

Abstract
Colonic diverticular disease is the most common cause of lower gastrointestinal bleeding. In the past, this condition was usually managed with urgent colectomy. Recently, the development of endoscopy and interventional radiology has led to a change in the management of colonic diverticular bleeding.
The aim of this systematic review is to define the best treatment for colonic diverticular bleeding.
A systematic bibliographic research was performed on the online databases for studies (randomized controlled trials [RCTs], observational trials, case series, and case reports) published between 2005 and 2014, concerning patients admitted with a diagnosis of diverticular bleeding according to the PRISMA methodology.
The outcomes of interest were: diagnosis of diverticulosis as source of bleeding; incidence of self-limiting diverticular bleeding; management of non self-limiting bleeding (endoscopy, angiography, surgery); and recurrent diverticular bleeding.
Fourteen studies were retrieved for analysis. No RCTs were found. Eleven non-randomized clinical controlled trials (NRCCTs) were included in this systematic review. In all studies, the definitive diagnosis of diverticular bleeding was always made by urgent colonoscopy. The colonic diverticular bleeding stopped spontaneously in over 80% of the patients, but a re-bleeding was not rare. Recently, interventional endoscopy and angiography became the first-line approach, thus relegating emergency colectomy to patients presenting with hemodynamic instability or as a second-line treatment after failure or complications of hemostasis with less invasive treatments.
Colonoscopy is effective to diagnose diverticular bleeding. Nowadays, interventional endoscopy and angiographic treatment have gained a leading role and colectomy should only be entertained in case of failure of the former.
BACKGROUND
Lower gastrointestinal bleeding (LGIB) has an annual incidence of 36 per 100,000 in the United States, approximately 5 times less than upper gastrointestinal (GI) bleeding1 and it is usually caused by diverticular disease.2,3 Diverticular bleeding resolves spontaneously with conservative management in the majority of patients, but often recurs. Moreover, persistent bleeding or acute and massive bleeding presenting with hemodynamic disorders requires an interventional treatment.4 Recently, the development of new technologies such as interventional endoscopy, angiography, and laparoscopic surgery has led to a change in the management of patients with colonic diverticular bleeding.5–7 Colectomy is still necessary in extreme settings and when less invasive procedures are unsuccessful or unavailable. Although this topic has been the subject of several studies in the recent past, the question of what is the best treatment for acute diverticular bleeding still remains unanswered. Therefore, we performed a systematic review of the literature on the current management of bleeding from colon diverticular disease.
METHODS
We followed the methodology suggested by PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.8 A systematic bibliographic research was performed on the following online databases: PubMed, EMBASE, Cochrane Register of Controlled Clinical Trials, Scopus, and Publish or Perish. The research was conducted since January 2005 through August 2014.
These following search strategies were used in PubMed:
Diverticular [All Fields] AND (“hemorrhage” [All Fields] OR “hemorrhage” [MeSH Terms] OR “hemorrhage” [All Fields]).
“management” [All Fields] OR “disease management” [MeSH Terms] OR (“disease” [All Fields] AND “management” [All Fields]) OR “disease management” [All Fields] AND diverticular [All Fields] AND (“hemorrhage” [All Fields] OR “hemorrhage” [MeSH Terms] OR “hemorrhage” [All Fields]).
Studies Selection
Inclusion criteria for the present systematic review included: published randomized controlled trials (irrespective of sample size, follow-up, or methodological quality), observational trials, case series, and case reports published between January 2005 and August 2014, concerning patients admitted with a diagnosis of colonic bleeding. We excluded the studies that did not report specific data on the cause of the LGIB. Two authors performed the online bibliographic research (CR and RC) and screened the papers by their title and their abstract to identify those needing further full text assessment to establish their possible relevance according to the inclusion and exclusion criteria. In case of overlapping patient populations, the most recent study or the study with the better methodological quality was considered.
