

Abstract
Background
POEMS syndrome is a rare paraneoplastic syndrome due to an underlying plasma cell neoplasm. Hypogonadism is the most common endocrine abnormality in POEMS syndrome. There is no data about improvement of hypogonadism and sexual dysfunction after appropriate treatment of POEMS syndrome so far. In this single-center prospective study, the efficacy of low-dose lenalidomide and dexamethasone combination therapy in the improvement of sexual and gonadal function in POEMS syndrome was evaluated.
Results
Thirty-five patients with newly diagnosed POEMS syndrome were treated with Lenalidomide (10 mg daily for 21 days) and dexamethasone (40 mg once per week) for 12 cycles. The international index of erectile function (IIEF) in male patients, the female sexual function index (FSFI) in female patients, total testosterone, estradiol and vascular endothelial growth factor (VEGF) levels were reviewed. Sexual dysfunction was reported in 88.8 % (24/27)male and 90.9 % (10/11) female patients. 62.9 % (17/27) male and 25.0 % (3/12) female patients had hypogonadism. After 12-month treatment, the mean total FSFI score had increased from 17.1 ± 7.2 to 23.7 ± 7.2(p < 0.05). The arousal, orgasm and sex pain domains had been improved significantly. The mean IIEF scores had increased from 12.9 ± 13.0 to 20.5 ± 18.4 (p < 0.05). Erectile function, sexual desire and intercourse satisfaction had improved significantly at the end of treatment. No association between VEGF levels and sexual function improvement was found in both genders.
Conclusion
Combination therapy with low-dose lenalidomide plus dexamethasone is successful in improving sexual function in POEMS syndrome.
Keywords: POEMS syndrome, Lenalidomide, Sexual function, Hypogonadism
Background
POEMS (polyneuropathy, organomegaly, endocrinopathy, M-spike, skin changes) syndrome is a rare paraneoplastic syndrome characterized with multisystem involvement and markedly increased vascular endothelial growth factor (VEGF) levels [1]. VEGF is a growth factor for endothelial cells that induces vascular permeability, which is important in angiogenesis and often decreases with successful treatment [2].
Endocrinopathy is a central but poorly understood feature of POEMS. In Mayo Clinic series, about 84 % of patients had a recognized endocrinopathy, with hypogonadism as the most common endocrine abnormality, followed by thyroid dysfunction, abnormal glucose metabolism, and lastly by adrenal insufficiency [3]. In their report, 79 % male patients had subnormal total testosterone levels and 61 % reported erectile dysfunction. Gonadal dysfunction is a serious problem that reduces patients’ quality of life and interpersonal relationships. Most of the information regarding hypogonadism in POEMS syndrome is from isolated case reports or small series that have not systematically studied. Little is known about improvement of hypogonadism after appropriate treatment of POEMS syndrome.
Lenalidomide is a derivative of thalidomide, with powerful activity against malignant plasma cells as well as acting to decrease the levels of proinflammatory and proangiogenic cytokines. Recently, it has been showed that lenalidomide might play a promising role in the treatment of POEMS syndrome [4, 5]. In our previous work, the efficacy and safety of low dose lenalidomide plus dexamethasone had been demonstrated in patients with relapsed or refractory POEMS syndrome [2]. Here we conducted a pilot study to assess the efficacy of lenalidomide plus dexamethasone in the improvement of gonadal and sexual function of POMES syndrome in our center.
Methods
Patients
Forty-one consecutive patients with newly diagnosed POEMS syndrome (male 28, female 13) were treated with combination of low-dose lenalidomide and dexamethasone at Peking Union Medical College Hospital from April 2014 to November 2015. All patients met the diagnostic criteria defined by Dispenzieri, with two mandatory criteria (polyneuropathy and monoclonoal plasma cell proliferating disorder), at least one major criterion (sclerotic bone lesion, Castleman disease or VEGF elevation) and one minor criterion (organomegaly, edema, endocrinology, skin change, papillary edema or thrombocytosis) [6]. Excluded from the study were patients with a history of medication use, such as antidepressants, psychotropic drugs, beta-blockers and spirolactone, which can interfere with sexual function. No hormone replacement therapy was employed in patients with hypogonadism.
