

Abstract
Background:
Dexmedetomidine hydrochloride (Dex) is a useful adjuvant for general anesthesia. The aim was to evaluate the effects of Dex infusion during living donors liver transplantation (LDLT) on the general anesthetic requirements, hemodynamics, oxygen consumption (VO2), and CO2 production (VCO2).
Materials and Methods:
Forty LDLT recipients were allocated randomly to receive either Dex (0.2-0.7 μg/kg/h) or placebo (control [C]). Patient state index (PSI), SEDLine monitored anesthesia depth (25-50) with desflurane (Des) % and fentanyl altered accordingly. Transesophageal Doppler (TED), invasive mean arterial blood pressure (MAP) and heart rate (HR) were monitoring any Dex side effects and altering infusion rate accordingly; TED was used for fluid optimization. Metabolic gas monitoring (VO2, VCO2) and Des consumption were recorded.
Results:
Dex reduced Des and fentanyl consumption versus C (120.0 ± 30.2 vs. 248.0 ± 38.8) ml, (440.0 ± 195.74 vs. 1300.0 ± 32) μg, respectively (P < 0.01). Dex was delivered for 11.35 ± 2.45 h with comparable HR, MAP, and TED variables versus C and with similar mean noradrenaline support (5.63 ± 2.44 vs. 5.83 ± 2.57 mg, P = 0.81). VO2 was reduced with Dex vs. C during anhepatic, 30 min postreperfusion and end of surgery (193.2 ± 26.78 vs. 239 ± 14.93) (172.1 ± 28.14 vs. 202.7 ± 18.03) and (199.7 ± 26.63 vs. 283.8 ± 14.83) ml/min/m2 respectively (P < 0.01). VCO2 was also reduced with Dex versus C during the same periods (195.2 ± 46.41 vs. 216.7 ± 29.90, P = 0.09), (210.6 ± 60.71 vs. 253.9 ± 32.51, P = 0.01), and (158.7 ± 49.96 vs. 209.7 ± 16.78, P < 0.01), ml/min/m2 respectively.
Conclusion:
TED and PSI guided Dex infusion helped to reduce Des and fentanyl consumption as well as VO2 and VCO2 at a lower cost with no adverse effects on hemodynamics.
Keywords: Adult living donor liver transplantation, dexmedetomidine, intraoperative, recipient
Introduction
Adult living donor liver transplantation (ALDLT) is long major operations that is, characterized by hemodynamic instability and requires high anesthetic drugs consumption including opioids and inhalational anesthetics. Trying to provide hemodynamic stability and decrease the anesthetic requirement may have a good impact on the newly transplanted graft function and on the patient recovery besides the decrease in the total anesthetic cost. During liver transplantation, oxygen consumption decreased rapidly by 25% when the blood supply to the native liver was interrupted. After the anhepatic period, there was a sharp increase of oxygen consumption with successful reperfusion of the allograft. Carbon dioxide production fell by 14% and returned to preanhepatic values after successful declamping.[1] During ALDLT, reperfusion of the donor graft is associated with rapid physiological and metabolic changes; these include an increase in cardiac output, central venous pressure, and a decrease in systemic vascular resistance (SVR) which when severe constitute the postreperfusion syndrome. Alterations in metabolic rate also occur as the graft is perfused with oxygenated blood and becomes metabolically active. It has been previously shown that the increase in whole body oxygen consumption occurs after reperfusion which may reflect oxygen uptake by the graft; however, there are no detailed studies on the alterations in gas exchange which accompany this increase or their relationship to hemodynamic changes.[2] Dexmedetomidine (Dex) was approved in the USA in 1999 for sedation and analgesia in the Intensive Care Unit (ICU). Compared with clonidine, Dex is about 8 times more specific for α2-adrenoreceptors with a α2:α1 selectivity ratio of 1600:1. These unique properties of Dex makes it a α2-adrenoreceptor full agonist agent with sedative and anxiolytic effects.[3] The short half-life of Dex makes it particularly suitable for intravenous (IV) infusion. Administration of IV Dex produces an anesthetic – sparing effect with 25% reduction of maintenance concentrations of isoflurane in patients undergoing hysterectomy[4,5] and 17% reduction in sevoflurane requirements for maintenance of anesthesia in elderly patients.[6] In addition, the use of Dex produces intraoperative and postoperative opioid-sparing effect. Administration of Dex at dose of 0.4 μg/kg in patients undergoing laparoscopic tubal ligation caused 33% decrease in morphine use postoperatively.[7] We, therefore, designed this study to evaluate the effects of Dex infusion during ALDLT on the general anesthetic requirements (primary outcome), hemodynamics, VO2, VCO2, and cost (secondary outcome).