Data Extraction
CR and RC assessed the included studies for their methodological quality using the revised and modified grading system of the Scottish Intercollegiate Guidelines Network (SIGN).9 The same 2 authors (CR and RC) independently retrieved the data of interest. The outcomes of interest were: rate of diverticular disease as source of GI bleeding; incidence of self-limiting diverticular bleeding; management of persistent (non self-limiting) bleeding (endoscopy, angiography, surgery); and recurrent diverticular bleeding.
Ethics Approval
This study is a systematic review. Ethics approval or institutional review board approval was not necessary, as the study did not involve patient consent.
RESULTS
The PRISMA flow diagram for systematic review is shown in Figure 1. The initial search produced 643 potentially relevant papers. After screening for titles and abstracts, 14 papers were further assessed for eligibility; 3 were excluded because outcome data were not available. No RCTs were found. Eleven non-randomized controlled trials (NRCTs), with 701 patients were included in this systematic review (Table 1).10–20 The mean modified SIGN grading score of the included articles was 7.3 points (Table 2).
FIGURE 1.
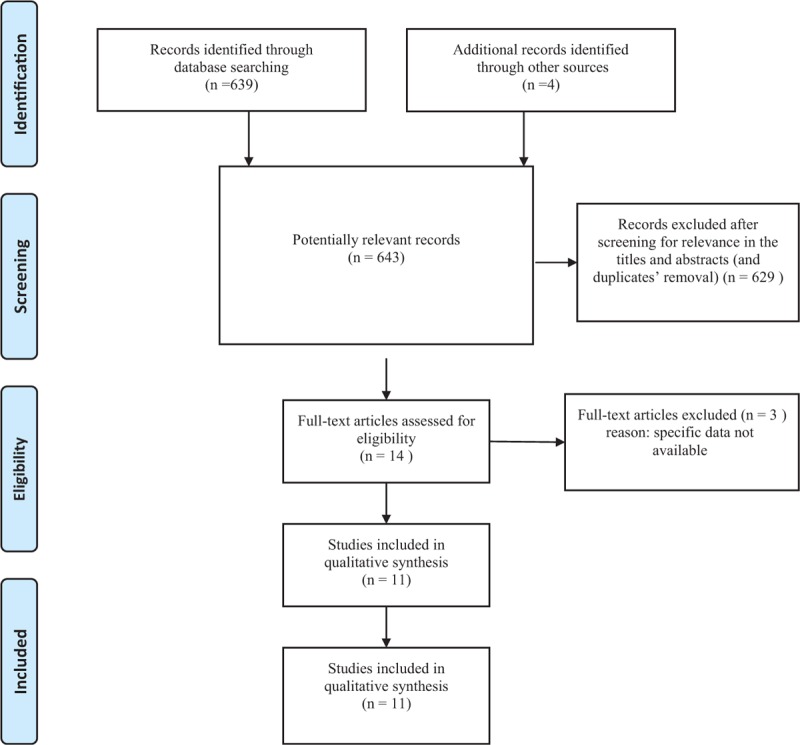
PRISMA flow chart of literature search.
TABLE 1.
Characteristics of Nonrandomized Controlled Trials (NRCTs) Included in This Systematic Review

TABLE 2.
Evaluation of Methodological Qualities of the Included Studies

Weaknesses of the Included Studies
Some of the announced outcomes were often not available. None of the studies noted any information about the colonoscopy sedation and not all study reported if bowel preparation before colonscopy was done (Table 3); only 1 article (Heianna et al10) reported that during transcatheter arterial embolization (TAE) no patient received any sedation. Data on TAE and surgical approach (laparotomy vs. laparoscopy) were not well defined; those concerning the extent and location of colonic diverticula, endoscopic treatment, and/or arteriography with immediate superselective embolization, surgical treatment, and/or diagnostic-therapeutic timing were variable between the included studies and not homogeneous. Most of the studies did not report follow-up data12,14–16,18,20 (Table 1).
TABLE 3.
