

Abstract
We present a technique for anterior cruciate ligament (ACL) reconstruction using hamstring tendon autograft with preserved tibial insertions. The tendons, harvested with an open-ended tendon stripper while their tibial insertions are preserved, are looped around to prepare a quadrupled graft. The femoral tunnel is drilled independently through a transportal technique, whereas the tibial tunnel is drilled in a standard manner. The length of the quadrupled graft and loop of the RetroButton is adjusted so that it matches the calculated length of both tunnels and the intra-articular part of the proposed ACL graft. After the RetroButton is flipped, the graft is manually tensioned with maximal stretch on the free end, which is then sutured to the other end with preserved insertions. We propose that preserving the insertions is more biological and may provide better proprioception. The technique eliminates the need for a tibial-side fixation device, thus reducing the cost of surgery. Furthermore, tibial-side fixation of the free graft is the weakest link in the overall stiffness of the reconstructed ACL, and this technique circumvents this problem. Postoperative mechanical stability and functional outcome with this technique need to be explored and compared with those of ACL reconstruction using free hamstring autograft.
The most common surgical treatment for an anterior cruciate ligament (ACL)–deficient knee is reconstruction of the ligament using an autograft, either a quadrupled semitendinosus and gracilis (STG) tendon free hamstring graft or a free bone–patellar tendon–bone graft.1 The objective mechanical stability of a reconstructed ACL ranges from 85% to 90%,2 and this has correlated poorly with functional outcome; lack of proprioception is thought to be one of the reasons for poor correlation.3, 4, 5, 6, 7 Furthermore, tibial-side fixation of the free graft has been observed to be the weakest link in the overall stiffness of the construct of the reconstructed ACL.8, 9 We hypothesized that using a technique that preserves the insertions of the hamstring tendons on the tibial side would eliminate the disadvantages of a free graft, such as poor proprioception, tibial-side fixation being the weakest link in the overall construct, and the added cost of using a tibial-side fixation device for a free graft.
Technique
An oblique incision is performed, positioned proximal and medial to the insertion of the pes anserinus (Video 1). The infrapatellar branch of the saphenous nerve is preserved. A nick is made on the sartorius fascia. The insertions of the STG tendons are identified, and any associated fascial bands are carefully dissected with forceps, scissors, and finger dissection. With the tibial insertions of the tendons left intact, an open-ended tendon stripper is used to harvest the graft (Fig 1). The proximal free ends of the tendons are sutured together by wrapping the broader aponeurosis of the semitendinosus around the gracilis tendon using No. 5 Ethibond suture (Ethicon, Somerville, NJ). The tendons are looped around a No. 5 Ethibond suture, thus creating a quadrupled graft. The graft is sized with a sizer. Standard anterolateral and far-medial arthroscopic portals are made. The femoral point of entry is marked with a bone awl at the junction of the lateral condylar ridge and bifurcate ridge using arthroscopic guidance (Fig 2). A guide pin is introduced into the femur. With the knee in maximal hyperflexion, a 4.5-mm cannulated drill bit is used to create a tunnel in the femur (Fig 3). The length of the tunnel (length A) is measured with a depth gauge (Fig 4, Fig 5). Reaming of the tunnel is performed with a femoral reamer corresponding to the size of the quadrupled tendon. No. 5 Ethibond suture is passed into the tunnel and the loop parked inside the joint (Fig 6). The tibial tunnel is drilled in a routine manner using an ACL tibial guide (Fig 7). The Ethibond suture loop placed through the femoral tunnel into the joint is retrieved from the tibial tunnel with a grasper (Fig 8). The length of the tibial tunnel and the intra-articular part of the proposed ACL graft (length B) is measured with a depth gauge (Fig 5, Fig 9); this length is added to the already measured length of the femoral tunnel to determine the exact length of both tunnels plus the intra-articular portion of the graft (length A plus length B). A marking suture is placed on the hamstring tendons just opposite the entry of the tibial tunnel so that when the graft is pulled inside the joint, the mark stays at the entry of the tunnel (Fig 10). A RetroButton (Arthrex, Naples, FL) is loaded onto the quadrupled graft. The length of the quadrupled graft and loop of the RetroButton is adjusted so that it exactly corresponds to length A plus length B (Fig 11). The sutures of the RetroButton are pulled through the tibial and femoral tunnels by loading them onto the Ethibond loop placed in the tunnels (Fig 12). The RetroButton is flipped outside the femoral tunnel onto the cortex. The free end of the graft exiting the tibial tunnel is pulled to maximal stretch and the joint moved through full range of motion at least 10 times to remove any kinks in the graft (Fig 13). The tightness of the ACL graft is checked arthroscopically with a probe. With maximal stretch on the free end of the graft, it is sutured to the preserved end (Fig 14).