Materials and Methods
Ethics Committee approval (0076/2014) was provided by the Menoufia University National Liver Institute Institutional Review Board, (Chairperson Professor Mohamed EL-Guindi) (on January 01, 2014) Pan African Clinical Trial Registry of South Africa (PACTR201408000872245) (www.pactr.org) and consent approvals, 40 patients, aged 18-60 years, with model for end-stage liver disease (MELD) score 12-20, living donor liver transplant recipients with no severe hemodynamic instability, normoxia, normothermia, and no major intraoperative events. We excluded patients older than 60 years, those with a history of psychiatric/neurological illness, cardiovascular disease, hypertensive patients, and morbid obese patients, with known allergic reaction to any of the study medication and with significant laboratory abnormalities. Unwilling to participate in the study. The consenting patients were randomly allocated into two equal groups using a simple random technique (closed envelopes), Dex group (group D) and control group (group C). After arrival in the operating room, preoxygenation using O2/air mixture (FIO2= 0.8) for 3-5 min, general anesthesia was induced with IV propofol 2 mg/kg, fentanyl 1 μg/kg and rocuronium 0.6-0.9 mg/kg followed by endotracheal intubation. Anesthesia was maintained after intubation with (desflurane [Des]) (Baxter, Erlangen, Germany) in O2/air mixture (FIO2= 0.4) to keep the patient state index (PSI™) value between 25 and 50 (SEDLine Brain Function Monitor (Masimo, Irvine, CA, USA) to monitor depth of anesthesia. Mechanical ventilation was performed in all patients using a semi-closed system (Datex Omeda, GE, USA), adjusted to keep SaO2>95% and end-tidal CO2 between 35 and 40 mmHg. Rocuronium administered to provide a balanced general anesthesia according to nerve stimulator results and incremental doses of fentanyl are used. 22 gauge into the left radial artery after performing modified Allen's test for continuous blood pressure (BP) monitoring and arterial blood gas analysis. By the aid of ultrasound 7 Fr triple central venous catheter was passed through the right internal jugular vein. A rapid infusion system (Level 1® H-1200 Fast Flow Fluid Warmer with Integrated Air Detector/Clamp, Smith Medical Com, USA) was used when needed to allow rapid transfusion of warmed fluids and blood (37-38°C) at rates of up to 1500 ml/min multiple (at least 3) wide IV lines (14 gauge) were inserted, and an indwelling bladder catheter was used for urine collection. All patients received piperacillin sodium 4 g, tazobactam 500 mg, and metronidazole 0.5 g every 8 h along the course of operation. Intermittent pneumatic compression (Kendall Company, Tyco, USA) were applied to both lower limbs to prevent postoperative deep venous thrombosis. The patients were covered by air forced warm blankets (Model 750, Bair Hugger Temperature Management Unit, SMA MISR, Arizant Healthcare Inc., USA) to maintain normothermia. A lubricated nasogastric tube was gently inserted via the nose to decompress the patient's stomach and to optimize the surgical field exposure. Transesophageal Doppler (TED) was inserted via oral airway and used to monitor and measure hemodynamic variables. The patient's position was carefully checked before draping to ensure that there were no pressure points and that IV lines were not occluded. The patient's arms were well padded and generally placed along the body or with the least amount of abduction possible using jelly pads. Warmed infusions were used all through the procedure; blood has been warmed using blood warmer (Ranger Blood/Fluid Warming Unit, Arizant Healthcare Inc., Lifecare, USA). The fluid regimen consisted of Ringer's acetate solutions at 6 mL/kg/h albumin 5% was infused only to treat hypoalbuminemia related to ascites. Packed red blood cells were transfused to maintain hematocrit above 25%. Other blood products were administered under the guidance of rotational thromboelastometry. Boluses of colloid were administered, guided by an algorithm depending on the Doppler estimations of stroke volume (SV) and corrected flow time (FTc). At the end of surgery as a protocol, the patient was monitored on sedation in ICU for about 6 h before extubation if hemodynamics were stable.
The protocol of Dex infusion: Pharmacy Department supplied the infusions to the Anesthesia Department prior to the planned surgery. Both anesthesia provider and the accessors were blind to the content of the infusion. Sealed opaque envelopes were only opened by the pharmacist to allocate the patient to his group.
The 1st group (control) received saline boluses and infusion as placebo. The 2nd group (Dex group) received: Dex hydrochloride for injection (100 mcg/mL in a 2 mL glass vial, Hospira Healthcare Company for pharmaceutical and chemical industries.) a continuous infusion of dexmedetomidine starting by 0.5 mic/kg/h (0.2-0.7 mic/kg/h) depending on heart rate (HR), BP, and SEDLine value changes. Started with the induction of anesthesia by continuous infusion without bolus dose with a syringe pump over the entire operation period until the end of skin wound closure.
