

Abstract
To our knowledge, the clinical characteristics of traumatic vertebral fractures and concomitant fractures of the rib (TVF-RF) have not been described in previous studies.
To investigate the clinical characteristics of patients managed for TVF-RF. A retrospective study of 3142 patients who presented with traumatic vertebral fractures was performed. Two hundred twenty-six patients (7.2%) suffered from TVF-RF.
Incidence rate ratios were then calculated with respect to the level of injury to the spine, the ASIA classification of neurological deficits and age.
There were 171 male (75.7%) and 55 female (24.3%) patients with a mean age of 43.8 years. The most common mechanisms were falls from high heights in 81 cases and road traffic crashes in 67 cases. Right-sided rib injury occurred in 106 cases, left-sided injury occurred in 76 cases, and bilateral injury occurred in 44 cases. The most frequent location of the rib fractures was from the fourth rib to the ninth rib (70.3%, 510/725). Initial pulmonary complications (IPC) after trauma occurred in 116 cases (51.3%). The mortality rate for the entire group was 1.3% (3/226). The patients with thoracic vertebral fractures and neurological deficits had a higher frequency of multiple rib fractures and IPC than the other patients (P < 0.05). With the increased number of rib fractures, the frequency of IPC and mean intensive care unit (ICU) length of stay also increased.
The rates of complications for patients with rib fractures were significantly different from those without rib fractures. We should pay much attention to the patients who presented with thoracic vertebral fractures and neurological deficits for minimizing further complications and mortality in such patients who had a higher frequency of multiple rib fractures and IPC than the other patients.
INTRODUCTION
Traumatic injuries are the most common cause of death among young people and are a leading cause of disability and years of life lost.1–3 Spinal fractures are common after traumatic injuries and are associated with the poorest functional outcomes and the lowest rates of return to work after injury.2 The assessment of patients with spinal trauma requires awareness of the patterns of associated injuries. The associated injuries of spinal fractures were examined in previous studies, with the most common associated nonspinal cord injuries being extremity and head injuries.4–6 In a study by Leucht et al,6 18.5% of the patients with a spine fracture suffered from a thoracic injury, the third most common injury associated with traumatic fracture of the spine. The clinical characteristics of vertebral fractures and concomitant fractures of the sternum have been well described by Vioreanu et al7 these authors suggested that the relative severity of the neurological compromise and the attendant injuries in the upper thoracic fracture group from their study offered compelling evidence in support of the “fourth column” theory, as expressed by Berg.8
An important but frequently overlooked combination is that of spinal and rib fractures. Rib fractures are a painful and disabling injury commonly found among trauma patients. Many studies have pointed out that the unexpected frequency of rib fractures and the rib fractures did adverse impact on the patients.9,10 Work by Bulger et al11 on the impact of rib fractures after blunt trauma has demonstrated the linear relationship between age, increasing numbers of rib fractures and complications including mortality. To our knowledge, the clinical characteristics of traumatic vertebral fractures and concomitant fractures of the rib have not been described in previous studies. In this study, we sought to examine correlations, such as the occurrence of traumatic vertebral fractures and concomitant fractures of the rib. In addition, we analyzed our study population to determine the relationship between the fracture distribution and the level of injury to the spinal column, the ASIA classification of neurological deficit or the different age groups and if there were any correlations among age, gender, the cause of the accident and the fracture distribution. Through the study, we want to know what the information of the study means and how it affects us, whether this information is valuable to primary healthcare providers, such as paramedics or trauma specialists in minimizing further complications and mortality in such patients. The information can change the way patients are handled from site of accident to emergency response centers and provide recommendations to enforce safer workplace environments.
MATERIALS AND METHODS
Study Site
Chongqing Municipality is a city located in southwest China, and the rural population accounted for 61.7% of the total population.12 The data were collected from Third Military Medical University affiliated hospitals which were the 2 biggest public tertiary hospitals located in the Shapingba district. Shapingba district is a core district located in the northwest region of Chongqing.
Patient Survey
This study was a retrospective cross-sectional study using data from the Military Hospital Information Registry Database gathered from January 2001 to December 2010. The procedure was approved by the Ethics Committee of the Third Military Medical University. The clinical notes for all of the patients with rib fractures associated with spinal column fractures who had been admitted to our unit were reviewed. The level of spinal fracture and rib fracture, the presence or absence of underlying neurological symptoms, the classification of neurological deficit, the presence of associated injuries, and the type of management provided to each patient were studied.
Statistical Analyses
All statistical analyses were performed using SPSS 15.0 (SPSS, Inc., Chicago, IL). Statistical analyses were conducted using the Student t test and nonparametric tests. Statistical analyses of the quantitative data were performed for all variables. Chi-squared testing of frequency data was also performed where appropriate. All P-values reported are 2-sided, the significance level was set at 0.05.