Diagnosis of Diverticular Bleeding Was Always Performed by Urgent Colonoscopy

Effects of Interventions
In all studies, diverticular bleeding was always diagnosed by colonoscopy (Table 3); only 4 of them were based on the criteria described by Jensen, Prakash, and Zuckerman,13,15,17,20 which consist in evident endoscopic stigmata such active bleeding, visible vessel, and adherent clot, and presumptive findings such as presence of fresh blood within 1 or more colonic segments and diverticular erosions. Our literature revision confirmed that in most of cases spontaneous hemostasis avoided interventional treatment. In fact, the identified reports showed how only 16% (7.6% to 100%) of patients with colonic bleeding needed an interventional treatment. Endoscopic treatment represents the most performed initial approach for unremissive bleeding, accounting for 66% of all treated patients. TAE was performed in about 10.5% (3.3% to 100%) of all the bleedings. Collecting data from the revised works, we estimated a failure rate of all conservative treatments combined of 2.6% (3/114 patients underwent conservative treatment). Emergency surgical approach was necessary in 28 of 114 cases. This means that almost 25% (2.2% to 30.4%) of patients admitted with a diagnosis of diverticular bleeding could undergo surgery (Table 4).
TABLE 4.
Treatment of Diverticular Bleeding

DISCUSSION
Patients with diverticular disease may develop diverticular bleeding in 3% to 15% of cases21,22; however, this condition usually stops spontaneously up to 90% of times.23,24 The mechanisms for colonic diverticular bleeding is not completely understood. Probably the bleeding is caused by perforation of small arteries, damaged in their endothelial layer. The first injury produces an eccentric damage to the lumen of the artery that reacts with eccentric intimal thickening.25 If damage persists or recurs, the first thickening becomes concentric, the arterial wall weakens and leads to eccentric rupture and bleeding. Atherosclerosis has been considered to be the main cause of diverticular bleeding. Nonsteroidal anti-inflammatory drugs, cerebrovascular disease, and hyperuricemia are significant predictors of diverticular bleeding. The most significant risk factor is the current usage of nonsteroidal anti-inflammatory drugs, because they inhibit prostaglandin synthesis and platelet aggregation, causing bleeding if diverticular disease is present.26 Hyperuricemia favors diverticular bleeding. Elevated uric acids induce the oxygenation of low-density lipoprotein cholesterol and promote lipid peroxidation, causing elevated production of oxygen-free radicals. These events show progression of atherosclerosis.27 Atherosclerosis and related diseases favor diverticular bleeding28 and a prospective study must be planned to demonstrate that atherosclerosis may cause diverticular bleeding. Contrast-enhanced computed tomography (CT) is useful to detect colonic diverticular bleeding.29 Extravasation of contrast medium was observed in 30% of patients and in 68% of the patients with diverticular bleeding, bleeding diverticula were identified and treated with colonoscopy. In patients with diverticular bleeding, contrast-enhanced CT is mandatory before colonoscopy, because identifying the source of bleeding prior to surgery may result in a less invasive urgent colonoscopy and more effective hemostasis.29 Diagnosis of bleeding diverticulosis has evolved during the last decade with the constant use of CT helical angiography and selective mesenteric angiography performed in those patients in whom colonoscopy is not feasible, contraindicated or incomplete.30 The management of bleeding colonic diverticula is very heterogeneous in the analyzed literature and it has evolved in the last 10 years with the introduction of interventional endoscopy (epinephrine injection, multipolar or heat probe coagulation, placement of endoclips and band ligation) and angiographic treatment through the use of intra-arterial infusion of vasopressin (TAE) (Figure 2). Approximately 10% to 25% of patients require urgent surgery for hemodynamic instability. Morbidity and mortality have been reported to be 17% and 8.3%, respectively, in patients with acute colonic diverticular bleeding who have undergone urgent surgery.18 Normally, surgery by means of laparotomy or laparoscopy is considered the treatment of choice if hemodynamic instability occurs or in case of failure of less invasive treatments such as endoscopy or angiography.31 The colonic resection may be limited to the segment in which the bleeding is located. On the other hand, in patients with