Measurements
All patients had full laboratory data as a baseline before the operation, Intraoperatively, HR (beat/min). Mean arterial blood pressure (MAP) (mmHg). TED parameters were recorded until the end of surgery included: Cardiac output (CO) (L/min). SV (ml). SVR (dyns.s/cm5) FTc (ms). Moreover, metabolic gas monitoring; VO2, VCO2 were performed using a portable metabolic cart system (Deltatrac, Datex/Instrumentarium, Helsinki, Finland [disposable Spirometry tube GE Healthcare Finland Helsinki]) as follows: After induction of anesthesia and before surgical incision (baseline) (T0), 5 min before reperfusion (anhepatic phase) (T1), 60 min after reperfusion (T2), and at the end of operation (T3). Time of operation (h) volatile anesthetic (Des) consumption (ml). The dosage of used opioids, for example, fentanyl (μg). Final core temperature (°C). Total costs. Red blood cell transfusion requirements (units). Any other side effects and laboratory data were recorded.
Statistical procedure
The data were assessed for normality using the Kolmogorov–Smirnov test. Data are described as the mean and standard deviation (SD), with 95% confidence intervals where appropriate. SPSS version 15 (SPSS Inc., Chicago, IL, USA) was used to conduct all the statistical analyses. Comparisons were carried out between the two studied groups using the independent t-test. A P < 0.05 was considered statistically significant Box and Whiskers graph were done. Chi-square test and Fisher exact test were used to measure the association between qualitative variables.
Sample size and power of the study: In the present study, α was set to 0.05 (priori), and maximum β accepted = 10% with a minimum power of the study of 90%. Twenty patients per group was calculated to be sufficient as the primary outcome of this RCT was anesthetic consumption ml between experimental group (Dex group: 0.2-0.7 mic/kg/h) and control group, no drug in saline infusion with a mean difference of (32 ml) and SD of (±30 ml),[8] two-tailed analysis will be adopted. Calculation of sample size was done using (IBM SPSS sample power) software and was also confirmed using Lenth Java applets for power and sample size.[9]
Results
Forty living donor liver transplantation recipients were enrolled in this study, 20 patients in each group. Patient characteristics in Dex (D group) versus control (C group) were comparable regarding mean age, weight, and body mass index. The male/female ratio was 16/4 in D group and 14/6 in C group [Table 1]. Mean model of end-stage liver disease (MELD) values were (14.3 ± 1.13) in D group versus (14.20 ± 1.44) in C group and there were no statistically significant differences between both groups, as presented in Table 1. Dex reduced Des and fentanyl consumption versus C (120.0 ± 30.2 vs. 248.0 ± 38.8) ml, (440.0 ± 195.74 vs. 1300.0 ± 32) μg, respectively (P < 0.01). Dex was delivered for 11.35 ± 2.45 h with comparable HR, MABP and TED variables vs. C and with similar mean noradrenaline support (5.63 ± 2.44 vs. 5.83 ± 2.57 mg, P = 0.80) [Tables 2 and 3 and Figure 1]. VO2 was reduced with Dex vs. C during anhepatic (T1), 30 min post reperfusion (T2) and end of surgery (T3) (193.2 ± 26.78 vs. 239 ± 14.93) (172.1 ± 28.14 vs. 202.7 ± 18.03) and (199.7 ± 26.63 vs. 283.8 ± 14.83) ml/min/m2 respectively (P = 0.00). VCO2 was also reduced with Dex versus C during the same periods (195.2 ± 24.48 vs. 216.60 ± 30, P = 0.02), (210.6 ± 60.71 vs. 253.9 ± 37.63, P = 0.02), and (158.7 ± 49.96 vs. 209.7 ±30.65, P = 0.00), ml/min/m2 respectively Figures 2 and 3. Comparable operative times and graft weights with Des vs., C (11.35 ± 2.45 vs. 12.0 ± 2.38 h, P = 0.40), (785.0 ± 110.14 vs. 775.0 ± 137.66 g, P = 0.80), respectively. Total Dex consumed 205 ± 15.39 μg. Dex reduced the total anesthetic cost (654.17 ± 116.21 vs. 807.22 ± 99.01, Egyptian pounds, LE, P < 0.01).
Table 1.
Demographic data in the two study groups
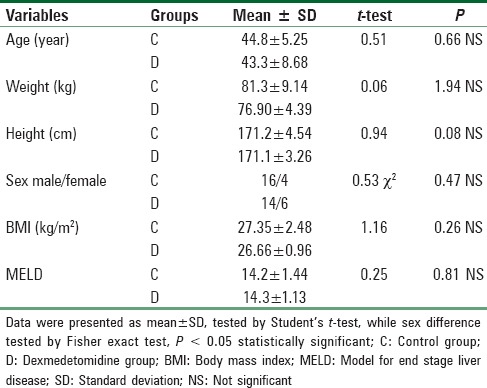
Table 2.