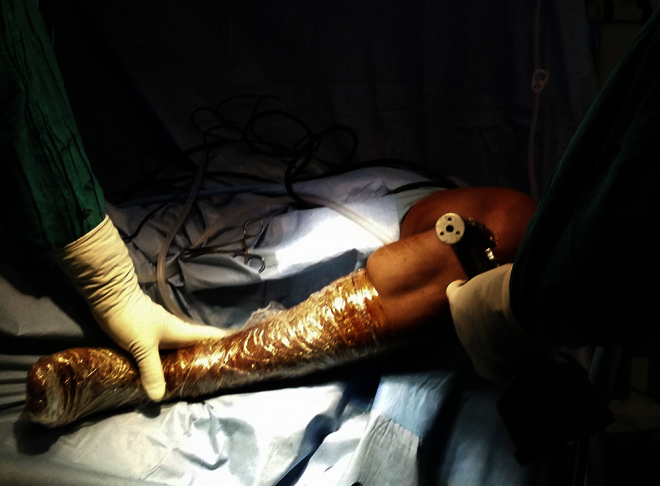
Fig 1.

With the tibial insertions of the tendons left intact, an open-ended tendon stripper is used to harvest the graft.
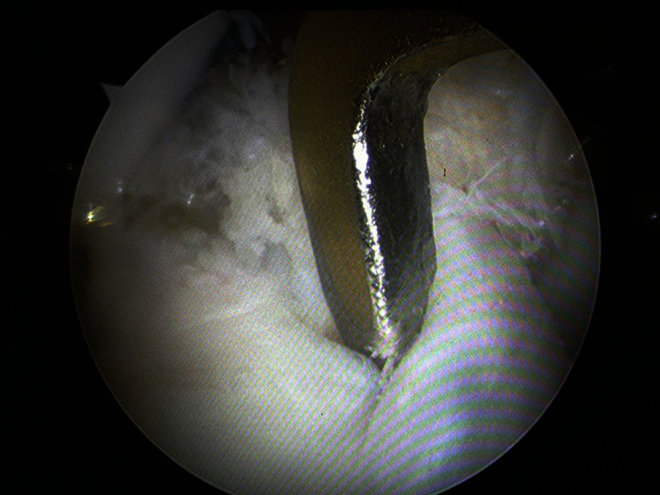
Fig 2.
The femoral point of entry is marked with a bone awl at the junction of the lateral condylar ridge and bifurcate ridge with arthroscopic guidance.
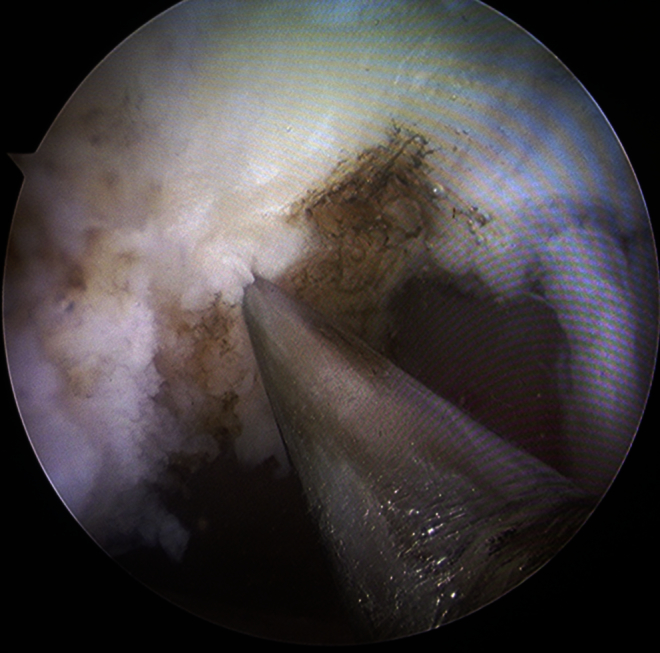
Fig 3.