Regimen and doses
All patients received lenalidomie (Revlimid; Celgene Corporation, Summit, NJ, USA) at a dose of 10 mg daily for 21 days of a 28-day cycle, plus oral dexamethasone at 40 mg once per week. Aspirin at a dose of 100 mg daily was prescribed for thromboprophylaxis.
Study objectives
Assessment of sexual function
International Index of Erectile Function (IIEF) questionnaire and Female Sexual Function Index (FSFI) questionnaire were administered in male and female patients respectively at every visit. IIEF is sensitive and specific for detecting treatment-related changes in patients with erectile dysfunction [7]. In this 15-item self-reporting questionnaire, five separate domains of sexual function are measured, including erectile function, orgasmic function, sexual desire, intercourse satisfaction and overall satisfaction. FSFI is a 19-item multidimensional self-reporting measure, which quantifies six domains of female sexual dysfunction, including desire, arousal, lubrication, orgasm, satisfaction and pain. It has become the de facto “gold standard” in the assessment of female sexual function and an indispensable tool in clinical research of female sex dysfunction [8]. The reliability and validity of Chinese version of FSFI had been demonstrated in Chinese women [9].
Laboratory procedures
All blood samples were collected between 7 and 11 AM. Total testosterone in male and estradiol in female patients were measured with Access testosterone reagent and Access Estradiol reagent (Beckman Instrument, Inc. Chaska, MN, USA) in the central laboratory of Peking Union Medical College Hospital. Serum VEGF levels were measured with human Quantikine ELISA Kit (R&D Systems, Minneaplis, MN, USA). Normal serum VEGF was less than 600 pg/ml, which was determined in our previous work [10].
Statistical analysis
Data analysis was performed with the statistical software package SPSS 22.0 (SPSS, Inc., Chicago, IL, USA). t-test was used to detect the statistical significance of the Hormone levels, VEGF levels, FSFI and IIEF scores before and after lenalidomide treatment. Spearman correlation test was performed to determine the association between IIEF/FSFI scores and hormone levels or serum VEGF. A value of P < 0.05 was considered statistically different.
Results
Baseline characteristics of participants
A total of 41 patients were enrolled in this study (male 28, female 13). The median age at diagnosis was 49 years (range, 21–70). One female patient and one male patient were ruled out because of sexually inactivity. Two female patients died during follow up and two male patients retreated. All other 35 patients finished the 12-months study. All the participants were married. Before treatment, the mean total FSFI score was 17.1 ± 7.2, much lower than that of normal Chinese female (27.3 ± 2.79) [9]. 90.9 % (10/11) female patients had FSFI score lower than 26.55, the cut-off value for a diagnosis of FSD [8]. 25.0 % (3/12) female patients had estradiol levels below the lower limit of normal range, including one patient with primary hypogonadism and two patients with secondary hypogonadism. Based on the score of IIEF, 88.8 %(24/27)male patients reported erectile dysfunction, including 66.7 %(18/27) with severe ED, 18.5 % (5/27) with moderate ED, 3.7 % (1/27) with mild to moderate ED. 62.9 % (17/27) male patients had total testosterone levels below the lower limit of normal range, including 6 patients with primary hypogonadism and 11 patients with secondary hypogonadism. The median VEGF level was 5155 pg/ml (range, 534–14328) before treatment. 94.7 % (38/39) had elevated VEGF than the cut-off value (600 pg/ml).