persistent bleeding and no angiographic or endoscopic identification of a definite bleeding source a subtotal colectomy may be required.32 In 13.8% of the cases, an urgent colectomy becomes necessary, but is burdened by high mortality and morbidity rates (20%).18 In all the analyzed studies, urgent colonoscopy was performed to achieve the diagnosis of diverticular bleeding. Timing and type of preparation to this procedure are still matter of debate.31,33 It is commonly accepted that early colonoscopy within 24 hr may improve both diagnosis and management of the bleeding thus reducing the length of hospital stay. Once the bleeding site was successfully identified and did not stop spontaneously, the majority of authors (Niikura et al13, Tanaka et al15, Poncet et al17, and Chen et al18) performed endoscopic hemostasis with various techniques such as epinephrine injection, multipolar or heat probe coagulation, endoclips placement, and band ligation. When those latter failed, TAE was performed in order to stop the bleeding. Surgical colectomy was considered only in case of hemodynamic instability, or after arteriography for identification of the site of diverticular bleeding, or when TAE was unsuccessful. All patients with active bleeding on admission enrolled in Fujino's study were treated with endoclips placement.12 Drawing on our review, we can suggest that the management of diverticular bleeding should go through 4 phases: primarily active surveillance pending the remission, followed in cases of not spontaneous hemostasis, with an interventional endoscopic treatment as first-line therapy. In all cases, when the endoscopic approach is not curative, a second-line treatment should be considered. TAE, however, although effective, requires a blood flow of more than 1 mL/min,34 angiography must be performed during the active bleeding, which is often intermittent, in order to detect the exact source and the use of contrast in elderly patients may cause acute renal failure. Finally, the risk of bowel infarction after TAE has been reported 13% to 33% of patients.11 Heianna et al10 proposed a colonoscopy-guided superselective arterial embolization for patients in whom endoscopic treatment was not effective. In these cases, some radiopaque clips were placed at the bleeding site during colonoscopy to mark the embolization site for the subsequent angiography. We consider TAE useful as a second conservative step before resorting to surgery, mostly in those cases where surgery can present several perioperative complications. In fact, as reported in the literature, surgery should be reserved only to patients that cannot be managed conservatively. As reported, the low failure rate of both the conservative treatments encourage this kind of approach, reserving surgery for the instances without alternative (severe hemorrhage and hemodynamically unstable patients). The surgical management depends on the bleeding site: hemicolectomy after diagnosis of left colon diverticula or total abdominal colectomy with ileorectal anastomosis in case of uncertainty of the exact bleeding site. The incidence of overall recurrent colonic diverticular bleeding was 38%.35 Recurrence rate within the first year was 15%, which becomes 30% by the end of the second year. Colonic diverticular bleeding often recurs within a short period of time and nonsteroidal anti-inflammatory and anti-platelet drugs increase the risk of recurrence.
FIGURE 2.

Transcatheter arterial embolization of colonic diverticular bleeding.
CONCLUSION
Colonic diverticular bleeding stops spontaneously in over 80% of cases but often recurs. According to the most recent literature, the management of acute or persistent colonic diverticular bleeding has evolved with the advent of interventional endoscopy and angiography. That allowed restricting urgent colectomy only in case of failure of such less invasive procedures or hemodynamic instability of the patient. However, as no RCTs are available many points of debate still remain open.
Footnotes
Abbreviations: CT = computed tomography, EMBASE = Excerpta Medica Database, GI = gastrointestinal, LGIB = lower gastrointestinal bleeding, NRCCTs = nonrandomized clinical controlled trials, PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses, RCTs = randomized controlled trials, SIGN = Scottish Intercollegiate Guidelines Network, TAE = transcatheter arterial embolization.
Authors’ contribution: All authors contributed equally to the manuscript drafting.
The authors are the only ones responsible for the content and writing of the paper.
The authors have no conflicts of interest to disclose.