A guide pin is introduced into the femur, and with the knee in maximal hyperflexion, a 4.5-mm cannulated drill bit is used to create a tunnel in the femur.
Fig 4.
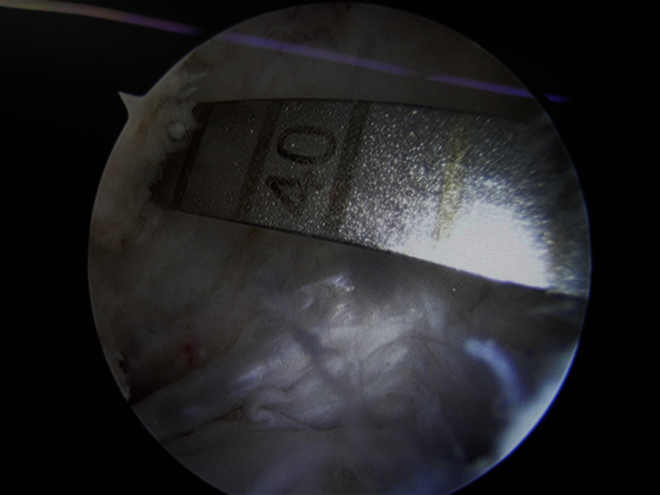
The length of the tunnel is measured with a depth gauge.
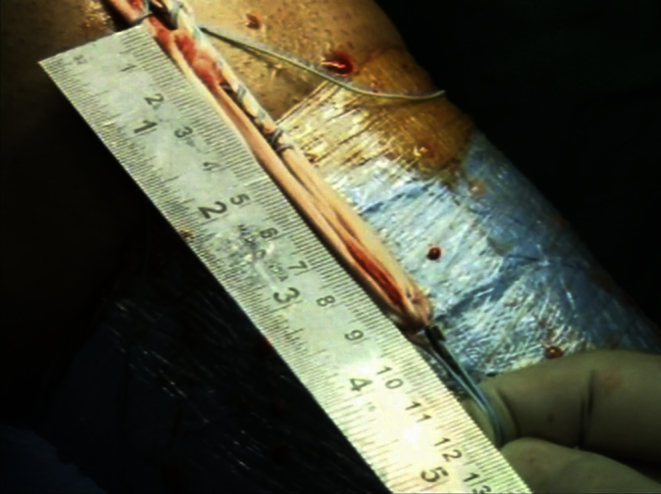
Fig 5.
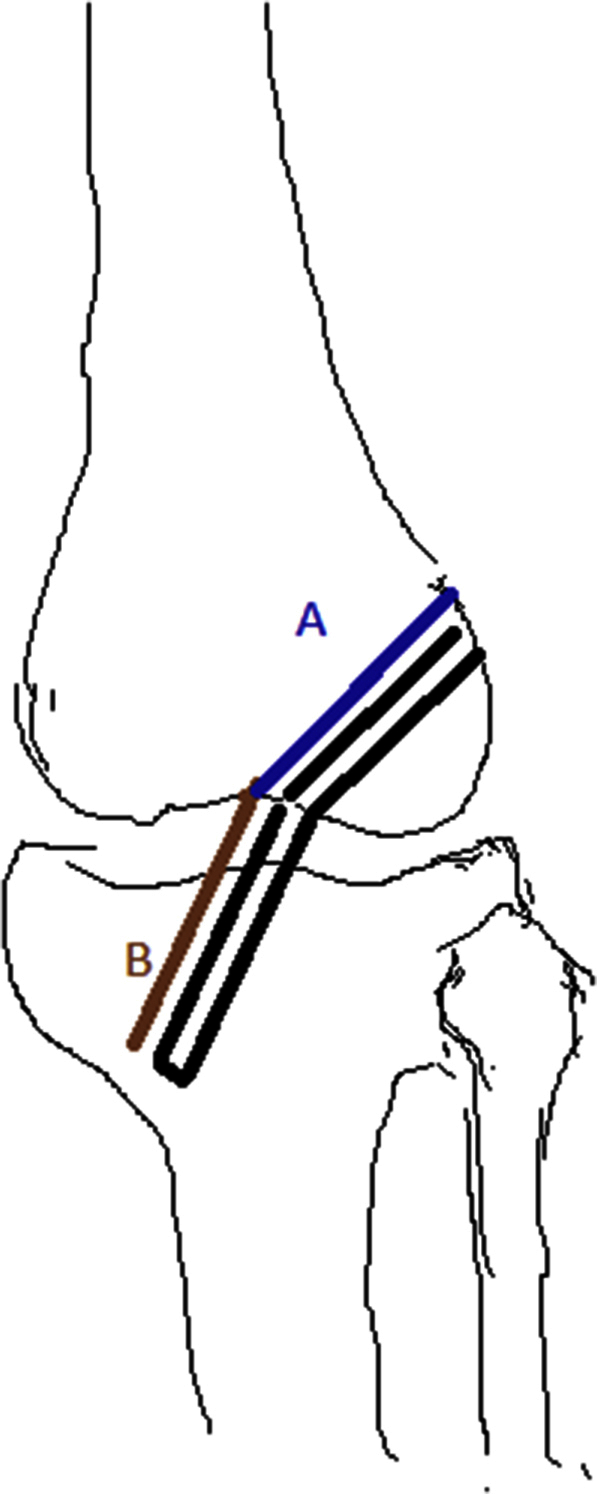
Length of femoral tunnel (length A) and length of tibial tunnel plus intra-articular part of graft (length B).
Fig 6.

No. 5 Ethibond suture (left arrow) is passed into the tunnel, and the loop (right arrow) is parked inside the joint.
Fig 7.
By use of an anterior cruciate ligament tibial guide, the tibial tunnel is reamed.
Fig 8.

The Ethibond suture loop placed through the femoral tunnel into the joint is retrieved from the tibial tunnel with a grasper.
Fig 9.

The length of the tibial tunnel and the intra-articular part of the proposed anterior cruciate ligament graft is measured with a depth gauge.