Improvement of female sexual function after 12-months treatment
The mean total FSFI score had been improved to 23.7 ± 7.2 after 12-month treatment. On the basis of the total FSFI score, FSD was diagnosed in 10 of 11 patients (90.9 %) at baseline and 7 of 10 patients (70.0 %) after treatment. The arousal, orgasm and sex pain domains had been improved significantly at the end of 12-month treatment (Fig. 1 and Table 1). Changes in mean scores from baseline to the end of the study for individual questions assessing desire, lubrication and sex satisfaction were not statistically different.
Fig. 1.
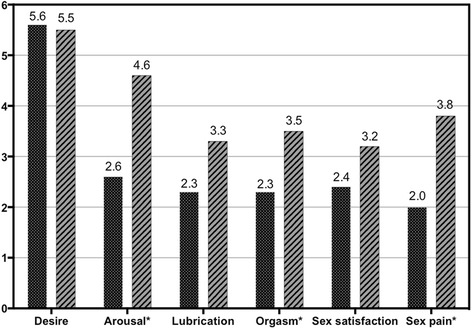
Mean FSFI distribution by domain before and after 12-month combination therapy. FSFI: Female Sexual Function Index. * p < 0.05
Table 1.
Changes in FSFI scores and laboratory parameters after 12-month combination therapy in Female patients
| Baseline (N = 12) | End of study (N = 10) | 95 % confidence interval of the diff (N = 10) | P value | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| FSFI Domains Desire | 5.6 ± 0.9 | 5.5 ± 1.0 | −0.9 | 0.6 | 0.468 |
| Arousal | 2.6 ± 1.9 | 4.6 ± 1.8 | 0.6 | 4.0 | 0.002* |
| Lubrication | 2.3 ± 1.9 | 3.3 ± 2.0 | −0.8 | 3.3 | 0.084 |
| Orgasm | 2.3 ± 1.9 | 3.5 ± 2.1 | −0.6 | 3.4 | 0.050* |
| Satisfaction | 2.4 ± 1.2 | 3.2 ± 2.0 | −0.6 | 2.1 | 0.112 |
| Pain | 2.0 ± 1.6 | 3.8 ± 2.4 | −0.7 | 4.8 | 0.046* |
| Total FSFI score | 17.1 ± 7.2 | 23.7 ± 7.2 | 1.5 | 13.6 | 0.003* |
| FSH (IU/L) | 12.38 ± 13.47 | 33.20 ± 28.75 | 4.45 | 61.95 | 0.067 |
| LH (IU/L) | 8.05 ± 9.09 | 17.26 ± 18.81 | −1.55 | 36.07 | 0.017* |
| E2 (pg/mL) | 81.92 ± 62.62 | 59.50 ± 92.79 | −93.99 | 113.69 | 0.771 |
| VEGF (pg/mL) | 6190.5 ± 3979.3 | 1468.2 ± 1495.4 | 908.7 | 8871.7 | 0.004* |
SD standard deviation
Association between female sexual function, estradiol and VEGF levels
In female patients, levels of estradiol were 81.92 ± 62.62 pg/ml at baseline and 59.50 ± 92.79 pg/ml at the end of study (p = 0.771). There was no significant improvement of estradiol levels. The mean VEGF levels decreased from 6190.5 ± 3979.3 pg/ml at baseline to 1468.2 ± 1495.4 pg/ml at the end of treatment (p = 0.004). No association between VEGF levels and estradiol levels was found (p = 0.580, Spearman test). Nor did the association between VEGF levels and FSFI scores (p = 0.841, Spearman test).
Improvement of male sexual function after 12-months treatment
After 12-month treatment, the mean IIEF scores have increased from 12.9 ± 13.0 to 20.5 ± 18.4 (p < 0.05). Patients with severe ED have decreased from 66.7 % (18/27) to 40.0 % (10/25). Ratio of patients with normal erectile function have increased from 11.1 % (3/27) to 36.0 (9/25) (Table 2). Erectile function, sexual desire and intercourse satisfaction had improved significantly at the end of treatment (Fig. 2, Table 3). Changes in mean scores from baseline to the end of the study for individual questions assessing orgasmic function and overall satisfaction were not statistically different.