RESULTS
General Characteristics
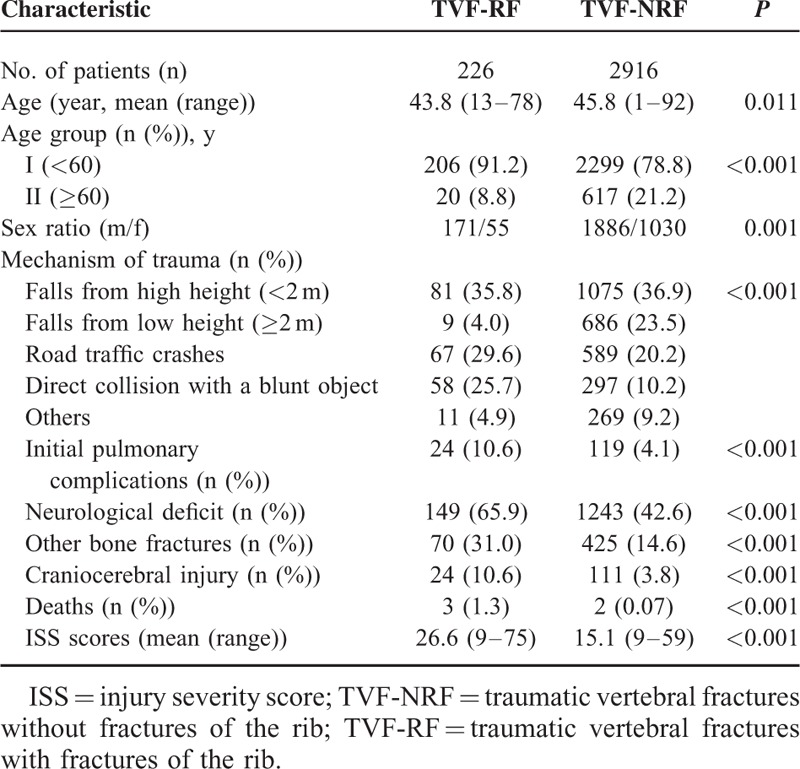
In total, 3142 patients were admitted to the Third Military Medical University Affiliated Hospitals, and 226 patients (7.2%, 95% CI: 6.3–8.1%) presented with traumatic vertebral fractures and concomitant rib fractures. The overall annual incidence of rib fractures associated with vertebral fractures was 21.6 ± 7.1 cases per 100,000 hospital admissions per year. The annual incidence rates fluctuated between years, but the rates generally increased with the year of admission from 9.4 cases per 100,000 hospital admissions in 2001 to 24.8 cases per 100,000 hospital admissions in 2010. The rates of complications for patients with rib fractures were significantly different from those patients without rib fractures among all of the patients with traumatic vertebral fractures. Additionally, a rib fracture was a predictor of other more serious injuries (Table 1).
TABLE 1.
Characteristics of Patients With Traumatic Vertebral Fractures With/Without Fractures of the Rib
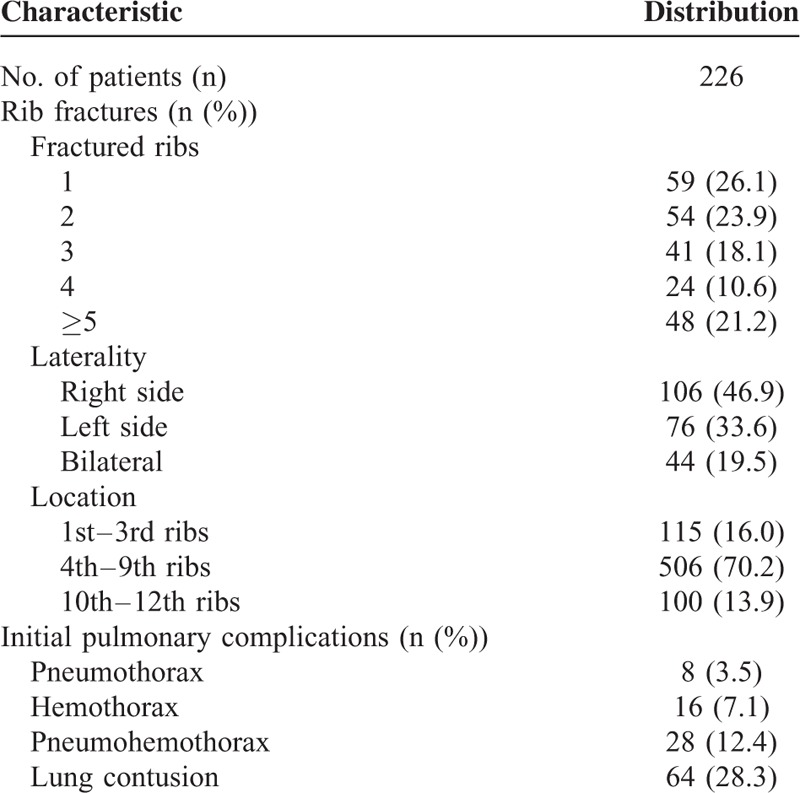
The general characteristics of the patients with traumatic vertebral fractures and concomitant fractures of the rib are listed in Table 2. The study group included 226 patients with an average age of 43.8 ± 11.0 years (95% CI: 42.4–45.2 years). The most common mechanism of trauma for patients with traumatic vertebral fractures and concomitant rib fractures was a fall from a high height (35.8%, 81/226, 95% CI: 29.5–42.1%). Among all 226 patients, 116 patients (51.3%, 95% CI: 44.8–57.8%) presented with initial pulmonary complications (IPC) after the trauma. Other associated bone fractures were recorded for 70 patients (31.0%, 95% CI: 25.0–37.0%), including information on 99 fractures sites, such as the extremities (43), scapula (21), pelvis (13), clavicle (13), sternum (5), skull (2), and mandible (2). Fifty-nine patients sustained 1 rib fracture, 54 had 2 rib fractures, 41 suffered 3 rib fractures, 24 suffered 4 rib fractures, and 48 suffered 5 or more rib fractures. A right-sided injury occurred in 106 cases, a left-sided injury occurred in 76 cases, and a bilateral injury occurred in 44 cases. The most frequent location of the rib fractures was from the fourth rib to the ninth rib (70.2%, 506/721, 95% CI: 66.9–73.5%).