Operative data and anesthetic requirement
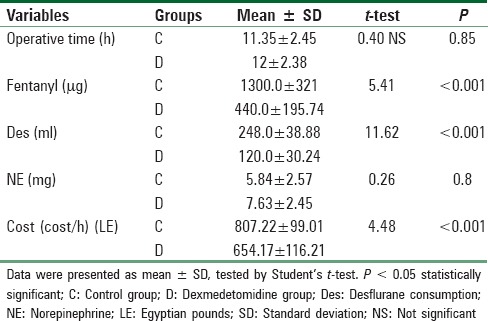
Table 3.
HR (beat/min), MAP (mmHg), COP (L/min), and FTc (ms) in both groups
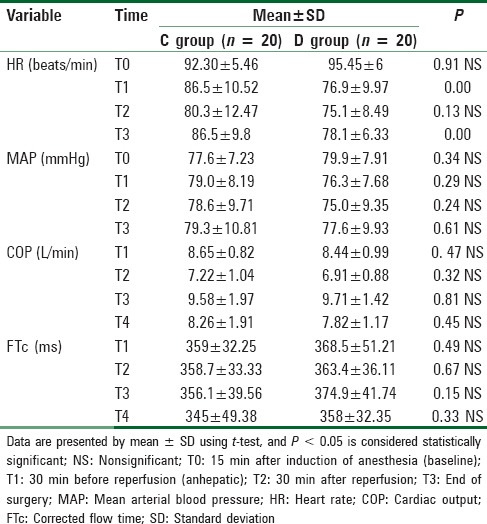
Figure 1.
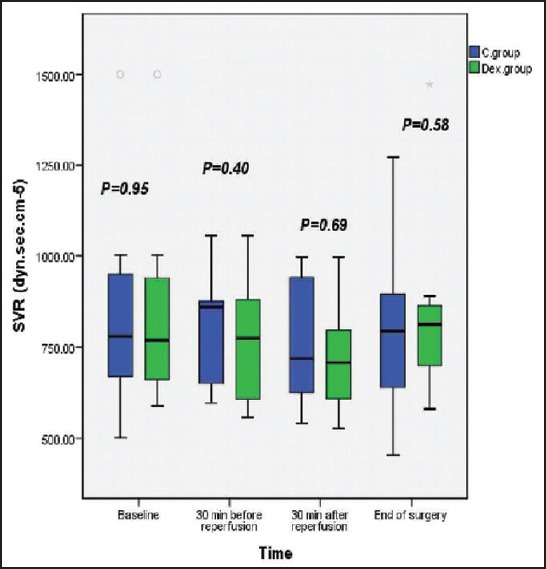
Box and whiskers graph of systemic vascular resistance (dyns.s/cm5) in the two studied groups; C group (control group); D group (dexmedetomidine group), significantP< 0.05
Figure 2.
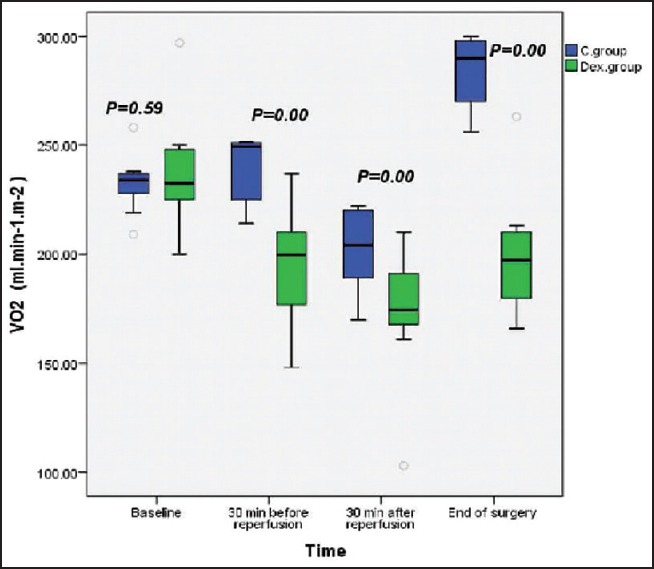
Box and whiskers graph of oxygen consumption VO2 (ml/min/m2) in the two studied groups; C group (control group); D group (dexmedetomidine group), significantP< 0.05
Figure 3.