REFERENCES
- 1.Barnert J, Messmann H. Diagnosis and management of lower gastrointestinal bleeding. Nat Rev Gastroenterol Hepatol 2009; 6:637–646. [DOI] [PubMed] [Google Scholar]
- 2.Hreinsson JP, Gumundsson S, Kalaitzakis E, et al. Lower gastrointestinal bleeding: incidence, etiology, and outcomes in a population-based setting. Eur Gastroenterol Hepatol 2013; 25:37–43. [DOI] [PubMed] [Google Scholar]
- 3.Nagata N, Niikura R, Aoki T, et al. Impact of discontinuing non-steroidal antiinflammatory drugs on long-term recurrence in colonic diverticular bleeding. World J Gastroenterol 2015; 21:1292–1298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hoedema RE, Luchtefeld MA. The management of lower gastrointestinal hemorrhage. Dis Colon Rectum 2005; 48:2010–2024. [DOI] [PubMed] [Google Scholar]
- 5.Rasuli P, Doumit J, Boulos M, et al. Factors influencing the yield of mesenteric angiography in lower gastrointestinal bleed. World J Radiol 2014; 6:218–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Raphaeli T, Menon R. Current treatment of lower gastrointestinal hemorrhage. Clin Colon Rectal Surg 2012; 25:219–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kaltenbach T, Watson R, Shah J, et al. Colonoscopy with clipping is useful in the diagnosis and treatment of diverticular bleeding. Clin Gastroenterol Hepatol 2012; 10:131–137. [DOI] [PubMed] [Google Scholar]
- 8.Moher D, Altman DG, Liberati A, et al. PRISMA statement. Epidemiology 2011; 22:128.author reply 128. [DOI] [PubMed] [Google Scholar]
- 9.Scottish Intercollegiate Guidelines Network (SIGN) guidelines. Available at: http://www.sign.ac.uk/guidelines/fulltext/50/checklist3 [Accessed: July 30, 2014]. [Google Scholar]
- 10.Heianna J, Miyauchi T, Yamano H, et al. Management of angiogram-negative acute colonic hemorrhage: safety and efficacy of colonoscopy-guided superselective embolization. Tech Coloproctol 2014; 18:647–652. [DOI] [PubMed] [Google Scholar]
- 11.Couto-Worner I, González-Conde B, Estévez-Prieto E, et al. Colonic diverticular bleeding: urgent colonoscopy without purging and endoscopic treatment with epinephrine and hemoclips. Rev Esp Enferm Dig 2013; 105:495–498. [DOI] [PubMed] [Google Scholar]
- 12.Fujino Y, Inoue Y, Onodera M, et al. Risk factors for early re-bleeding and associated hospitalization in patients with colonic diverticular bleeding. Colorectal Dis 2013; 15:982–986. [DOI] [PubMed] [Google Scholar]
- 13.Niikura R, Nagata N, Yamada A, et al. Recurrence of colonic diverticular bleeding and associated risk factors. Colorectal Dis 2012; 14:302–305. [DOI] [PubMed] [Google Scholar]
- 14.Suh S, Seo PJ, Park H, et al. The risk factors for colonic diverticular bleeding. Korean J Gastroenterol 2012; 60:349–354. [DOI] [PubMed] [Google Scholar]
- 15.Tanaka Y, Motomura Y, Akahoshi K, et al. Predictive factors for colonic diverticular rebleeding: a retrospective analysis of the clinical and colonoscopic features of 111 patients. Gut Liver 2012; 6:334–338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lee KK, Shah SM, Moser MA. Risk factors predictive of severe diverticular hemorrhage. Int J Surg 2011; 9:83–85. [DOI] [PubMed] [Google Scholar]
- 17.Poncet G, Heluwaert F, Voirin D, et al. Natural history of acute colonic diverticular bleeding: a prospective study in 133 consecutive patients. Aliment Pharmacol Ther 2010; 32:466–471. [DOI] [PubMed] [Google Scholar]