Fig 10.
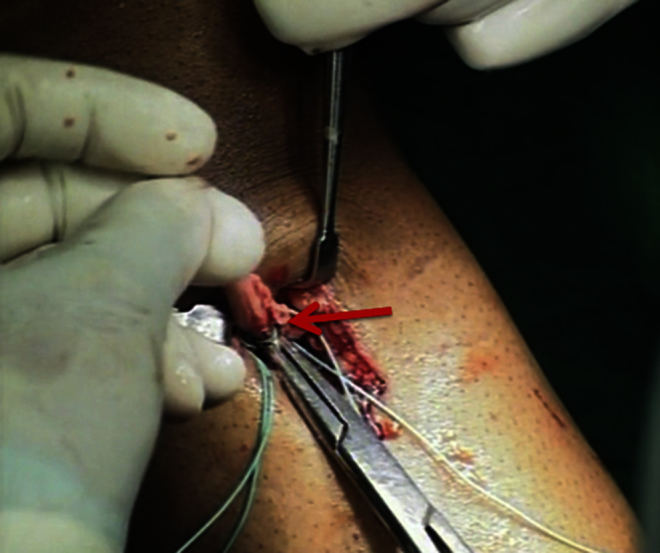
A marking suture (arrow) is placed on the hamstring tendons just opposite the entry of the tibial tunnel so that when the graft is pulled inside the joint, the mark stays at the entry of the tunnel.
Fig 11.
The length of the quadrupled graft and loop of the RetroButton is adjusted so that it exactly corresponds to length A (length of femoral tunnel) plus length B (length of tibial tunnel plus intra-articular part of graft).
Fig 12.

The sutures of the RetroButton are pulled through the tibial and femoral tunnels by loading them onto the Ethibond loop placed in the tunnels.
Fig 13.

The free end of the graft exiting the tibial tunnel is pulled to maximal stretch and the joint moved through full range of motion at least 10 times to remove any kinks in the graft.
Fig 14.

With maximal stretch on the free end of the graft, it is sutured to the preserved end.