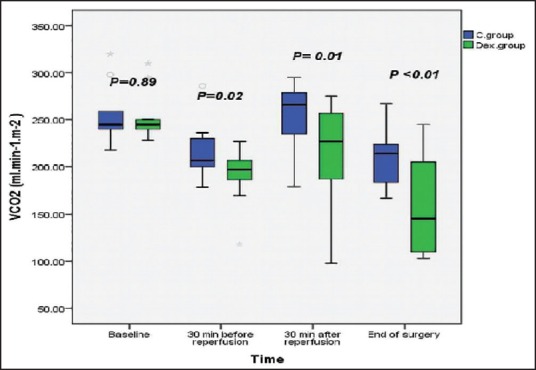
Box and whiskers graph of carbon dioxide consumption VCO2 (ml/min/m2) in the two studied groups; C group (control group); D group (dexmedetomidine group), significantP< 0.05
Discussion
The major observation in our study was that Dex infusion as an adjuvant in general anesthesia causes decreased requirement of Des and fentanyl in patients undergoing ALDLT without compromising adequate depth of anesthesia, Dex offers a unique ability of providing both sedation and analgesia without respiratory depression thus it has anesthetic-sparing property.[10] Patel et al. concluded that Dex continuous infusion reduced sevoflurane requirements during general anesthesia.[11] Anesthetic-sparing effect of Dex in our study is consistent with earlier studies. A study done on patients undergoing hysterectomy showed a 30% reduction of maintenance concentration of isoflurane.[5] Similarly, a reduction in 35-50% in isoflurane concentration with a low or high dose of Dex was found in a study on healthy human volunteers.[12] The results of our study are consistent with that of the study done by Fragen, et al.[6] Dex by its sympatholytic action decreases HR and BP, thus assessing the depth of anesthesia by hemodynamic parameters would be unreliable in evaluating its effect on requirement of inhalational agent, so we used SEDLine brain function monitor to altered Des accordingly. Use of Dex produces intra-operative and postoperative opioids-sparing effect. Dex by its sympatholytic action attenuates sympathoadrenal response to tracheal intubation.[13] In patients undergoing laparoscopic tubal ligation, a 33% decrease in morphine use postoperatively was observed when Dex was used at a dose of 0.4 mcg/kg.[7] Dex has a specific analgesic effect and provides visceral pain relief.[14] In morbidly obese, Dex produces a greater decrease in sympathovagal balance intra-operatively than fentanyl along with better postoperative analgesia.[15]
Dex, when used as sole substitute for remifentanil in ambulatory gynecologic laparoscopic surgery, provides better perioperative hemodynamic stability, and post-operative analgesia.[16] Dex provides similar intra-operative hemodynamic response and better postoperative analgesia compared to remifentanil in patients undergoing supratentorial craniotomy.[17] Ghodki et al.[18] concluded that Dex is an effective anesthetic adjuvant that can be safely used in laparoscopy without the fear of awareness. Dex infusion prevents postoperative shivering in patients undergoing gynecologic laparoscopic surgery.[19] Our study demonstrated that Dex decreased mean HR and MAP as Dex attenuates various stress responses during surgery and maintains the hemodynamic stability, when used as an adjuvant in general anesthesia. Dex increases the hemodynamic stability by altering the stress-induced sympathoadrenal responses to intubation during surgery and during emergence from anesthesia.[20,21] Jaakola et al. in their study concluded that Dex attenuates the increase in HR and BP during intubation.[22] Dex, the ideal drug for attenuating the pressor response.[23,24] Dex improves intra- and post-operative hemodynamic stability during laparoscopic surgery without prolongation of recovery.[25] Khetarpal et al. described the management of patient of pheochromocytoma in which the combination of Dex and sevoflurane was very effective to control hypertensive surges in the patients who are adequately prepared preoperatively.[26] The oxygen available to the tissues at every stage of the liver transplantation is dependent on the CO and the arterial oxygen content (CaO2). Bleeding, vascular clamping, and hypotension are some of the factors that may adversely affect the oxygen availability with undesirable consequences on graft viability in orthotopic liver transplantation.[27] Abnormal changes in total oxygen consumption are considered as an early indicator for the occurrence of primary nonfunction of the newly transplanted liver.[28] Attempts to correlate changes in oxygen uptake with the function of the newly implanted liver have also had contradictory results. Our results concluded that Dex decreased intraoperative VO2 and VCO2. Dex able to decrease oxygen consumption in the intraoperative period (up to 8%) and in the postoperative period (up to 17%) in patients undergoing plastic surgery procedures under general anesthesia.[29] Previous studies have shown that hemodynamic stabilization by the application of α2 adrenoceptor agonists in the Perioperative period leads to a reduction in perioperative myocardial ischemia episodes.