TABLE 2.
General Characteristics of Patients With Traumatic Vertebral Fractures and Concomitant Fractures of the Rib
There were 24 patients (10.6%, 95% CI: 6.6–14.6%) with a craniocerebral injury, 4 patients with an injury of the peripheral nerves, 6 patients with shock, 2 patients with retroperitoneal hematoma, 2 patients with a kidney contusion, 3 patients with multiple organ failure, and 1 patient each with pneumopericardium, a cardiac contusion, and an injury of the urinary tract. Thirty-nine patients (17.3%, 39/226, 95% CI: 12.9–21.7%) suffered 45 complications: bed sores (16), pulmonary infection (15), urinary tract infection (4), postoperative cerebrospinal fluid leakage (3), sepsis (2), deep venous thrombosis (2), surgical site infection (2), and fungal enteritis (1). Thirteen patients (5.8%, 95% CI: 2.8–8.8%) presented with a history of cardiopulmonary resuscitation, and 3 patients died. The mortality rate for the entire group was 1.3%. A total of 149 patients (65.9%, 95% CI: 59.7–72.1%) suffered a spinal cord injury (SCI). Using the ASIA classification, 89 patients (39.4% of the total study population) exhibited complete motor and sensory deficits (ASIA A). Sixty patients (26.5%) suffered from incomplete motor and sensory deficits (ASIA B, C, and D). Seventy-seven patients (34.1%) experienced no motor or sensory deficits (ASIA E).
Characteristics According to the Level of Injury to the Spinal Column
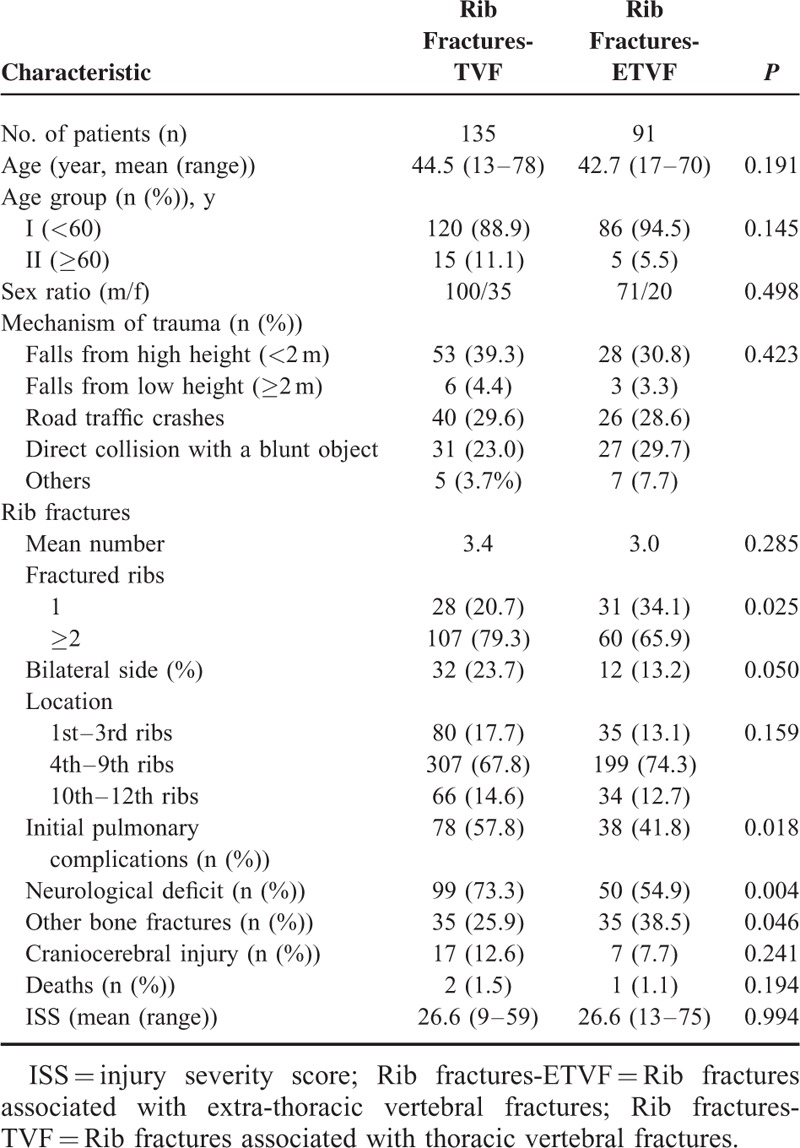
The patients were divided into 2 groups according to the level of injury to the spinal column: rib fractures associated with thoracic vertebral fractures (Rib fractures-TVF) and rib fractures associated with extra-thoracic vertebral fractures (Rib fractures-ETVF). Among all of the 3142 traumatic spinal fracture cases, 1027 patients presented with thoracic vertebral fractures. In the Rib fractures-TVF group, there were 135 patients with an average age 44.5 ± 12.0 years (95% CI: 42.5–46.5 years). There were 35 patients (25.9%, 95% CI: 18.5–33.3%) who suffered from other bone fractures at the following sites: scapula (11), pelvis (6), clavicle (4), sternum (2), skull (1), mandible (1), and extremities (26). The patients with neurological deficits accounted for 73.3% of the Rib fractures-TVF