Table 2.
Severity of erectile dysfunction at baseline and at the end of study
| Baseline (N = 27) | End of study (n = 25) | |
|---|---|---|
| Severity of ED (EFD score),n% | ||
| Severe (<11) | 18(66.7) | 10(40.0) |
| Moderate (11 ~ 16) | 5(18.5) | 5(20.0) |
| Mild to moderate (17 ~ 21) | 1(3.7) | 1(4.0) |
| Mild (22 ~ 25) | 0(0.0) | 0(0.0) |
| Normal (>25) | 3(11.1) | 9(36.0) |
Fig. 2.
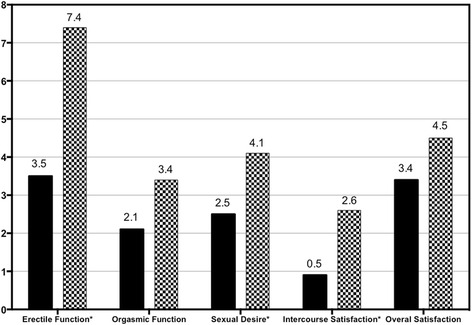
Mean IIEF distribution by domain before and after 12-month combination therapy * p < 0.05
Table 3.
Changes in IIEF scores and laboratory parameters after 12-month combination therapy in male patients
| Baseline (N = 27) | End of study (N = 25) | 95 % confidence interval of the diff (N = 25) | P value | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| IIEF Domains | |||||
| Erectile Function | 3.6 ± 5.4 | 7.3 ± 8.9 | −3.3 | 10.6 | 0.012* |
| Orgasmic Function | 2.2 ± 2.5 | 3.0 ± 3.2 | −1.7 | 3.4 | 0.106 |
| Sexual Desire | 2.6 ± 1.4 | 3.8 ± 2.6 | −1.1 | 3.6 | 0.012* |
| Intercourse Satisfaction | 0.9 ± 2.8 | 2.2 ± 3.6 | −0.4 | 3.9 | 0.022* |
| Overall Satisfaction | 3.6 ± 2.1 | 4.2 ± 2.6 | −2.1 | 3.4 | 0.228 |
| Total IIEF Score | 12.9 ± 13.0 | 20.5 ± 18.4 | −6.1 | 21.4 | 0.009* |
| FSH (IU/L) | 10.77 ± 12.51 | 19.32 ± 12.50 | 6.82 | 31.82 | 0.411 |
| LH (IU/L) | 8.32 ± 5.07 | 10.15 ± 9.45 | 0.70 | 19.60 | <0.001* |
| Total T (nmol/L) | 5.38 ± 3.23 | 11.30 ± 5.67 | −1.54 | 2.78 | <0.001* |
| VEGF (pg/mL) | 5965.0 ± 2860.3 | 1355.6 ± 1563.4 | 1422.4 | 7862.0 | <0.001* |
Association between male sexual function, total testosterone and VEGF levels
In male patients, levels of total testosterone were 5.38 ± 3.23 nmol/L at baseline and had been improved to 11.30 ± 5.67 nmol/L at the end of study (p < 0.001). The mean VEGF levels decreased from 5965.0 ± 2860.3 pg/ml at baseline to 1355.6 ± 1563.4 pg/ml at the end of treatment. No association between total testosterone levels and IIEF scores was found. There was no association between VEGF levels and IIEF scores or testosterone levels, neither.
Discussion
The present study explored the under-investigated area of sexual quality of life in patients with POEMS syndrome. Our results demonstrated that low-dose lenalidomide plus dexamethasone combination therapy is successful in improving sexual function in patients with POEMS syndrome.