[30] Dex possesses neuroprotective properties in various experimental models of cerebral ischemia and attenuated hypoxic-ischemic brain injury in developing brains, highly susceptible to neuronal damage.[31] Moreover, a significant improvement in functional neurological outcomes after a brain injury was demonstrated.[31] The exact mechanisms of neuroprotection are not clear, but catecholamine pathways play an important role. α2 adrenoceptors modulate neurotransmitter release in the central and peripheral sympathetic nervous system, thus offering a possible explanation for the neuroprotective properties of Dex. Kucuk et al. results suggest that Dex has beneficial effects on liver ischemia/reperfusion.[32] Perioperative stress associated with surgery and anesthesia evokes an endocrine response that includes stimulation of the sympathetic nervous system.[33] This increases circulating plasma adrenaline and noradrenaline concentrations with consequent increases in arterial pressure, HR, and oxygen consumption.[33,34] controlling this perioperative stress response is an important goal of modern anesthesia.[35] Dex, decreases central sympathetic outflow and modify intraoperative cardiovascular and endocrine responses favorably to surgical stimuli and laryngoscopy.[36,37] The reduction in tachycardia, hypertension, sympathetic activity, plasma catecholamine concentration results in decreased whole body metabolism and consequently total body oxygen consumption may be of benefit in patients at risk of developing inadequate CO or myocardial ischemia.[34,35] These combined effects may contribute to the reduction observed in VO2 and VCO2. The analgesic effects of Dex and the indirect effects of sedation and neuromuscular block might account in part for the reduction in VO2. It has been demonstrated that effective analgesia in the postoperative period can decrease VO2 by up to 7-8%.[38]
One of the limitation to our study was not measuring the changes in plasma concentration of Dex, which if undertaken would have helped to establish the precise correlation between the Dex doses and Des requirements. From this study, TED and PSI guided Dex infusion helped to reduce Des and fentanyl consumption as well as VO2 and VCO2 at a lower cost with no adverse effects on intraoperative hemodynamics. This observed effect on oxygen consumption and its impact on the newly transplanted graft function need to be studied further.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Svensson KL, Persson H, Henriksson BA, Karlberg I, Sonander H, Lundholm K, et al. Whole body gas exchange: Amino acid and lactate clearance as indicators of initial and early allograft viability in liver transplantation. Surgery. 1989;105:472–80. [PubMed] [Google Scholar]
- 2.Walsh TS, Hopton P, Garden OJ, Lee A. Effect of graft reperfusion on haemodynamics and gas exchange during liver transplantation. Br J Anesth. 1998;81:311–6. doi: 10.1093/bja/81.3.311. [DOI] [PubMed] [Google Scholar]
- 3.Kamibayashi T, Maze M. Clinical uses of alpha2 -adrenergic agonists. Anesthesiology. 2000;93:1345–9. doi: 10.1097/00000542-200011000-00030. [DOI] [PubMed] [Google Scholar]
- 4.Aantaa R, Kanto J, Scheinin M, Kallio A, Scheinin H. Dexmedetomidine, an alpha 2-adrenoceptor agonist, reduces anesthetic requirements for patients undergoing minor gynecologic surgery. Anesthesiology. 1990;73:230–5. doi: 10.1097/00000542-199008000-00007. [DOI] [PubMed] [Google Scholar]
- 5.Aho M, Lehtinen AM, Erkola O, Kallio A, Korttila K. The effect of intravenously administered dexmedetomidine on perioperative hemodynamics and isoflurane requirements in patients undergoing abdominal hysterectomy. Anesthesiology. 1991;74:997–1002. doi: 10.1097/00000542-199106000-00005. [DOI] [PubMed] [Google Scholar]
- 6.Fragen RJ, Fitzgerald PC. Effect of dexmedetomidine on the minimum alveolar concentration (MAC) of sevoflurane in adults age 55 to 70 years. J Clin Anesth. 1999;11:466–70. doi: 10.1016/s0952-8180(99)00081-1. [DOI] [PubMed] [Google Scholar]
- 7.Aho MS, Erkola OA, Scheinin H, Lehtinen AM, Korttila KT. Effect of intravenously administered dexmedetomidine on pain after laparoscopic tubal ligation. Anesth Analg. 1991;73:112–8. doi: 10.1213/00000539-199108000-00002. [DOI] [PubMed] [Google Scholar]
- 8.Birkett MA, Day SJ. Internal pilot studies for estimating sample size. Stat Med. 1994;13:2455–63. doi: 10.1002/sim.4780132309. [DOI] [PubMed] [Google Scholar]
- 9.Lenth RV. Java Applets for Power and Sample Size [Computer Software] 2006-9. [Last retrieved on 2013 Jan 01]. Available from: http://www.stat.uiowa.edu/~rlenth/Power .