group (99/135, 95% CI: 65.8–80.8%); 67 of these patients (49.6%) had complete neurological deficits (ASIA A), and 32 patients (23.7%) had incomplete deficits (ASIA B, C, or D). In the Rib fractures-ETVF group, there were 91 patients with an average age 42.7 ± 9.4 years (95% CI: 40.7–44.7 years). There were 35 patients (38.5%, 95% CI: 28.5–48.5%) who suffered from other bone fractures at the following sites: scapula (9), pelvis (7), clavicle (9), sternum (3), skull (1), mandible (1), and extremities (17). The patients with neurological deficits accounted for 54.9% of the Rib fractures-ETVF group (50/91, 95% CI: 44.7–65.1%); 22 of these patients (24.2%) had complete neurological deficits (ASIA A), and 28 patients (30.8%) had incomplete deficits (ASIA B, C, or D). The differences between the 2 groups according to the level of injury to the spinal column are shown in Table 3. The frequency of multiple rib fractures, IPC, neurological deficits, and other bone fractures in the Rib fractures-TVF group was higher than the values for the Rib fractures-ETVF group.
TABLE 3.
Characteristics of Patients According to the Level of Injury to the Spinal Column
Characteristics According to the ASIA Classification of Neurological Deficit
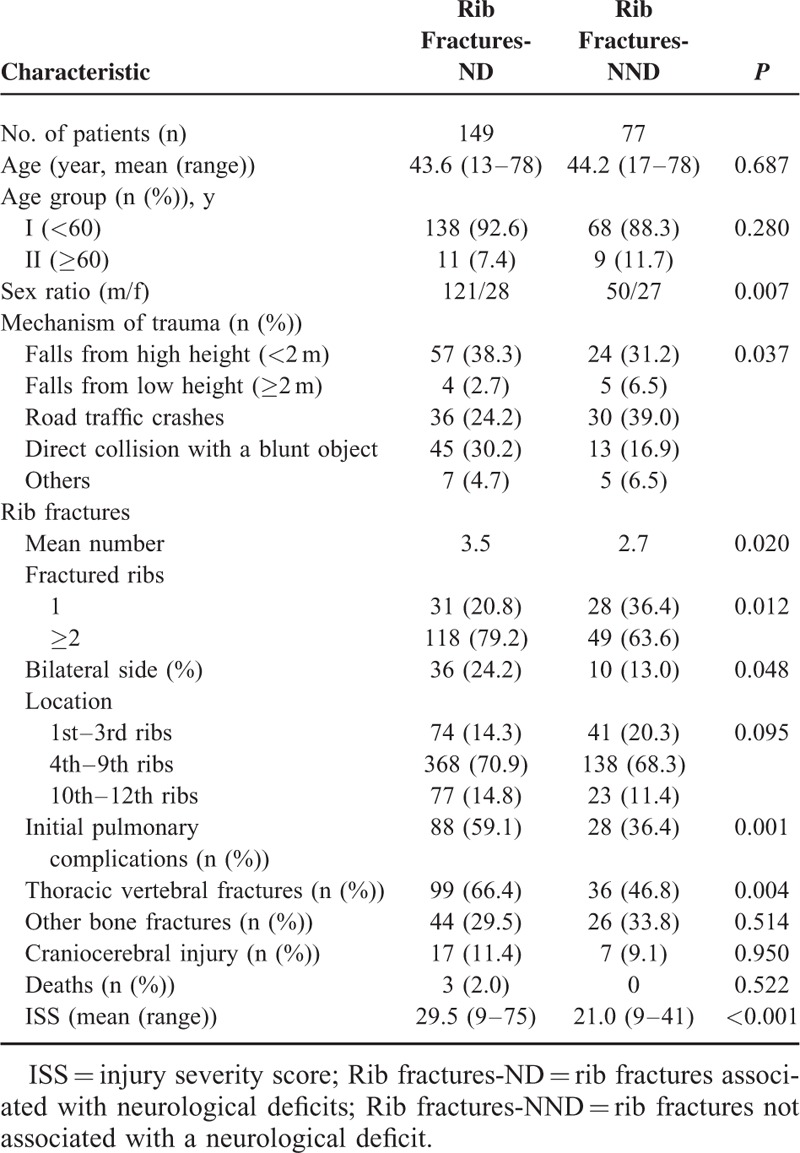
The patients were divided into 2 groups according to the ASIA classification of neurological deficit: rib fractures associated with neurological deficits (Rib fractures-ND) graded as ASIA A, B, C, and D (Rib fractures-ND) and rib fractures associated with no neurological deficit graded as ASIA E (Rib fractures-NND). Among all of the 3142 traumatic spinal fractures, 1392 patients presented with neurological deficits. In the Rib fractures-ND group, there were 149 patients with an average age of 43.6 ± 11.0 years (95% CI: 41.8–45.4 years). There were 44 patients (29.5%, 95% CI: 22.2–36.8%) who suffered from other bone fractures at the following sites: scapula (14), pelvis (7), clavicle (6), sternum (4), skull (1), mandible (2), and extremities (36). In this group, 99 patients (66.4%, 95% CI: 58.5–74.0%) suffered from thoracic vertebral fractures, and 17 patients (11.4%, 95% CI: 6.3–16.5%) suffered from a craniocerebral injury. In the Rib fractures-NND group, there were 77 patients