Hypogonadism is the most common endocrine disorders in POEMS syndrome. Because of the low incidence, there were only case reports about hypogonadism in POEMS so far [11, 12]. In the Mayo series, 79 % (26/38) male patients had hypogonadism and 61 % (23/39) reported erectile dysfunction [3]. In our reported series, hypogonadism was seen in 52.2 % (26/46) male patients. Impotence (89 %) and gynecomastia (12 %) were common findings in male patients [13]. Sasano et al. reported the first case that showed an improvement in gonadotropin secretion after corticosteroid therapy [14]. After three months of corticosteroids treatment, the 49-year-old male patient showed an improvement in danadotropin secretion but no considerable change in the secretion of the other hormones. Recently, Chu et al. reported their experience of a patient with POEMS syndrome with long-term therapy with lenalidomide. The total testosterone levels had increased from 55 ng/dl to 624 ng/dl after one year [15].
There are no clinical trials assessing improvement of hypogonadism or sexual function after appropriate treatment of POEMS syndrome. Our study is the first report about improvement of sexual function in POEMS syndrome. Sexual dysfunction had been reported in 90.9 % female patients and 88.8 % male patients at baseline. In male patients, the mean IIEF scores have increased from 12.9 ± 13.0 to 20.5 ± 18.4 at the end of study. Patients with severe ED have decreased from 65.4 % to 42.3 %. Ratio of patients with normal erectile function had increased from 11.5 % to 34.6 %. Erectile function, sexual desire and intercourse satisfaction had improved significantly at the end of treatment. In female patients, the mean total FSFI score had been improved to 23.7 ± 7.2 after 12-month treatment. In female patients, FSD was diagnosed in 90.9 % at baseline and decreased to 70.0 % at the end of study. The arousal, orgasm and sex pain domains had been improved significantly at the end of 12-month treatment.
Sexual function is affected by multiple factors such as anatomical, physiological, psychological and social factors, and in consequence, it can lead to decreased quality of life. Autonomic nerve function plays an important role in sexual function. It was reported that autonomic fibers might be preserved despite major involvement of the large motor fibers in POEMS patients [16]. Hypogonadism is another important factor contributing to sexual dysfunction. In our study, hypogonadism was found in 25.0 % female patients and 62.9 % male patients. At the end of study, there was no significant improvement of estradiol levels in female patients but a significant increase of total testosterone levels was found in male patients. Surprisingly, no association between total testosterone levels and IIEF scores was found.
The pathogenesis of endocrinopathy is not well understood. Circulating antibodies against hormones or specific hormone receptors have not been found. No specific structural changes had been found in endocrine glands [17]. VEGF is a growth factor for endothelial cells that induces an increase in vascular permeability, is important in angiogenesis, and often decreases with successful therapy. There were accumulating evidences suggesting that the high level of VEGF contributed to some specific features of POEMS syndrome, such as extravascular volume overload, organomegaly, hemangioma, and peripapillary retinal thickness [18, 19]. In this study, after 12-month treatment, the mean VEGF levels decreased significantly in both gender. But no association between VEGF levels and IIEF score or FSFI score changes had been demonstrated. There are several other options for treatment of POEMS syndrome, including melphalan, thalidomide and transplantation. All these regimens are effective in decreasing VEGF levels. Whether the effects on sexual and gonadal function are specific to lenalidomide/dexamethasone or not is another interesting issue to investigate.
The present study had several limitations. The main limitation of this study is the number of participants. Taking into account the fact that POEMS syndrome is a rare disorder, small populations do not guarantee a very strong insight. A larger number of patients will provide more information between sexual function and gonadal hormone level changes especially in female patients. We also did not collect data regarding educational status or social economic status.
Conclusion
In summary, low-dose lenalidomide plus dexamethasone combination therapy is successful in improving gonadal function in patients with POEMS syndrome.