- 10.Afonso J, Reis F. Dexmedetomidine: Current role in anesthesia and intensive care. Rev Bras Anestesiol. 2012;62:118–33. doi: 10.1016/S0034-7094(12)70110-1. [DOI] [PubMed] [Google Scholar]
- 11.Patel CR, Engineer SR, Shah BJ, Madhu S. The effect of dexmedetomidine continuous infusion as an adjuvant to general anesthesia on sevoflurane requirements: A study based on entropy analysis. J Anesthesiol Clin Pharmacol. 2013;29:318–22. doi: 10.4103/0970-9185.117066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Khan ZP, Munday IT, Jones RM, Thornton C, Mant TG, Amin D. Effects of dexmedetomidine on isoflurane requirements in healthy volunteers 1: Pharmacodynamic and pharmacokinetic interactions. Br J Anesth. 1999;83:372–80. doi: 10.1093/bja/83.3.372. [DOI] [PubMed] [Google Scholar]
- 13.Keniya VM, Ladi S, Naphade R. Dexmedetomidine attenuates sympathoadrenal response to tracheal intubation and reduces perioperative anesthetic requirement. Indian J Anesth. 2011;55:352–7. doi: 10.4103/0019-5049.84846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cortinez LI, Hsu YW, Sum-Ping ST, Young C, Keifer JC, Macleod D, et al. Dexmedetomidine pharmacodynamics: Part II: Crossover comparison of the analgesic effect of dexmedetomidine and remifentanil in healthy volunteers. Anesthesiology. 2004;101:1077–83. doi: 10.1097/00000542-200411000-00006. [DOI] [PubMed] [Google Scholar]
- 15.Feld JM, Hoffman WE, Stechert MM, Hoffman IW, Ananda RC. Fentanyl or dexmedetomidine combined with desflurane for bariatric surgery. J Clin Anesth. 2006;18:24–8. doi: 10.1016/j.jclinane.2005.05.009. [DOI] [PubMed] [Google Scholar]
- 16.Salman N, Uzun S, Coskun F, Salman MA, Salman AE, Aypar U. Dexmedetomidine as a substitute for remifentanil in ambulatory gynecologic laparoscopic surgery. Saudi Med J. 2009;30:77–81. [PubMed] [Google Scholar]
- 17.Turgut N, Turkmen A, Ali A, Altan A. Remifentanil-propofol vs dexmedetomidine-propofol – Anesthesia for supratentorial craniotomy. Middle East J Anesthesiol. 2009;20:63–70. [PubMed] [Google Scholar]
- 18.Ghodki PS, Thombre S, Sardesai SP, Harnagle KD. Dexmedetomidine as an anesthetic adjuvant in laparoscopic surgery: An observational study using entropy monitoring. J Anesthesiol Clin Pharmacol. 2012;28:334–8. doi: 10.4103/0970-9185.98329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Karaman S, Gunusen I, Ceylan MA, Karaman Y, Etin EN, Derbent A, et al. Dexmedetomidine infusion prevents postoperative shivering in patients undergoing gynecologic laparoscopic surgery. Turk J Med Sci. 2013;43:232–7. [Google Scholar]
- 20.Scheinin B, Lindgren L, Randell T, Scheinin H, Scheinin M. Dexmedetomidine attenuates sympathoadrenal responses to tracheal intubation and reduces the need for thiopentone and peroperative fentanyl. Br J Anesth. 1992;68:126–31. doi: 10.1093/bja/68.2.126. [DOI] [PubMed] [Google Scholar]
- 21.Patel CR, Engineer SR, Shah BJ, Madhu S. Effect of intravenous infusion of dexmedetomidine on perioperative haemodynamic changes and postoperative recovery: A study with entropy analysis. Indian J Anesth. 2012;56:542–6. doi: 10.4103/0019-5049.104571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jaakola ML, Ali-Melkkilä T, Kanto J, Kallio A, Scheinin H, Scheinin M. Dexmedetomidine reduces intraocular pressure, intubation responses and anesthetic requirements in patients undergoing ophthalmic surgery. Br J Anesth. 1992;68:570–5. doi: 10.1093/bja/68.6.570. [DOI] [PubMed] [Google Scholar]
- 23.Sulaiman S, Karthekeyan RB, Vakamudi M, Sundar AS, Ravullapalli H, Gandham R. The effects of dexmedetomidine on attenuation of stress response to endotracheal intubation patients undergoing elective off-pump coronary artery bypass grafting. Ann Card Anaeth. 2012;15:39–43. doi: 10.4103/0971-9784.91480. [DOI] [PubMed] [Google Scholar]