with an average age of 44.2 ± 11.2 years (95% CI: 41.7–46.8 years). There were 26 patients (33.8%, 95% CI: 23.2–44.4%) who suffered from other bone fractures at the following sites: scapula (7), pelvis (6), clavicle (7), sternum (1), skull (1), and extremities (7). In the Rib-fractures-NND group, 36 patients (46.8%, 95% CI: 35.6–58.0%) suffered from thoracic vertebral fractures, and 7 patients (9.1%, 95% CI: 35.6–58.0%) suffered from a craniocerebral injury. The differences between the 2 groups according to the ASIA classification of neurological deficits are shown in Table 4. There were significant differences in the distribution of the mechanism of trauma and the sex ratio between the 2 groups, and the mean number of rib fractures, bilateral side rib fractures, IPC, thoracic vertebral fractures and the frequency of multiple rib fractures were higher in the Rib fractures-ND group than the Rib fractures-NND group.
TABLE 4.
Characteristics of Patients According to the ASIA Classification of Neurological Deficit
Characteristics According to the Different Age Groups
The patients were divided into 2 groups according to different age groups: traumatic vertebral fractures and concomitant fractures of the rib among patients younger than 60 years (TVF-RF < 60) and traumatic vertebral fractures and concomitant fractures of the rib among elderly patients older than 60 years (TVF-RF ≥ 60). In the TVF-RF < 60 group, there were 206 patients; 64 patients in this group (31.1%, 95% CI: 24.8–37.4%) suffered from other bone fractures. Twenty patients (9.7%, 95% CI: 5.6–13.7%) suffered from a craniocerebral injury, and 109 patients (52.9%, 95% CI: 46.1–59.7%) suffered from IPC. In the TVF-RF ≥ 60 group, there were 20 patients; 6 patients in this group (30.0%, 95% CI: 10.0–50.5%) suffered from other bone fractures, 4 patients (20.0%, 95% CI: 2.6–37.4%) suffered from a craniocerebral injury, and 7 patients (35.0%, 95% CI: 14.1–55.9%) suffered from IPC (Table 5). The frequency of patients with IPC and mean intensive care unit (ICU) length of stay increased with the increasing number of rib fractures regardless of the age group (Fig. 1).
TABLE 5.
Characteristics of Patients According to Different Age Groups
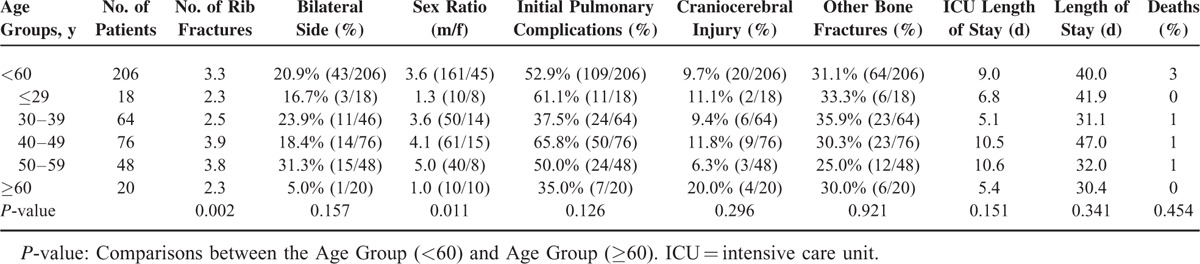
FIGURE 1.