Discussion
Kim et al.10 in 1997 proposed the preservation of the tibial insertions of the STG tendons while harvesting the graft, with an additional fixation by a double spiked washer on the tibial side. In 2010 a new technique was developed in which the STG graft was harvested while solely relying on the tibial insertions of the hamstring tendons and femoral fixation of the graft was achieved with 2 bioabsorbable RigidFix pins (Mitek [Johnson & Johnson], Mumbai, India); a transtibial technique was used for drilling of the femoral tunnel.11 In our method, we have used a transportal technique and the femoral fixation has been achieved by a RetroButton (Arthrex) instead of RigidFix pins. In 2013 Natali et al.12 described a technique for ACL reconstruction using distally inserted doubled hamstring tendons fixed at the femoral level using a second-generation cortical suspensory device.
In our technique the tibial-side fixation is based on preserved insertions only, thus eliminating the cost of a tibial-side fixation device; the average cost of a bio-interference screw in India is US $150. Furthermore, because it is believed that tibial-side fixation is the weakest link in the stiffness of a reconstructed ACL,8, 9 by relying on the natural insertions of the STG tendons on the tibia, we were also able to eliminate the weakest link in the overall construct of the reconstructed ACL.
Because we are not severing the insertions of the STG tendons from the tibia, the blood supply of the tendons remains intact. We believe that the preserved blood supply may have a role in early and superior healing of the graft and may have the potential to reduce the incidence of late rupture of the graft (Table 1). However, further studies are required to prove this.
Table 1.
Advantages
| Preserving the insertions of the hamstring tendons is more biological and may provide better proprioception and, hence, a better functional outcome in the postoperative period. |
| Because we are not severing the insertions of the STG tendons from the tibia, the blood supply of the tendons remains intact, which may facilitate superior healing of the graft and prevent graft rupture. |
| Tibial-side fixation of the free graft is the weakest link in the overall stiffness of the reconstructed ACL; our technique circumvents this problem. |
| The technique eliminates the need for a tibial-side fixation device, thus reducing the cost of surgery. |
| We propose that well-controlled, randomized comparative studies need to be performed to compare the results of ACL reconstruction using hamstring autograft with preserved insertions versus free hamstring autograft. |
ACL, anterior cruciate ligament; STG, semitendinosus and gracilis.
Our technique has certain limitations as well (Table 2). It is possible only with the use of an open-ended tendon harvester. If the harvested graft is short, then this procedure is not possible. Furthermore, the minimum length of graft required in the femoral tunnel is 15 mm.13 The minimum length of RetroButton loop available is 15 mm. Thus the femoral tunnel should be at least 30 mm long. If the femoral tunnel length is less than 30 mm, then the RetroButton cannot be used for femoral fixation of the graft.
Table 2.
Limitations and Pitfalls
| Our technique is only possible with the use of an open-ended tendon harvester. |
| If the harvested graft is short, then this procedure is not possible. |
| The minimum length of RetroButton loop available is 15 mm, and the minimum length of graft required in the femoral tunnel is 15 mm. Thus the femoral tunnel should be at least 30 mm long. If the femoral tunnel length is less than 30 mm, then the RetroButton cannot be used for femoral fixation of the graft. |
Ethibond has been readily used as a mode of fixation on the tibial side in association with a suture disk.14 Hence we believe that sewing the graft to itself using No. 5 Ethibond will provide sufficient strength to the graft. However, because we are using suspensory fixation at both the femoral and tibial ends, the theoretical risk of the windshield-wiper effect exists (Table 3).14 Comparing the mechanical stability and functional outcome of patients undergoing ACL reconstruction using hamstring tendon autograft with preserved insertions with those in patients undergoing ACL reconstruction using free hamstring autograft is a very interesting and promising subject and should be explored (Table 4, Table 5, Table 6).
Table 3.
Risks
| Ethibond has been used readily as a mode of fixation on the tibial side in association with a suture disk. Hence we believe that sewing the graft to itself using No. 5 Ethibond will provide sufficient strength to the graft. However, because we are using suspensory fixation at both the femoral and tibial ends, the theoretical risk of the windshield-wiper effect exists. |
Table 4.
Pearls
| Efforts must be taken to preserve the infrapatellar branch of the saphenous nerve while harvesting the graft. |
| While harvesting the graft, the surgeon must be careful not to prematurely amputate the graft. |
| The surgeon should keep the patient's knee in maximal hyperflexion during transportal drilling of the femoral tunnel to prevent a blowout fracture of the posterior wall of the lateral femoral condyle. |
Table 5.