- 24.Saraf R, Jha M, Kumar SS, Damani K, Bokil S, Galante D. Dexmedetomidine, the ideal drug for attenuating the pressor response. Pediatr Anesth Crit Care J. 2013;1:78–86. [Google Scholar]
- 25.Bindu B, Pasupuleti S, Gowd UP, Gorre V, Murthy RR, Laxmi MB. A double blind, randomized, controlled trial to study the effect of dexmedetomidine on hemodynamic and recovery responses during tracheal extubation. J Anesthesiol Clin Pharmacol. 2013;29:162–7. doi: 10.4103/0970-9185.111665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Khetarpal M, Yadav M, Kulkarni D, Gopinath R. Role of dexmedetomidine and sevoflurane in the intraoperative management of patient undergoing resection of phaeochromocytoma. Indian J Anesth. 2014;58:496–7. doi: 10.4103/0019-5049.139028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kostopanagiotou G, Smyrniotis V, Theodoraki K, Skalkidis Y, Heaton N, Potter D. Oxygen availability during orthotopic liver transplantation. Liver Transpl. 2003;9:1216–21. doi: 10.1053/jlts.2003.50241. [DOI] [PubMed] [Google Scholar]
- 28.Steltzer H, Hiesmayr M, Tüchy G, Zimpfer M. Perioperative liver graft function: The role of oxygen transport and utilization. Anesth Analg. 1993;76:574–9. doi: 10.1213/00000539-199303000-00022. [DOI] [PubMed] [Google Scholar]
- 29.Taittonen MT, Kirvelä OA, Aantaa R, Kanto JH. Effect of clonidine and dexmedetomidine premedication on perioperative oxygen consumption and haemodynamic state. Br J Anesth. 1997;78:400–6. doi: 10.1093/bja/78.4.400. [DOI] [PubMed] [Google Scholar]
- 30.Wallace AW, Galindez D, Salahieh A, Layug EL, Lazo EA, Haratonik KA, et al. Effect of clonidine on cardiovascular morbidity and mortality after noncardiac surgery. Anesthesiology. 2004;101:284–93. doi: 10.1097/00000542-200408000-00007. [DOI] [PubMed] [Google Scholar]
- 31.Ma D, Hossain M, Rajakumaraswamy N, Arshad M, Sanders RD, Franks NP, et al. Dexmedetomidine produces its neuroprotective effect via the alpha 2A-adrenoceptor subtype. Eur J Pharmacol. 2004;502:87–97. doi: 10.1016/j.ejphar.2004.08.044. [DOI] [PubMed] [Google Scholar]
- 32.Kucuk A, Yaylak F, Cavunt-Bayraktar A, Tosun M, Arslan M, Comu FM, et al. The protective effects of dexmedetomidine on hepatic ischemia reperfusion injury. Bratisl Lek Listy. 2014;115:680–4. doi: 10.4149/bll_2014_132. [DOI] [PubMed] [Google Scholar]
- 33.Udelsman R, Norton JA, Jelenich SE, Goldstein DS, Linehan WM, Loriaux DL, et al. Responses of the hypothalamic-pituitary-adrenal and renin-angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J Clin Endocrinol Metab. 1987;64:986–94. doi: 10.1210/jcem-64-5-986. [DOI] [PubMed] [Google Scholar]
- 34.Ensinger H, Weichel T, Lindner KH, Grünert A, Ahnefeld FW. Effects of norepinephrine, epinephrine, and dopamine infusions on oxygen consumption in volunteers. Crit Care Med. 1993;21:1502–8. doi: 10.1097/00003246-199310000-00018. [DOI] [PubMed] [Google Scholar]
- 35.Roizen MF. Should we all have a sympathectomy at birth? Or at least preoperatively. Anesthesiology. 1988;68:482–4. [PubMed] [Google Scholar]
- 36.Aho M, Erkola O, Kallio A, Scheinin H, Korttila K. Dexmedetomidine infusion for maintenance of anesthesia in patients undergoing abdominal hysterectomy. Anesth Analg. 1992;75:940–6. [PubMed] [Google Scholar]
- 37.Bonnet F, Boico O, Rostaing S, Loriferne JF, Saada M. Clonidine-induced analgesia in postoperative patients: Epidural versus intramuscular administration. Anesthesiology. 1990;72:423–7. doi: 10.1097/00000542-199003000-00004. [DOI] [PubMed] [Google Scholar]
- 38.Muneyuki M, Ueda Y, Urabe N, Takeshita H, Inamoto A. Postoperative pain relief and respiratory function in man: Comparison between intermittent intravenous injections of eperidine and continuous lumbar epidural analgesia. Anesthesiology. 1968;29:304–13. doi: 10.1097/00000542-196803000-00015. [DOI] [PubMed] [Google Scholar]