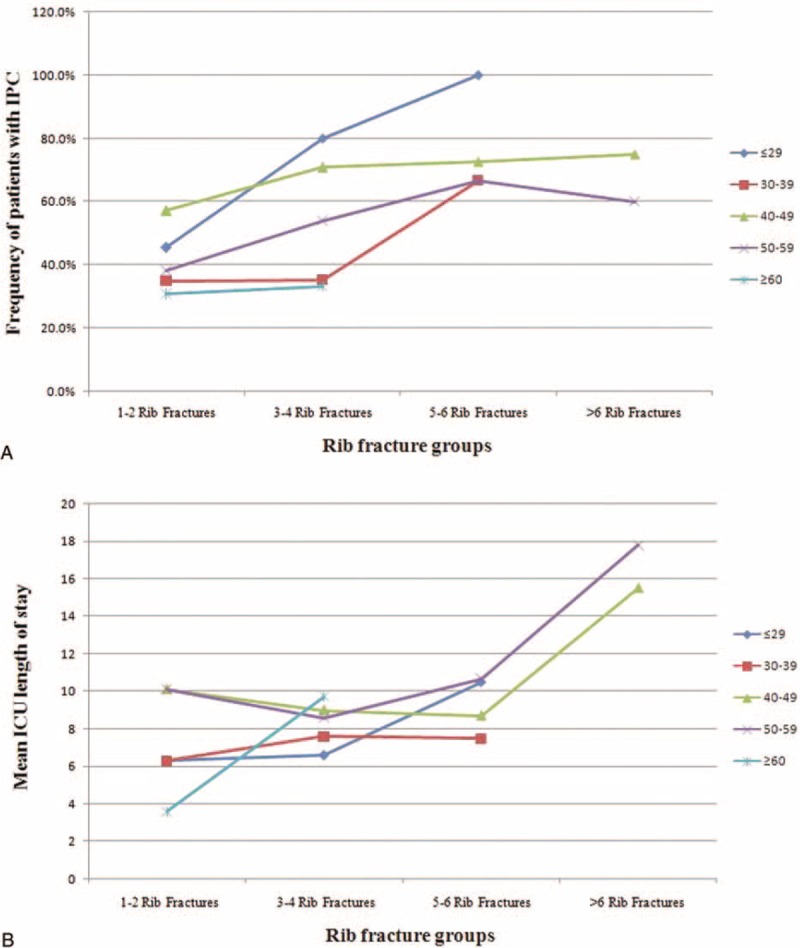
The effect of the number of rib fractures and age on the number of initial pulmonary complications (IPC) after trauma and the mean intensive care unit (ICU) length of stay. The patients were grouped into 5 age and 4 rib fracture divisions. (A) The effect of the number of rib fractures and age on the number of initial pulmonary complications (IPC) after trauma. (B) The effect of the number of rib fractures and age on the mean ICU length of stay.
DISCUSSION
Now, the incidence of rib fractures associated with spinal fracture is uncertain. Hasler et al13 reported that 17.78% of 24,000 patients with spinal fractures or dislocations had sustained a chest injury, which was the second most common associated injury in their study followed by injuries to the extremities. Rib fractures are very common injuries, comprising up to 10% of admissions to trauma services.11,14 The overall annual incidence of rib fractures associated with vertebral fractures was 215.9 ± 71.0 cases per 100,000 hospital admissions per year. The annual incidence rates fluctuated between years, but the rates generally increased with the year of admission from 9.4 cases per 100,000 hospital admissions in 2001 to 24.8 cases per 100,000 hospital admissions in 2010.
We report an incidence of 7.2% of rib fractures associated with vertebral fractures among cases of traumatic spinal fractures. When we analyzed our 2 subgroups according to the level of injury to the spinal column, there were 91 cases with an attendant rib fracture out of 2115 extra-thoracic traumatic vertebral fracture cases, giving an incidence of 4.3%. This rate compares to an incidence of 13.1% within the thoracic spine group. Rib fractures should be identified in the primary survey of spinal fracture patients especially the patients presented with thoracic vertebral fractures and then key steps may be started by the initial clinician such as paramedics, EMTs, or trauma specialists to help prevent significant morbidity. We should not use pain masking drugs before conducting a comprehensive diagnosis to avoid mask of important symptoms and conditions such as rib fracture and abdominal disease. Paramedics and EMTs should pay much attention to the patients presented with spinal and rib fractures then prevent secondary lesion when carrying these injured patients. When we analyzed our 2 subgroups according to the ASIA classification of neurological deficits, there were 149 cases with an attendant rib fracture out of 1392 neurological deficit traumatic vertebral fracture cases, giving an incidence of 10.7%. This rate compares to an incidence of 4.4% within the rib fractures not associated with a neurological deficit (Rib fractures-NND) group. The serious spinal fracture and SCI characterize severe, multiple injury and complex injury, most trauma specialists may pay much attention to the spine and spinal cord, rib fracture maybe misdiagnosis and delayed diagnosis. So trauma specialists should pay much more attention to the spinal fracture patients especially patients presented with thoracic vertebral fractures and neurological deficits in avoiding misdiagnosis and delayed diagnosis and minimizing further complications and mortality in such patients.