Tips
| The harvested graft should be covered with moist gauze before starting preparation of the tunnels to prevent it from drying and desiccation. |
| The mathematical calculations must be correct while matching the length of the graft and loop of the RetroButton (Arthrex, Naples, FL) to the length of both the femoral and tibial tunnels plus the intra-articular part of the proposed graft. Any error in these calculations can result in the graft being lax or can cause problems in flipping the RetroButton. |
| The marking suture placed on the hamstring tendons should be just opposite the entry of the tibial tunnel so that when the graft is pulled inside the joint, the mark stays at the entry of the tunnel. |
Table 6.
Manufacturers of Equipment Used in Our Technique
| Open-ended tendon stripper: Arthrex, Naples, FL |
| Bone awl: Smith & Nephew, Mumbai, India |
| Cannulated drill bit: Smith & Nephew |
| Arthroscope: Stryker, Kalamazoo, MI |
| RetroButton: Arthrex |
| No. 5 Ethibond: Ethicon, Somerville, NJ |
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Anterior cruciate ligament reconstruction with preserved-insertion technique in left knee. The patient is lying supine on the operating table with the affected leg hanging from the edge of the table. An open-ended tendon stripper is used to harvest the hamstring tendons so that their tibial insertions are preserved. The proximal free ends of the tendons are sutured together using a No. 5 Ethibond suture. The tendons are then looped around a No. 5 Ethibond suture, thus creating a quadrupled graft, which is sized using a sizer. With the arthroscope in the anterolateral portal, the femoral tunnel is drilled in a transportal manner through the far-medial portal, with the knee kept in maximal hyperflexion, with a freehand technique, at the junction of the lateral condylar ridge and bifurcate ridge. The tibial tunnel is drilled in the standard manner. The length of the femoral tunnel (length A) and the length of the tibial tunnel plus the intra-articular part of the proposed graft (length B) are measured. A marking suture is placed on the hamstring tendons just opposite the entry of the tibial tunnel so that when the graft is pulled inside the joint, the mark stays at the entry of the tunnel. A RetroButton is loaded onto the quadrupled graft. The length of the quadrupled graft and loop of the RetroButton is adjusted so that it exactly corresponds to length A plus length B. The sutures of the RetroButton are pulled through the tibial and femoral tunnels by loading them onto the Ethibond loop placed inside the tunnels. The RetroButton is flipped outside the femoral tunnel onto the cortex. The free end of the graft exiting the tibial tunnel is pulled to maximal stretch and the joint moved through full range of motion at least 10 times to remove any kinks in the graft. The tightness of the anterior cruciate ligament graft is checked arthroscopically with a probe. With maximal stretch on the free end of the graft, it is sutured to the preserved end.
References
- 1.Gobbi A., Mahajan S., Zanazzo M., Tuy B. Patellar tendon versus quadrupled bone–semitendinosus anterior cruciate ligament reconstruction: A prospective clinical investigation in athletes. Arthroscopy. 2003;19:592–601. doi: 10.1016/s0749-8063(03)00393-1. [DOI] [PubMed] [Google Scholar]
- 2.Freeman J.W., Kwansa A.L. Recent advancements in ligament tissue engineering: The use of various techniques and materials for ACL repair. Recent Pat Biomed Eng. 2008;1:18–23. [Google Scholar]
- 3.Denti M., Monteleone M., Berardi A., Panni A.S. Anterior cruciate ligament mechanoreceptors. Histologic studies on lesions and reconstruction. Clin Orthop Relat Res. 1994:29–32. [PubMed] [Google Scholar]
- 4.Mou-wang Z., Li G., Ya-ping C. Factors affecting proprioceptive recovery after anterior cruciate ligament reconstruction. Chin Med J (Engl) 2008;121:2224–2228. [PubMed] [Google Scholar]
- 5.Barret D.S. Proprioception and function after anterior cruciate ligament reconstruction. J Bone Joint Surg Br. 1991;73:833–837. doi: 10.1302/0301-620X.73B5.1894677. [DOI] [PubMed] [Google Scholar]
