that boost brain function and improve well-being. Nature. 2013;494:425–426. doi: 10.1038/494425a. [DOI] [PubMed] [Google Scholar]
- 54.Ferguson M, Henshaw H. Auditory training as an intervention for adults with hearing loss; the current state of play. ENT Audiol News. 2011;20(4):104–106. [Google Scholar]
- 55.Sedgwick P. Clinical significance versus statistical significance. BMJ. 2014;348:g2130. [Google Scholar]
- 56.Cohen J. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. Statistical Power Analysis for the Behavioral Sciences, 2nd ed. [Google Scholar]
- 57.Humes L E. Individual differences research and hearing aid outcomes. Semin Hear. 2013;34(02):67–73. [Google Scholar]
- 58.Gatehouse S. Rehabilitation: identification of needs, priorities and expectations, and the evaluation of benefit. Int J Audiol. 2003;42(2) 02:S77–S83. [PubMed] [Google Scholar]
- 59.Gatehouse S, Noble W. The Speech, Spatial and Qualities of Hearing Scale (SSQ) Int J Audiol. 2004;43(2):85–99. doi: 10.1080/14992020400050014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Chan R CK, Shum D, Toulopoulou T, Chen E YH. Assessment of executive functions: review of instruments and identification of critical issues. Arch Clin Neuropsychol. 2008;23(2):201–216. doi: 10.1016/j.acn.2007.08.010. [DOI] [PubMed] [Google Scholar]
- 61.Henshaw H, McCormack A, Ferguson M A. Intrinsic and extrinsic motivation drives computer-based auditory training uptake, engagement, and adherence for people with hearing loss. Frontiers in Psychology. 2015;6(1067):1–13. doi: 10.3389/fpsyg.2015.01067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Lampit A, Hallock H, Valenzuela M. Computerized cognitive training in cognitively healthy older adults: a systematic review and meta-analysis of effect modifiers. PLoS Med. 2014;11(11):e1001756. doi: 10.1371/journal.pmed.1001756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Song J H, Skoe E, Banai K, Kraus N. Training to improve hearing speech in noise: biological mechanisms. Cereb Cortex. 2012;22(5):1180–1190. doi: 10.1093/cercor/bhr196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Anderson S, White-Schwoch T, Choi H J, Kraus N. Training changes processing of speech cues in older adults with hearing loss. Front Syst Neurosci. 2013;7(97):97. doi: 10.3389/fnsys.2013.00097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Henshaw H Ferguson M A Assessing the benefits of auditory training to real-world listening: identifying appropriate and sensitive outcomes. Paper presented at: Proceedings of ISAAR 2013: Auditory Plasticity—Listening with the Brain 4th Symposium on Auditory and Audiological Research. Nyborg, Denmark; 2014
- 66.Henshaw H, Ferguson M A. Working memory training for adult hearing aid users: study protocol for a double-blind randomized active controlled trial. Trials. 2013;14(1):417. doi: 10.1186/1745-6215-14-417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Ferguson M A, Henshaw H. Auditory training can improve working memory, attention, and communication in adverse conditions for adults with hearing loss. Front Psychol. 2015;6:556. doi: 10.3389/fpsyg.2015.00556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Owen A M, Hampshire A, Grahn J A. et al. Putting brain training to the test. Nature. 2010;465(7299):775–778. doi: 10.1038/nature09042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Shinn-Cunningham B G. Object-based auditory and visual attention. Trends Cogn Sci. 2008;12(5):182–186. doi: 10.1016/j.tics.2008.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Howard C S, Munro K J, Plack C J. Listening effort at signal-to-noise ratios that are typical of the school classroom. Int J Audiol. 2010;49(12):928–932. doi: 10.3109/14992027.2010.520036. [DOI] [PubMed] [Google Scholar]
- 71.Zekveld A A, Kramer S E, Festen J M. Cognitive load during speech perception in noise: the influence of age, hearing loss, and cognition on the pupil response. Ear Hear. 2011;32(4):498–510. doi: 10.1097/AUD.0b013e31820512bb. [DOI] [PubMed] [Google Scholar]
- 72.Kuchinsky S E, Ahlstrom J B, Vaden K I Jr. et al. Pupil size varies with word listening and response selection difficulty in older adults with hearing loss. Psychophysiology. 2013;50(1):23–34. doi: 10.1111/j.1469-8986.2012.01477.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Petersen E B, Wöstmann M, Obleser J, Stenfelt S, Lunner T. Hearing loss impacts neural alpha oscillations under adverse listening conditions. Front Psychol. 2015;6:177. doi: 10.3389/fpsyg.2015.00177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Brehmer Y, Westerberg H, Bäckman L. Working-memory training in younger and older adults: training gains, transfer, and maintenance. Front Hum Neurosci. 2012;6(63):63. doi: 10.3389/fnhum.2012.00063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kronenberger W G, Pisoni D B, Henning S C, Colson B G, Hazzard L M. Working memory training for children with cochlear implants: a pilot study. J Speech Lang Hear Res. 2011;54(4):1182–1196. doi: 10.1044/1092-4388(2010/10-0119). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Melby-Lervåg M, Hulme C. Is working memory training effective? A meta-analytic review. Dev Psychol. 2013;49(2):270–291. doi: 10.1037/a0028228. [DOI] [PubMed] [Google Scholar]
- 77.Thompson T W, Waskom M L, Garel K L. et al. Failure of working memory training to enhance cognition or intelligence. PLoS ONE. 2013;8(5):e63614. doi: 10.1371/journal.pone.0063614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Dunning D L, Holmes J. Does working memory training promote the use of strategies on untrained working memory tasks? Mem Cognit. 2014;42(6):854–862. doi: 10.3758/s13421-014-0410-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Ferguson M Brandreth M Leighton P Brassington W Wharrad H A randomised controlled trial to evaluate the benefits of a multimedia educational programme for first-time hearing aid users Ear Hear [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Thorén E S, Öberg M, Wänström G, Andersson G, Lunner T. A randomized controlled trial evaluating the effects of online rehabilitative intervention for adult hearing-aid users. Int J Audiol. 2014;53(7):452–461. doi: 10.3109/14992027.2014.892643. [DOI] [PubMed] [Google Scholar]
- 81.Hickson L, Worrall L, Scarinci N. A randomized controlled trial evaluating the active communication education program for older people with hearing impairment. Ear Hear. 2007;28(2):212–230. doi: 10.1097/AUD.0b013e31803126c8. [DOI] [PubMed] [Google Scholar]
- 82.Laplante-Levesque A, Hickson L, Worrall L. A qualitative study of shared decision making in rehabilitative audiology. J Acad Rehabilitative Audiol. 2010;43:27–43. [Google Scholar]
- 83.Kamil R J, Lin F R. The effects of hearing impairment in older adults on communication partners: a systematic review. J Am Acad Audiol. 2015;26(2):155–182. doi: 10.3766/jaaa.26.2.6. [DOI] [PubMed] [Google Scholar]
- 84.Deloitte The smartphone generation gap: over 55? There's no app for that Available at: http://www2.deloitte.com/content/dam/Deloitte/global/Documents/Technology-Media-Telecommunications/gx-tmt-2014prediction-smartphone.pdf2014. Accessed December 10, 2014
- 85.Ferguson M Henshaw H Computer and Internet interventions to optimise listening and learning for people with hearing loss: accessibility, use and adherence Am J Audiol In press [DOI] [PubMed] [Google Scholar]