- 18.Chen CY, Wu CC, Jao SW, et al. Colonic diverticular bleeding with comorbid diseases may need elective colectomy. Gastrointest Surg 2009; 13:516–520. [DOI] [PubMed] [Google Scholar]
- 19.Jansen A, Harenberg S, Grenda U, et al. Risk factors for colonic diverticular bleeding: a Westernized community based hospital study. World J Gastroenterol 2009; 15:457–461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yamada A, Sugimoto T, Kondo S, et al. Assessment of the risk factors for colonic diverticular hemorrhage. Dis Colon Rectum 2008; 51:116–120. [DOI] [PubMed] [Google Scholar]
- 21.Jensen DM, Machicado GA, Jutabha R, et al. Urgent colonoscopy for the diagnosis and treatment of severe diverticular hemorrhage. N Eng J Med 2000; 342:78–82. [DOI] [PubMed] [Google Scholar]
- 22.Jacobs DO. Clinical practice. Diverticulitis. N Eng J Med 2007; 357:2057–2066. [DOI] [PubMed] [Google Scholar]
- 23.Goldberg SM, Nivatvongs S, Rothenberger DA. Schwartz SI, Shires GT, Spencer FC. Diverticular disease with acute hemorrhage. Principles of Surgery. New York: McGraw-Hill; 1989. 255–259. [Google Scholar]
- 24.Myron L. Bleeding colonic diverticular. J Clin Gastroenterol 2008; 42:1156–1158. [DOI] [PubMed] [Google Scholar]
- 25.Sugihara Y, Kudo SE, Miyachi H, et al. Analysis of risk factors for colonic diverticular bleeding: a Marche case-control study. Gut Liver 2015; Published online June 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Aldoori WH, Giovannucci EL, Rimm EB, et al. Use of acetaminophen and nonsteroidal anti-inflammatory drugs: a prospective study and the risk of symptomatic diverticular disease in men. Arch Fam Med 1998; 7:255–260. [DOI] [PubMed] [Google Scholar]
- 27.De Scheerder IK, Van de Kraay AM, Lamers JM, et al. Myocardial malondialdehyde and uric acid release after short-lasting coronary occlusions during coronary angioplasty: potential mechanisms for free radical generation. Am J Cardiol 1991; 68:392–395. [DOI] [PubMed] [Google Scholar]
- 28.Okamoto T, Watabe H, Yamada A, et al. The association between arteriosclerosis related diseases and diverticular bleeding. Int J Colorectal Dis 2012; 27:1161–1166. [DOI] [PubMed] [Google Scholar]
- 29.Nakatsu S, Yasuda H, Maehata T, et al. Urgent computed tomography for determining the optimal timing of colonoscopy in patients with acute lower gastrointestinal bleeding. Intern Med 2015; 54:553–558. [DOI] [PubMed] [Google Scholar]
- 30.Vernava AM, III, Moore BA, Longo WE, et al. Lower gastrointestinal bleeding. Dis Colon Rectum 1997; 40:846–858. [DOI] [PubMed] [Google Scholar]
- 31.Ghassemi KA, Jensen DM. Lower GI bleeding: epidemiology and management. Curr Gastroenterol Rep 2013; 15:333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Stollman NH, Raskin JB. Diagnosis and management of diverticular disease of the colon in adults. Am J Gastroenterol 1999; 94:3117–3118. [DOI] [PubMed] [Google Scholar]
- 33.Lhewa DY, Strate LL. Pros and cons of colonoscopy in management of acute lower gastrointestinal bleeding. World J Gastroenterol 2012; 18:1185–1190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Zuckerman DA, Bocchini TP, Birnbaum EH. Massive hemorrhage in the lower gastrointestinal tract in adults: diagnostic imaging and intervention. Am J Roentgenol 1993; 161:703–711. [DOI] [PubMed] [Google Scholar]
- 35.Niikura R, Nagata N, Yamada A, et al. Recurrence of colonic diverticular bleeding and associated risk factors. Colorectal Dis 2012; 14:302–305. [DOI] [PubMed] [Google Scholar]