- 6.Dvir Z., Korean E., Halperin N. Knee joint position sense after reconstruction of anterior cruciate ligament. J Orthop Sports Phys Ther. 1988;10:117–120. doi: 10.2519/jospt.1988.10.4.117. [DOI] [PubMed] [Google Scholar]
- 7.Harter R.A., Osternig L.R., Singer K.M. Long term evaluation of knee stability and function following surgical reconstruction for anterior cruciate ligament insufficiency. Am J Sports Med. 1988;16:434–443. doi: 10.1177/036354658801600502. [DOI] [PubMed] [Google Scholar]
- 8.Steiner M.E., Hecker A.T., Brown C.H., Jr. Anterior cruciate ligament graft fixation: Comparison of hamstring and patellar tendon grafts. Am J Sports Med. 1994;22:240–247. doi: 10.1177/036354659402200215. [DOI] [PubMed] [Google Scholar]
- 9.Sgaglione N.A., Warren R.F., Wickiewicz T.L. Primary repair with semitendinosus tendon augmentation of acute anterior cruciate ligament injuries. Am J Sports Med. 1990;18:64–73. doi: 10.1177/036354659001800111. [DOI] [PubMed] [Google Scholar]
- 10.Kim S.J., Kim H.K., Lee Y.T. Arthroscopic anterior cruciate ligament reconstruction using autogenous hamstring tendon graft without detachment of the tibial insertion. Arthroscopy. 1997;13:656–660. doi: 10.1016/s0749-8063(97)90198-5. [DOI] [PubMed] [Google Scholar]
- 11.Gupta R.K., Aggarwal S., Aggarwal V., Garg S., Kumar S. Preserved insertions of the semitendinosus and gracilis tendons (STG) in ACL reconstruction: A new surgical technique with preliminary results. Curr Orthop Pract. 2010;21:409–414. [Google Scholar]
- 12.Natali S., Buda R., Ruffilli A. Anatomic ACL reconstruction using distally inserted doubled hamstring tendons: Surgical technique and results. Orthopedics. 2013;5:147–151. doi: 10.3928/01477447-20130523-04. [DOI] [PubMed] [Google Scholar]
- 13.Zantop T., Diermann N., Schumacher T., Schanz S., Fu F.H., Peterson W. Anatomical and nonanatomical double-bundle anterior cruciate ligament reconstruction: Importance of femoral tunnel location on knee kinematics. Am J Sports Med. 2008;36:678–685. doi: 10.1177/0363546508314414. [DOI] [PubMed] [Google Scholar]
- 14.Chidanand K.J.C., Ballal M., Gupta S. Suspensory fixation of grafts in anterior cruciate ligament fixation using Endobutton and suture disc—A prospective study of 30 cases. Int J Sci Res Publ. 2015;5:1–3. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Anterior cruciate ligament reconstruction with preserved-insertion technique in left knee. The patient is lying supine on the operating table with the affected leg hanging from the edge of the table. An open-ended tendon stripper is used to harvest the hamstring tendons so that their tibial insertions are preserved. The proximal free ends of the tendons are sutured together using a No. 5 Ethibond suture. The tendons are then looped around a No. 5 Ethibond suture, thus creating a quadrupled graft, which is sized using a sizer. With the arthroscope in the anterolateral portal, the femoral tunnel is drilled in a transportal manner through the far-medial portal, with the knee kept in maximal hyperflexion, with a freehand technique, at the junction of the lateral condylar ridge and bifurcate ridge. The tibial tunnel is drilled in the standard manner. The length of the femoral tunnel (length A) and the length of the tibial tunnel plus the intra-articular part of the proposed graft (length B) are measured. A marking suture is placed on the hamstring tendons just opposite the entry of the tibial tunnel so that when the graft is pulled inside the joint, the mark stays at the entry of the tunnel. A RetroButton is loaded onto the quadrupled graft. The length of the quadrupled graft and loop of the RetroButton is adjusted so that it exactly corresponds to length A plus length B. The sutures of the RetroButton are pulled through the tibial and femoral tunnels by loading them onto the Ethibond loop placed inside the tunnels. The RetroButton is flipped outside the femoral tunnel onto the cortex. The free end of the graft exiting the tibial tunnel is pulled to maximal stretch and the joint moved through full range of motion at least 10 times to remove any kinks in the graft. The tightness of the anterior cruciate ligament graft is checked arthroscopically with a probe. With maximal stretch on the free end of the graft, it is sutured to the preserved end.