Rib fractures are commonly associated with pulmonary contusions, which may significantly contribute to the pulmonary morbidity seen in multisystem injury patients.15–21 Battle et al15 suggested that the risk factors for mortality in patients sustaining blunt chest wall trauma were a patient age of 65 years or older, 3 or more rib fractures and the presence of preexisting diseases, especially cardiopulmonary diseases. Despite lower indices of injury severity, even after considering comorbidities, mortality was significantly increased in elderly patients admitted to a trauma centre with rib fractures.16 However, Testerman18 and Holcomb et al19 suggested that patient as young as 45 years and who presented with more than 4 rib fractures were risk factors for adverse outcomes. An increasing number of rib fractures may cause significant morbidity on younger patients than previously appreciated.20 According to previous studies, efforts to decrease rib fracture morbidity should focus not only on elderly patients who presented with presence of pre-existing diseases but also on young patients who were hurt by great energy which transmitted to the chest wall. Early diagnosis and timely treatment are essential to reduce the mortality and improve the prognosis of patients presented with spinal and rib fractures.
In the present study, the rates of complications for patients with rib fractures were significantly more than those without rib fractures. The younger patients, particularly the patients with an age between 40 and 49 years, had the highest number of rib fractures, highest frequency of bilateral side rib fractures, highest frequency of IPC, longer ICU length of stay and longer length of total hospital stay; additionally, all 3 patients who died were young patients. With the increasing number of rib fractures, the frequency of IPC also increased. We speculate that the main reason was the difference in trauma mechanisms. The most common mechanism of trauma among adult patients (>18 years) with a diagnosis of chest trauma and 3 or fewer fractured ribs was a motor vehicle accident.22 Motor vehicle crashes were the most common mechanism of trauma among the patients with rib fractures.23 In cases of traumatic spinal fractures, more violent injuries were shown to occur among the younger groups of patients with high-risk labor occupations, such as construction; moreover, falls have become the main cause of spine trauma for young patients.6,24,25 Based on these data, primary healthcare providers, such as paramedics, EMTs, or trauma specialists should pay much attention to the young patients presented with spinal fractures especially patients caused by motor vehicle crashes. Our present study had several limitations, including the retrospective study design and the small number of patients. However, we think that the results of this study provide interesting clinical data which is valuable to primary health care providers in minimizing further complications and mortality in such patients despite these limitations.
CONCLUSIONS
Our results confirm that the annual incidence of TVF-RF fluctuated but generally increased with each year of admission. The patients with thoracic vertebral fractures and those with neurological deficits had a higher frequency of multiple rib fractures and IPC than the other patients. The patients with an increased number of rib fractures were at risk for prolonged ICU stays and an increased frequency of IPC. Based on these data, primary healthcare providers, such as paramedics, EMTs, or trauma specialists should pay much attention to the patients presented with thoracic vertebral fractures and neurological deficits in minimizing further complications and mortality in such patients.
Footnotes
Abbreviations: ICU = intensive care unit, IPC = initial pulmonary complications, ISS = injury severity score, Rib fractures-ETVF = Rib fractures associated with extra-thoracic vertebral fractures, Rib fractures-ND = rib fractures associated with neurological deficits, Rib fractures-NND = rib fractures not associated with a neurological deficit, Rib fractures-TVF = Rib fractures associated with thoracic vertebral fractures, SCI = spinal cord injury, TVF-NRF = traumatic vertebral fractures without fractures of the rib, TVF-RF = traumatic vertebral fractures with fractures of the rib.
The authors have no conflicts of interest to disclose.
This work was supported by the Foundation of the State Key Laboratory of Robotics (no. 2014-O12) and the Medjaden Academy & Research Foundation for Young Scientists (no. MJR20150013).