Abbreviations
FSFI, female sexual function index FSFI is a 19-item multidimensional self-reporting measure, which quantifies six domains of female sexual dysfunction, including desire, arousal, lubrication, orgasm, satisfaction and pain. It has become the de facto “gold standard” in the assessment of female sexual function and an indispensable tool in clinical research of female sex dysfunction; IIEF, international index of erectile function IIEF is a 15-item self-reporting questionnaire, in which five separate domains of sexual function are measured, including erectile function, orgasmic function, sexual desire, intercourse satisfaction and overall satisfaction. IIEF is sensitive and specific for detecting treatment-related changes in patients with erectile dysfunction; POEMS syndrome, POEMS (polyneuropathy, organomegaly, endocrinopathy, M-spike, skin changes) syndrome is a rare paraneoplastic syndrome characterized with multisystem involvement; VEGF, vascular endothelial growth factor VEGF is a growth factor for endothelial cells that induces vascular permeability
Acknowledgements
The authors offer their sincere thanks to all the participants and their families who participated in the clinical trial.
Funding
This work had been supported by the National Natural Science Foundation of China (no. 81570195), the Beijing Natural Science Foundation (no. 7142130) and the Specialized Research Fund for the Doctoral Program of Higher Education (no. 2013110611000).
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article.
Authors’ contributions
YHB participated in the design of the protocol of endocrine and sexual function assessment and drafted the manuscript. HXF carried out the statistical analysis of data. CQQ participated in data collecting. CXX and ZDB participated in clinical trial. LJ conceived the study and performed in clinical trial. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethnics approval and consent to participate
This single-center study was approved by the Institutional Review Boards of Peking Union Medical College Hospital and carried out in accordance with good clinical practices and ethical principles of the Declaration of Helsinki. All participants provided written informed consent prior to their participation.
Footnotes
Hongbo Yang and Xufei Huang are co-first authors.
Contributor Information
Hongbo Yang, Email: yanghb@pumch.cn.
Xufei Huang, Email: hxf443626812@163.com.
Qianqian Cai, Email: convenience_love@126.com.
Chen Wang, Email: chenw_07@126.com.
Xinxin Cao, Email: caoxinxin@126.com.
Daobin Zhou, Email: zhoudaobin@yahoo.com.
Jian Li, Email: lijian@pumch.cn.
References
- 1.Dispenzieri A. POEMS syndrome: update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90:951–62. doi: 10.1002/ajh.24171. [DOI] [PubMed] [Google Scholar]
- 2.Cai QQ, Wang C, Cao XX, Cai H, Zhou DB, Li J. Efficacy and safety of low-dose lenalidomide plus dexamethasone in patients with relapsed or refractory POEMS syndrome. Eur J Haematol. 2015;95:325–30. doi: 10.1111/ejh.12492. [DOI] [PubMed] [Google Scholar]
- 3.Gandhi GY, Basu R, Dispenzieri A, Basu A, Montori VM, Brennan MD. Endocrinopathy in POEMS syndrome: the Mayo Clinic experience. Mayo Clin Proc. 2007;82:836–42. doi: 10.4065/82.7.836. [DOI] [PubMed] [Google Scholar]
- 4.Dispenzieri A, Klein CJ, Mauermann ML. Lenalidomide therapy in a patient with POEMS syndrome. Blood. 2007;110:1075–6. doi: 10.1182/blood-2007-03-082354. [DOI] [PubMed] [Google Scholar]
- 5.Royer B1, Merlusca L, Abraham J, Musset L, Haroche J, Choquet S, et al. Efficacy of lenalidomide in POEMS syndrome: a retrospective study of 20 patients. Am J Hematol. 2013;88:207–12. doi: 10.1002/ajh.23374. [DOI] [PubMed] [Google Scholar]
- 6.Dispenzieri A. POEMS syndrome. Blood Rev. 2007;21:285–99. doi: 10.1016/j.blre.2007.07.004. [DOI] [PubMed] [Google Scholar]
- 7.Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49:822–30. doi: 10.1016/S0090-4295(97)00238-0. [DOI] [PubMed] [Google Scholar]
- 8.Sand M, Rosen R, Meston CM, Brotto LA. The Female Sexual Function Index (FSFI): A potential “gold standard” measure for assessing therapeutically-induced change in female sexual function. Fertil Steril. 2009;29:S-129. doi: 10.1016/j.fertnstert.2009.07.1173. [DOI] [Google Scholar]
- 9.Sun XG, Li CY, Jin LN, Fan YJ, Wang DM. Development and validation of Chinese version of female sexual function index in a Chinese population- a pilot study. J Sex Med. 2011;8:1101–11. doi: 10.1111/j.1743-6109.2010.02171.x. [DOI] [PubMed] [Google Scholar]
- 10.Li J, Zhang W, Jiao L, Duan MH, Guan HZ, Zhu WG, et al. Combination of melphalan and dexamethasone for patients with newly diagnosed POEMS syndrome. Blood. 2011;117:6445–49. doi: 10.1182/blood-2010-12-328112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Del Río Prado AF, Reza Albarrán AA1, Gómez Pérez FJ. Male aged 31 years with polyneuropathy, prostration, and hypogonadism. Gac Med Mex. 2015;151:256–9. [PubMed] [Google Scholar]
- 12.Sevketoglu E, Hatipoglu S, Ayan I, Dogan O, Salihoglu B. Case report: POEMS syndrome in childhood. J Pediatr Hematol Oncol. 2008;30:235–8. doi: 10.1097/MPH.0b013e31815f88da. [DOI] [PubMed] [Google Scholar]
- 13.Li J, Zhou DB, Huang Z, Jiao L, Duan MH, Zhang W, et al. Clinical characteristics and long-term outcome of patients with POEMS syndrome in China. Ann Hematol. 2011;90:819–26. doi: 10.1007/s00277-010-1149-0. [DOI] [PubMed] [Google Scholar]
- 14.Sasano T, Sakurai SI, Hara Y. Improvement in gonadotropin secretion after corticosteroid therapy in a case of POEMS syndrome. Endocr J. 1998;54:413–9. doi: 10.1507/endocrj.45.413. [DOI] [PubMed] [Google Scholar]
- 15.Chu BF, Shana'ah A, Hofmeister CC, Benson DM, Sell M, Tucker J, et al. Long-Term Therapy with Lenalidomide in a Patient with POEMS Syndrome. Eur J Case Rep Intern Med. 2014;1:1-7. [DOI] [PMC free article] [PubMed]
- 16.Fujinuma Y, Asahina M, Fukushima T, Katagiri A, Yamanaka Y, Misawa S, et al. Preserved autonomic function in patients with POEMS syndrome. J Neurol Sci. 2012;318:131–34. doi: 10.1016/j.jns.2012.03.004. [DOI] [PubMed] [Google Scholar]
- 17.Gherardi R, Baudrimont M, Kujas M, Malapert D, Lange F, Gray F, et al. Pathological findings in three non-Japanese patients with the POEMS syndrome. Virchows Arch A Pathol Anat Histopathol. 1988;413:357–65. doi: 10.1007/BF00783029. [DOI] [PubMed] [Google Scholar]
- 18.Watanabe O, Arimura K, Kitajima I, Osame M, Maruyama I. Greatly raised vascular endothelial growth factor (VEGF) in POEMS syndrome. Lancet. 1996;347:702. doi: 10.1016/S0140-6736(96)91261-1. [DOI] [PubMed] [Google Scholar]
- 19.Yokouchi H, Baba T, Misawa S, Sawai S, Kitahashi M, Oshitari T, et al. Correlation between peripapillary retinal thickness and serum level of vascular endothelial growth factor in patients with POEMS syndrome. Br J Ophthalmol. 2015 Oct 26. doi: 10.1136/bjophthalmol-2015-307068. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The dataset supporting the conclusions of this article is included within the article.