REFERENCES
- 1.Rivara FP, Grossman DC, Cummings P. Injury prevention. N Engl J Med 1997; 337:543–548. [DOI] [PubMed] [Google Scholar]
- 2.Johansson C, Mellström D, Rosengren K, et al. Prevalence of vertebral fractures in 85-year-olds. Radiographic examination of 462 subjects. Acta Orthop Scand 1993; 64:25–27. [DOI] [PubMed] [Google Scholar]
- 3.Price C, Makintubee S, Herndon W, et al. Epidemiology of traumatic spinal cord injury and acute hospitalization and rehabilitation charges for spinal cord injuries in Oklahoma, 1988–1990. Am J Epidemiol 1994; 139:37–47. [DOI] [PubMed] [Google Scholar]
- 4.Heidari P, Zarei MR, Rasouli MR, et al. Spinal fractures resulting from traumatic injuries. Chin J Traumatol 2010; 13:3–9. [PubMed] [Google Scholar]
- 5.Pirouzmand F. Epidemiological trends of spine and spinal cord injuries in the largest Canadian adult trauma center from 1986 to 2006. J Neurosurg Spine 2010; 12:131–140. [DOI] [PubMed] [Google Scholar]
- 6.Leucht P, Fischer K, Muhr G, et al. Epidemiology of traumatic spine fractures. Injury 2009; 40:166–172. [DOI] [PubMed] [Google Scholar]
- 7.Vioreanu MH, Quinlan JF, Robertson I, et al. Vertebral fractures and concomitant fractures of the sternum. Int Orthop 2005; 29:339–342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Berg EE. The sternal-rib complex. A possible fourth column in thoracic spine fractures. Spine 1993; 18:1916–1919. [PubMed] [Google Scholar]
- 9.Lee RB, Bass SM, Morris JA, Jr, et al. Three or more rib fractures as an indicator for transfer to a level 1 trauma center: a population-based study. J Trauma 1990; 30:689–694. [DOI] [PubMed] [Google Scholar]
- 10.Zeigler DW, Agarwal NN. The morbidity and mortality of rib fractures. J Trauma 1994; 37:975–979. [DOI] [PubMed] [Google Scholar]
- 11.Bulger EM, Arneson MA, Mock CN, et al. Rib fractures in the elderly. J Trauma 2000; 48:1040–1046.discussion 1046–1047. [DOI] [PubMed] [Google Scholar]
- 12.Wang H, Li C, Xiang Q, et al. Epidemiology of spinal fractures among the elderly in Chongqing, China. Injury 2012; 43:2109–2116. [DOI] [PubMed] [Google Scholar]
- 13.Hasler RM, Exadaktylos AK, Bouamra O, et al. Epidemiology and predictors of spinal injury in adult major trauma patients: European cohort study. Eur Spine J 2011; 20:2174–2180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Demetriades D, Sava J, Alo K, et al. Old age as a criterion for trauma team activation. J Trauma 2001; 51:754–757. [DOI] [PubMed] [Google Scholar]
- 15.Battle CE, Hutchings H, Evans PA. Risk factors that predict mortality in patients with blunt chest wall trauma: a systematic review and meta-analysis. Injury 2012; 43:8–17. [DOI] [PubMed] [Google Scholar]
- 16.Bergeron E, Lavoie A, Clas D, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma 2003; 54:478–485. [DOI] [PubMed] [Google Scholar]
- 17.Flagel BT, Luchette FA, Reed RL, et al. Half-a-dozen ribs: the breakpoint for mortality. Surgery 2005; 138:717–723.discussion 723–725. [DOI] [PubMed] [Google Scholar]
- 18.Testerman GM. Adverse outcomes in younger rib fracture patients. South Med 2006; 99:335–339. [DOI] [PubMed] [Google Scholar]
- 19.Holcomb JB, McMullin NR, Kozar RA, et al. Morbidity from rib fractures increases after age 45. J Am Coll Surg 2003; 196:549–555. [DOI] [PubMed] [Google Scholar]
- 20.Miller PR, Croce MA, Bee TK, et al. ARDS after pulmonary contusion: accurate measurement of contusion volume identifies high-risk patients. J Trauma 2001; 51:223–228.discussion 229–230. [DOI] [PubMed] [Google Scholar]
- 21.Wang HW, Xiang Q, Li CQ, et al. Traumatic vertebral fractures with concomitant fractures of the first rib. Orthop Surg 2013; 5:100–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lu MS, Huang YK, Liu YH, et al. Delayed pneumothorax complicating minor rib fracture after chest trauma. Am J Emerg Med 2008; 26:551–554. [DOI] [PubMed] [Google Scholar]
- 23.Kerr-Valentic MA, Arthur M, Mullins RJ, et al. Rib fracture pain and disability: can we do better? J Trauma 2003; 54:1058–1063. [DOI] [PubMed] [Google Scholar]
- 24.Kattail D, Furlan JC, Fehlings MG. Epidemiology and clinical outcomes of acute spine trauma and spinal cord injury: experience from a specialized spine trauma center in Canada in comparison with a large national registry. J Trauma 2009; 67:936–943. [DOI] [PubMed] [Google Scholar]
- 25.Couris CM, Guilcher SJ, Munce SE, et al. Characteristics of adults with incident traumatic spinal cord injury in Ontario, Canada. Spinal Cord 2010; 48:39–44. [DOI] [PubMed] [Google Scholar]